










Serviços Personalizados
Journal

Artigo
 texto em
texto em  Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Curriculum ScienTI
Curriculum ScienTILinks relacionados
Compartilhar

 Permalink
PermalinkOdontoestomatología
versão impressa ISSN 0797-0374versão On-line ISSN 1688-9339
Odontoestomatología vol.24 no.39 Montevideo jun. 2022 Epub 01-Jun-2022
https://doi.org/10.22592/ode2022n39e310
Update
Radiation-related caries treatment: a literature review
1
 http://orcid.org/0000-0002-9243-381X
http://orcid.org/0000-0002-9243-381X
1
http://orcid.org/0000-0003-0280-4259
1
http://orcid.org/0000-0002-3470-5290
1Programa de Posgraduación en Odontología, Universidad de Brasília, Brasília, DF. 1. drapinedamancia@gmail.com
Radiation-related caries are a frequent late complication caused by the direct and indirect effects of head and neck cancer radiotherapy. This study aimed to review and analyze the literature on managing radiation-related caries, restorative materials, treatment failures, and treatment protocols. A search was conducted in Pubmed, Lilacs, and Web of Science by three independent reviewers, and inclusion and exclusion criteria were used for paper selection. According to clinical studies and literature reviews, the most used materials are conventional glass-ionomer cement, resin-modified glass-ionomer cement, and composite resin with fluoride applications. More studies are needed to determine the best treatment, including cavity preparation technique and restorative material with better results. We suggest conducting studies comparing various adhesive systems, fluoride concentrations, and root dentin restorations.
Keywords: radiotherapy; dental caries; head and neck cancer
Caries relacionada a radiación es una complicación tardía frecuente de la radioterapia de cáncer de cabeza y cuello, ocasionada por efectos directos e indirectos de la radioterapia. El objetivo del presente trabajo es realizar una revisión y analizar literatura sobre el manejo de caries relacionada a radiación, materiales usados, fallas en el tratamiento y protocolo con mejores resultados; tres revisores independientes realizaron una búsqueda en diferentes bases de datos: PubMed, Lilacs y Web Of Science, determinando criterios de inclusión y exclusión para la selección. Estudios clínicos y revisiones indicaron que los materiales más usados son cemento ionómero de vidrio convencional, cemento ionómero de vidrio modificado con resina y resina compuesta con aplicaciones de flúor. Son necesarios más estudios para definir el mejor tratamiento que incluya técnica de preparación de la cavidad y material restaurador con mejores resultados. Se recomienda realizar estudios comparando diferentes sistemas adhesivos, concentraciones de flúor y restauraciones en dentina radicular.
Palabras clave: Radioterapia; Caries dental; Cáncer de cabeza y cuello
Cárie relacionada à radiação é uma complicação tardia frequente da radioterapia de câncer de cabeça e pescoço, ocasionada por efeitos diretos e indiretos da radioterapia. O objetivo do presente trabalho é realizar uma revisão e analisar literatura sobre o tratamento de cárie relacionada à radiação, materiais usados, falhas no tratamento e manejo com melhores resultados; foi realizada uma busca em diferentes bases de dados: PubMed, Lilacs e Web Of Science, por três revisores independentes, usando critérios de inclusão e exclusão. Estudos clínicos e revisões de literatura indicam que os materiais mais usados são cimento de ionômero de vidro convencional, cimento de ionômero de vidro modificado com resina e resina composta com aplicações de flúor. Mais estudos são necessários para definir o melhor tratamento que inclua a técnica de preparo cavitário e material restaurador com melhores resultados. Recomenda-se a realização de estudos comparando diferentes sistemas adesivos, concentrações de flúor e restaurações em dentina radicular.
Palavras chave: Radioterapia; Cárie dental; Câncer de cabeça e pescoço
Introduction
Radiotherapy for head and neck cancer is commonly associated with acute and late complications in healthy tissues located in the irradiated area. Common acute oral complications include mucositis, dysphagia, xerostomia, tender or painful soft tissues, and fungal infections.1,2 Other late complications include trismus, hyposalivation, osteoradionecrosis, changes in dental structures, and radiation-related caries.2-4
Radiation-related caries affect approximately 37% of irradiated head and neck cancer patients: it appears between 3 and 12 months after treatment is complete and is considered a late complication.5
Radiation-related caries is caused by a combination of the indirect effects of radiotherapy, such as damage to the salivary glands that modify the oral flora and reduce remineralization, damage to the temporomandibular joint and masticatory muscles causing trismus, and damage to the mucous membranes, which causes mucositis and limits adequate oral hygiene. There are also direct consequences on tooth structure,3,5 such as changes in microhardness, chemical composition, and micromorphology of enamel and dentin,6,7 predisposing patients to an increased risk of caries. It differs from conventional caries because it develops rapidly, is highly destructive, and is mostly painless.3,8-10 It mainly affects the root area near the cementoenamel junction4 and includes root-dentin caries.11
Restorative treatments for this type of caries are compromised by the harmful effect of radiotherapy on the bonding strength of the materials to enamel and dentin.12,13 This entails ineffective adhesion between the restoration and the dental substrate, mainly after high doses of radiotherapy.
Methods
An advanced search was conducted in PubMed, LILACS, and Web of Science databases using the following keywords in English, Spanish, and Portuguese: “radiation-related caries,” “radiotherapy,” “ionizing radiation,” “permanent dental restoration,” “composite resins,” “glass-ionomer cements,” “modified glass-ionomer cement,” “conventional glass-ionomer cement,” and “direct restoration.” The literature search was conducted from April to June 2021. The studies included fulfilled the following inclusion criteria: patients with head cancer treated with radiotherapy and treated for caries lesions, patients with any direct restoration with or without fluoride, clinical studies, randomized clinical trials, case-control, cohort, reviews without follow-up period restrictions. Exclusion criteria: reviews, letters, opinions, editorials, books, book chapters, in vitro or in situ studies, and other design studies different from those described in the inclusion criteria, and studies written in non-Latin script.
Development
We found the following studies on managing radiation-related caries: seven clinical studies, one case report, two systematic reviews, and one narrative review. One case report was excluded because it referred to indirect restorations, and one clinical study was excluded because it was written in non-Latin script. The studies included were in English, all available in full text and mainly in PubMed (Table 1).
Table 1: Main methodological data obtained from the studies on treating radiation-related caries
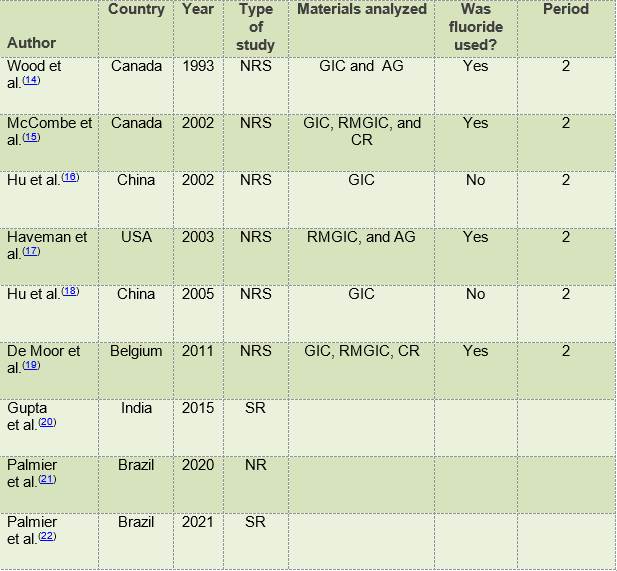
NRS: non-randomized study; SR: systematic review; NR: narrative review; GIC: glass-ionomer cement; AG: amalgam; RMGIC: resin-modified glass-ionomer cement, ART: atraumatic restorative treatment.
The oldest study was conducted in 1993 by Wood et al.14 They clinically compared VIC and AG restorations in the treatment of Class V caries in xerostomic patients with head and neck cancer. They divided the patients into fluoride users and non-fluoride users. They found that GIC failed, and AG restorations did not in patients using a slightly acidic sodium fluoride gel (pH 5.8) daily. In patients who stopped using topical fluoride as indicated, GIC restorations did not fail, but AG restorations did. The mean time to loss of restoration for both materials was 8.5 months.
In a 2002 study, Mc Comb et al.15 clinically compared GIC, RMGIC, and CR + conventional two-step adhesive system restorations to treat root caries in patients treated with radiotherapy for head and neck cancer. Each patient underwent a restoration with each of these materials. In addition, the daily use of a pH-neutral sodium fluoride gel in customized trays was indicated. Follow-up appointments were made after 6, 12, 18, and 24 months, and the restorations were examined for loss of material, marginal integrity, and recurrent caries at the restoration margin. No statistical differences were found between GIC and RMGIC, but statistical differences were found between these materials and CR in each recovery period. Reductions in recurrent caries in GIC and RMGIC restorations compared to CR were greater than 80% in patients using topical fluoride supplementation. The authors concluded that this clinical comparison provided evidence of the therapeutic efficacy of fluoride materials in reducing recurrent caries regardless of the material. They also concluded that fluoride-releasing restorative materials may offer a different clinical approach to the overall disease management of high-caries-risk patients.
In 2002, Hu et al. conducted a clinical study on 15 adult patients with radiation-related caries. They used two high-viscosity GICs in each patient to restore 146 caries lesions in exposed dentin and 93 in cementum areas. The restorations were monitored directly for two years to detect retention, secondary caries, anatomical shape, marginal integrity, marginal discoloration, and surface texture, and all patients received oral hygiene education. The authors found that placing highly viscous GIC in highcariesrisk patients seemed to prevent secondary caries, even when the restorations were subsequently lost.16
In 2003, Haveman et al. conducted a clinical study comparing RMGIC and AG restorations. They showed that fluoride-releasing materials could reduce caries around restorations in patients who do not use topical fluoride regularly.17
In 2005, Hu et al. conducted a clinical study restoring radiation-related caries at the root surface: GIC was placed in 72 conventional and 74 atraumatic restorative treatment (ART) preparations. Two professionals evaluated the restorations after 6, 12, and 24 months for retention, marginal defects and surface wear, and recurrent caries. They concluded that using hand instruments and the ART method was an equally effective alternative to conventional rotary instrumentation for cavity preparation. More extensive restorations had greater failure rates, usually due to loosening.18
In 2011, De Moor et al. evaluated the clinical performance of adhesive materials in Class V cavities in patients with head and neck cancer in terms of marginal adaptation, anatomical shape, and recurrent caries. Thirty-five adult patients with radiation-related caries with three or more root caries lesions in the same arch were selected. Each patient was treated with a restoration with GIC, RMGIC, CR + conventional 3-step adhesive system. Patients were instructed to use 1% neutral sodium fluoride gel in custom trays daily. After 6, 12, 18, and 24 months, the restorations were examined for loss of material, marginal integrity, and recurrent caries. The authors concluded that GIC is an optimal option to treat radiation-related root caries since its use is associated with protection against secondary caries (even after the loss of filling material). However, adaptation and disintegration are more marked in glass-ionomer cements than in composite resins. If glass ionomer cements fail, the defective restorative materials can be replaced, preferably preserving the remains of the glass-ionomer filling and restoring the tooth with a sandwich technique (with a composite covering the remains of the glass-ionomer cement).19
In 2015, a systematic review was published by Gupta et al. on the treatment and prevention of radiation-related caries. They state that, although this type of caries occurs for several reasons, hyposalivation remains the primary cause. Therefore, radiation-related caries can be prevented by preserving the salivary glands, or through prevention, by providing comprehensive dental care before, during, and after radiotherapy.20
In 2020, Palmier et al. wrote a narrative review on current diagnostic, prognostic, and management paradigms with clinical relevance. They found that several factors, such as xerostomia and dietary changes, may influence the development of radiation-related caries. CR with fluoride application appears to be the ideal option to manage radiation-related caries.21The most recent study found in the literature is a systematic review and meta-analysis conducted by Palmier et al. in 2021 on the impact of head and neck radiotherapy on the longevity of adhesive restorations, which includes the studies above.14-16,19 They concluded that head and neck radiotherapy affects the longevity of dental adhesive, and better survival rates were observed for CR restorations compared to GIC and RMGIC restorations. They also found that fluoride application showed a positive result in CR restorations and that CR restorations associated with fluoride gel applications appear to be the best method to restore Class V lesions in patients treated with head and neck radiotherapy.22)
Discussion
Studies show that the direct materials used to restore radiation-related caries are AG, CR, GIC, and RMGIC.14-16,19,21,22 GIC has the lowest success rate. Regarding the cavity restoration technique, only one study compared the conventional technique and ART and found no differences.18
Radiotherapy may induce a reduction in enamel crystallinity and enlarged crystals, contributing to reduced enamel wear resistance.7 Chemical alterations in dentin can occur during radiotherapy since its chemical components reorganize, thus altering the structures. This leads to a change in the structural organization of collagen.13 This causes the decarboxylation of the carboxylate side bonds in collagen, and this bond is responsible for the interaction of the mineral matrix and hydroxyapatite crystals.23 Morphologically, a disorganized dentin structure can be observed after radiotherapy using a scanning electron microscope. This can be associated with the reorganization of the collagen structure and compromises the dentin’s mechanical and adhesive properties.13 Performing direct restorations on patients undergoing radiotherapy is important since the literature shows that restorations can be compromised by the harmful effect of ionizing radiation on the bond strength to enamel and dentin, affecting the formation of the hybrid layer.12,13
CR restorations with fluoride gel applications seem to be a suitable alternative to restore Class V lesions in patients who have undergone radiotherapy.22 As irradiated patients present a high risk of caries, fluoride is recommended as it can reduce recurrent caries16,17 at defined specific concentrations and use instructions. The number of clinical studies is too small to determine the best management and protocol to follow to obtain better long-term results. Studies including CR as a restorative material did not analyze several adhesive systems.
The most analyzed failures in the studies were loss of material, marginal integrity, and recurrent caries at the restoration margin. Patient motivation, adequate plaque control, stimulation of salivary flow, and fluoride are essential to reduce the incidence of radiation-related caries.20 The follow-up period of the studies was two years, so long-term clinical studies are needed. These lesions most typically appear on roots. As the lesion progresses rapidly and salivary fluid decreases, the condition can advance and affect the root.11 In 2018, Velo et al. demonstrated that irradiated root dentin was less mineralized in vitro study. This could have decreased the substrate’s permeability and solubility11 and consequently affected the adhesion of restorative materials.
Conclusions
Based on the literature, it is concluded that radiation-related caries is commonly restored with conventional glass-ionomer cement, resin-modified glass-ionomer cement, and composite resin with fluoride applications. More studies are needed to determine the best treatment, including cavity preparation technique and restorative material with better results. We suggest conducting studies comparing various adhesive systems, fluoride concentrations, and root dentin restorations.
REFERENCES
1. Tenuta LMA, Cury JA. Fluoride: its role in dentistry. Braz Oral Res. 2010; 24 (Suppl 1):9 -17. [ Links ]
2. Estupiñán-Day S. Promoting oral health: the use of salt fluoridation to prevent dental caries. Washington: PAHO, 2005. [ Links ]
3. Horowitz HS. Decision-making for national programs of community fluoride use. Community Dent Oral Epidemiol. 2000; 28(5):321-9. [ Links ]
4. Marthaler T, Petersen P. Salt fluoridation- an alternative in automatic prevention of dental caries. Int Dent J. 2005;55(6):351-8. [ Links ]
5. Ditterich RG, Rodrigues CK, Wambier DS. Fluoride salt as a alternative in public oral health: advantages and disadvantages. Rev Inst Ciênc Saúde, 2005; 23(3): 231-4 [ Links ]
6. Uruguay. Ministerio de Salud Pública. Comisión Honoraria de Salud Bucal. Encuesta de Salud Bucal en escolares de 11 a 14 años. Sector Público. Montevideo: MSP, 1999 [ Links ]
7. Martínez-Mier EA, Soto Rojas AE, Buckley CM, Stookey GK, Zero DT, Margineda J. Evaluación del contenido de flúor en la sal de mesa fluorada. Salud Pública Mex. 2004 May-Jun; 46(3):2003-4. [ Links ]
8. Walsh K I and Cury J A. Fluoride concentrations in salt marketed in Managua, Braz. Oral Res. 2018;32: e45 [ Links ]
9. Hernández-Guerrero JC, Fuente-Hernández J, Jiménez-Farfán MD, Ledesma-Montes C, Castañeda-Castaneira E, Molina-Frechero N, et al. Fluoride content in table salt distributed in Mexico City, Mexico. J Public Health Dent. 2008; 68(4):242-5. [ Links ]
10. Franco AM, Saldarriaga A, Gonzalez MC, Martignon S, Arbelaez MI, Ocampo A. Concentración de fluor en la sal de cocina en cuatro ciudades colombianas. Revista CES Odontología 2003;16: 21-6. [ Links ]
11. Tovar Valencia S, Castrillon Misnaza S. Perspectiva del uso del flúor vs caries y fluorosis dental. Colombia: Minsalud; 2016 [cited 2017 Sep 29] Disponible en: http://www.minsalud.gov.co/sites/rid/Lists/Bibliotecadigital/RIDE//VS/PP/ENT/perspectiva-uso-fluor.pdf. [ Links ]
12. Walsh KI, Cury JA. Fluoride concentrations in salt marketed in Managua, Nicaragua. Braz Oral Res. 2018; 24, 32:e45. [ Links ]
13. Mier EAM, Rojas AES, Buckley CM, Margineda J, Zero DT. Evaluation of the direct and diffusion methods for the determination of fluoride content in table salt. Community Dent Health, 2009; 26(4): 204-10. [ Links ]
14. Marthaler TM. Salt Fluoridation and Oral Health. Acta Medica Academica, 2013; 42(2): 140-55. [ Links ]
15. Sagheri D, Mcloughlin J, Clarckson J J. A comparison of dental caries levels in two communities with different oral health prevention strategies stratified in different social classes. Journal of Public Health Dentistry, 2007; 67(1): 1-7. [ Links ]
16. Fabruccini A, Alves LS, Alvarez L, Alvarez R, Susin C, Maltz M. Comparative Effectiveness Of Water And Salt Community-Based Fluoridation Methods In Preventing Dental Caries Among Schoolchildren. Community Dent. Oral Epidemiol, 2016; 44(6): 577-85. [ Links ]
17. Mejía R, Espinal F, Vélez H, Aguirre M. Fluoruración de la sal en cuatro comunidades colombianas. VIII. Resultados obtenidos de 1964 a 1972. Bol Oficina Sanit Panam. Colombia, 1976; 80: 205. [ Links ]
18. Hu JY, Chen XC, Li YQ, Smales RJ, Yip KH. Radiation-induced root surface caries restored with glass-ionomer cement placed in conventional and ART cavity preparations: results at two years. Aust Dent J. 2005;50(3):186-90. doi: 10.1111/j.1834-7819. 2005.tb00359. x. [ Links ]
19. De Moor RJG, Stassen IG, Veldt YV, Torbeyns D, Hommez GMG. Two-year clinical performance of glass ionomer and resin composite restorations in xerostomic head- and neck-irradiated cancer patients. Clin Oral Invest. 2011;15:31-38 DOI 10.1007/s00784-009-0355-4 [ Links ]
20. Gupta N, Pal M, Rawat S, Mandeep S Grewal MS, Garg H, Chauhan D, Ahlawat P, et al. Radiation-induced dental caries, prevention and treatment - A systematic review. Natl J Maxillofac Surg. Jul-Dec 2015;6(2):160-6. doi: 10.4103/0975-5950.183870 [ Links ]
21. Palmier NR, Migliorati CA, Prado-Ribeiro AC Querido de Oliveira MC, Vechiato Filho AJV, et al. Radiation-related caries: current diagnostic, prognostic, and management paradigms. Oral Surg Oral Med Oral Pathol Oral Radiol. 2020;130(1):52-62. doi: 10.1016/j.oooo.2020.04.003 [ Links ]
22. Palmier NR, Troconis CCM, Normando AGC, Guerra ENS, Araújo ALD, Arboleda LPA, Fonsêca JM, Paglioni MP, Gomes-Silva W, Vechiato Filho AJ, González-Arriagada WA, Leme AFP, Prado-Ribeiro AC, Brandão TB, Goes MF, Lopes MJ, Santos-Silva AR. Impact of head and neck radiotherapy on the longevity of dental adhesive restorations: A systematic review and meta-analysis. J Prosthet Dent. 2021;11;S0022-3913(21)00068-8 [ Links ]
23. Franzel W, Gerlach R, Hein HJ, Schaller HG. Effect of tumor therapeutic irradiation on the mechanical properties of teeth tissue. Z Med Phys. 2006;16(2):148-54. https://doi.org/10.1078/0939-3889-00307 [ Links ]
Conflict of interest declaration: The authors have no conflict of interest regarding the publication of this paper.
Authorship contribution 1. Conception and design of study 2. Acquisition of data 3. Data analysis 4. Discussion of results 5. Drafting of the manuscript 6. Approval of the final version of the manuscript BLPM has contributed in: 1, 2, 3, 4, 5, 6. LVMLR has contributed in: 1, 2, 3, 4, 5, 6. LFT has contributed in: 1, 4, 5, 6. FCPG has contributed in: 1, 4, 5, 6. APDR has contributed in: 1, 3, 4, 5, 6.
Received: August 25, 2021; Accepted: November 30, 2021
 Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
