










Serviços Personalizados
Journal

Artigo
 texto em
texto em  Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
Links relacionados
Compartilhar

 Permalink
PermalinkOdontoestomatología
versão impressa ISSN 0797-0374versão On-line ISSN 1688-9339
Odontoestomatología vol.20 no.31 Montevideo jun. 2018
https://doi.org/10.22592/ode2018n31a3
Research
Morphometric characteristics of multirooted teeth and furcation area
1
 http://orcid.org/10000-0002-9587-520X
http://orcid.org/10000-0002-9587-520X
2
http://orcid.org/20000-0002-6926-2098
3
http://orcid.org/30000-0001-5247-2454
4
http://orcid.org/0000-0002-0804-4302
1 Universidad Nacional Mayor de San Marcos. Lima. Perú. yuricastro_16@hotmail.com
2 Dental Students’ Scientific Society. Universidad Nacional Mayor de San Marcos. Lima. Perú
3 Dental Students’ Scientific Society. Universidad Nacional Mayor de San Marcos. Lima. Perú
4 Dental Students’ Scientific Society. Universidad Nacional Mayor de San Marcos. Lima. Perú
5 Dental Students’ Scientific Society. Universidad Nacional Mayor de San Marcos. Lima. Perú
6 Dental Students’ Scientific Society. Universidad Nacional Mayor de San Marcos. Lima. Perú
Objective.
The aim of this study is to describe the morphometric characteristics of multirooted teeth at the furcation area.
Method.
Fifty-four multirooted teeth (maxillary and mandibular teeth) were evaluated using a precision calibrator: root trunk length, root separation, root divergence angle, root length, length of cervical enamel projections and presence of enamel pearls.
Results.
The divergence angle of the maxillary distal furcation (50°) was greater than on the buccal (22°) and mesial (37°) aspects. On the mandible it was 25° on the buccal aspect and 22° lingually. No enamel pearls were found. The cervical enamel projections most commonly found were class I on the oral aspect (60% for maxillary teeth and 31% for mandibular teeth). The length of the lingual root trunk was 2.8 mm, and on the buccal aspect it was 2.2 mm.
Conclusion.
The root trunk of mandibular molars is larger lingually than on the buccal aspect, as is the palatal area of maxillary molars. In maxillary molars the greater divergence angle appeared at the entrance of the distal furcation, which is the one recommended to start using mechanical instruments.
Keywords: furcation defects; periodontal disease; tooth root; periodontal attachment loss; periodontitis
Objetivo.
Describir las características morfométricas de los dientes multirradiculares a nivel de la zona de furcación.
Método.
54 dientes multirradiculares (maxilares y mandibulares); fueron evaluados a través de un calibrador de precisión: longitud del tronco radicular, separación radicular, ángulo de divergencia radicular, longitud radicular así como la extensión de las proyecciones cervicales del esmalte y presencia de perlas del esmalte. Resultados. El ángulo de divergencia de la furca distal (50°) maxilar fue mayor que a nivel bucal (22°) y mesial (37°), a nivel mandibular bucal fue de 25° y lingual de 22°. No se encontró perlas del esmalte y las proyecciones cervicales del esmalte más comunes fueron de clase I a nivel bucal (60% para maxilares y 31% para mandibulares). La longitud del tronco radicular lingual fue de 2,8mm y a nivel bucal de 2,2mm.
Conclusión.
El tronco radicular de los molares mandibulares es mayor a nivel lingual que bucal, al igual que la zona palatina de molares maxilares. En los molares maxilares el mayor ángulo de divergencia se presentó en la entrada de la furca distal, siendo esta la recomendable para iniciar la instrumentación mecánica.
Palabras clave: Defectos de furcación; enfermedades periodontales; raíz del diente; pérdida de la inserción periodontal; periodontitis
Introduction
Multirooted teeth have unique anatomical features that pose a challenge to patients and clinicians because they cannot be properly accessed to effectively control dental biofilm. This condition can affect patients that are susceptible to periodontal disease because insertion loss may progress and involve the furcation area both vertically and horizontally.
Dental furcation is the anatomic area of a multirooted tooth where the roots diverge1,2. Anatomically it consists of a roof, the fornix (most coronal surface from the root separation) and the area of root separation3,4.
It is essential to know the anatomy of multirooted teeth to make the right diagnosis and therapeutic decisions. For example, we know that the distobuccal root of the first mandibular molars and the distal root of maxillary molars have the smallest root surface area; this is why they are more likely to undergo root extraction4. Bower5 found that 81% of furcations have an entrance < 1 mm, and 58% an entrance < 0.75 mm. The width of a traditional curette is 0.75 mm, so its use is not enough in this area. Chiu6 found that 49% of molars have a < 0.75 mm entrance on average. Additionally, the furcation entrance through the vestibular area is smaller than through the lingual area in mandibular molars5; mechanical instruments are harder to use lingually, so furcation involvement is more likely to occur.
Furcation invasion or involvement is the pathological resorption of interradicular bone with the subsequent furcation exposure1. This is a condition that increases the risk of bone loss, causing bone defects which are difficult to treat given the complex and irregular anatomy of the area7. It is important to know the anatomical features of multirooted teeth such as root trunk length, root divergence angle, root separation, and to observe cervical enamel projections and enamel pearls to control the morphological predisposing factors that lead to furcation involvement. In this study we evaluated the morphometric characteristics of multirooted teeth that are related to dental furcation.
Method
Descriptive in vitro observational study that included 54 multirooted teeth (first, second and third mandibular and maxillary molars). The teeth were selected from the Tooth Bank of the Dental Students’ Scientific Society, School of Dentistry, Universidad Nacional Mayor de San Marcos, Lima, Perú. The teeth had to be in good morphological conditions from the cementoenamel junction to the root apex. We excluded the teeth with structures that made it difficult to see the root area (hypercementosis, fractures, concavities, etc.). We also excluded teeth with open apices or loss of structure in the tooth roots (root resorption). The teeth were washed with saline solution and scaled at the root surface with 5/6 and 7/8 Gracey curettes to see their anatomical features more clearly.
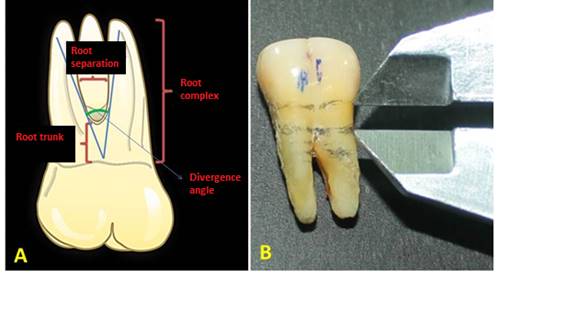
The characteristics evaluated included: root trunk length (RT, evaluated from the cementoenamel junction to the furcation entrance); root separation (RS, apical distance between the roots at the furcation level); root divergence angle (RD, angle formed by the roots at the furcation entrance); root length (RL, from the cementoenamel junction to the apex of each root) (Fig. 1). We also studied the presence/absence of enamel pearls (EP) as well as of cervical enamel projections (CEP) and classified them following Master’s8) categories: Class I (enamel projection < 1/3 of the root trunk), Class II (enamel projection > 1/3 of the root trunk without contact with the furcation) and Class III (enamel projection > 1/3 of the root trunk that extends to the furcation area).
The measurements were taken with a Mitutoyo© verner caliper and calibrated to an accuracy of 0.01 mm. The measurements were taken on the buccal and lingual/palatal aspects by a rater (YC); the comments on the extent of CEP and EP were made by two raters (YC and KS; interrater reliability Kappa = 0.96).
The data were processed with the SPSS 21 statistical package (IBM, United States). We used descriptive statistics and measures of central tendency and dispersion (mean and standard deviation). The differences between tooth types in the quantitative measurements were set with the ANOVA test for independent groups for mandibular molars; while the Student t test was used for independent groups for maxillary molars. The differences in the qualitative assessments between the groups were set applying the Mann-Whitney U test. A statistical significance of 0.05 was set to disprove the null hypothesis.
Results
Regarding mandibular molars (vestibular aspect), dimensions were greater for the second molar with an average root separation of 2.11 mm (p < 0.05), a divergence angle of 27.5° (p > 0.05) and a root length of 14 mm (p < 0.05). The root trunk of the first molar was greater than the second and third molars with an average of 2.6 mm (p < 0.05) (Table 1).
Table 1: Morphometric characteristics of mandibular molars on the buccal surface
| Tooth | Buccal characteristics | |||
|---|---|---|---|---|
| Root trunk | Root separation | Divergence angle | Root length | |
| First Molar | 2.59 ± 0.79mm* | 1.81 ± 0.27mm | 25.77 ± 3.75° | 12.68 ± 0.69mm |
| Second molar | 1.63 ± 0.32 | 2.11 ± 0.72* | 27.56 ± 11.31 | 13.97 ± 1.35* |
| Third molar | 2.5 ± 0.5 | 1.26 ± 1.15 | 10 ± 9.16* | 10.54 ± 0.43 |
| Total | 2.18 ± 0.75 mm | 1.86 ± 0.67 | 24.48 ± 9.9 | 12.9 ± 1.48 |
*p < 0.05 ANOVA for independent groups. Tuckey’s Post Hoc test.
On the lingual surface, root trunk, root separation, divergence angle and root length were greater in the first molar, unlike the second and third molars (p > 0.05 (Table 2).
Table 2: Morphometric characteristics of mandibular molars on the lingual surface
| Tooth | Lingual characteristics | |||
|---|---|---|---|---|
| Root trunk | Root separation | Divergence angle | Root length | |
| First Molar | 2.9 ± 0.44mm | 1.79 ± 0.33mm | 23,88 ± 4,51°* | 13.69 ± 0.71mm |
| Second molar | 2.7 ± 0.33 | 1.72 ± 0.86 | 24.12 ± 9.42 | 13.03 ± 0.84 |
| Third molar | 2.62 ± 0.44 | 1 ± 0.91 | 10.4 ± 9.52 | 9.68 ± 1.58* |
| Total | 2.78 ± 0.41mm | 1.66 ± 0.71 | 22.25 ± 8.65 | 12.91 ± 1.56 |
*p < 0.05 ANOVA for independent groups. Tuckey’s Post Hoc test.
On the vestibular area of maxillary molars we found a greater root length on the second molar (3.7 mm; p > 0.05) and higher root length (12 mm; p > 0.05). The first molar had greater lengths in the root separation and divergence angle (p > 0.05) (Table 3).
Table 3: Morphometric characteristics of maxillary molars on the buccal surface
| Tooth | Buccal characteristics | |||
|---|---|---|---|---|
| Root trunk | Root separation | Divergence angle | Root length | |
| First Molar | 3.42 ± 0.47mm | 2.22 ± 0.11mm | 23 ± 5.16° | 11.83 ± 0.71mm |
| Second molar | 3.72 ± 0.73 | 1.99 ± 0.58 | 20.6 ± 7.89 | 12.15 ± 1.28 |
| Total | 3.52 ± 0.57mm | 2.15 ± 0.34 | 22.2 ± 6.02 | 11.93 ± 0.9 |
The teeth selected did not include a third maxillary molar. On the palatal aspect we found greater dimensions of root separation at the distal furcation on the first molar, as well as greater divergence angles on the distal aspect on the first and second molars (p > 0.05) (Table 4).
Table 4: Morphometric characteristics of maxillary molars on the palatal surface
| Tooth | Palatal characteristics | ||||||
| Mesial root trunk | Distal root trunk | Mesial root separation | Distal root separation | Mesial divergence angle | Distal divergence angle | Root length | |
| First Molar | 3.92 ± 0.56mm | 3.3 ± 0.41mm | 3.2 ± 0.65mm | 2.92 ± 0.45mm | 38.3 ± 7.27° | 55 ± 16.2° | 13.37 ± 0.6mm |
| Second molar | 3.81 ± 0.52 | 3.78 ± 0.72 | 2.9 ± 0.81 | 2.52 ± 0.65 | 33.8 ± 10.3 | 40.2 ± 20.31 | 13.42 ± 0.71 |
| Total | 3.89 ± 0.53 | 3.46 ± 0.56 | 3.1 ± 0.7 | 2.78 ± 0.53 | 36.8 ± 8.31 | 50.06 ± 18.4 | 13.39 ± 0.61 |
We did not find any enamel pearls on the root surface, neither on the vestibular nor the lingual/palatal areas. Class I cervical enamel projections were predominant: they appeared on 60% of maxillary on the vestibular aspect, and on 31% of mandibular molars. We found no predisposition of cervical enamel projections according to type of tooth and the area assessed (p > 0.05) (Table 5).
Table 5: Characteristics of the cervical enamel projections found
| Cervical enamel projection | Buccal area | Lingual/palatal area | ||||
| Maxilla | Mandible | Total | Maxilla | Mandible | Total | |
| Absent | 6 (40%) | 24 (61.5%) | 30 (55.6%) | 15 (100%) | 34 (87.2%) | 49 (90.7%) |
| Class I | 9 (60%) | 12 (30.8%) | 21 (38.9%) | 0 | 5 (12.8%) | 5 (9.3%) |
| Class II | 0 | 3 (7.7%) | 3 (5.6%) | 0 | 0 | 0 |
| Class III | 0 | 0 | 0 | 0 | 0 | 0 |
| Total | 15 | 39 | 100 | 15 | 39 | 54 |
Discussion
Incomplete removal of dental biofilm reduces the success rate of periodontal treatment; multirooted teeth have special anatomical features that prevent the success of the treatment. We know that cervical enamel projections increase biofilm accumulation; additionally, during regenerative therapy they hinder the formation of new connective tissue9. Our study found no CEPs on the root surface, and the general prevalence is low; Moskow10 reports an incidence of 2.6%. If they appear, their removal through odontoplasty is recommended as they are a predisposing factor for furcation involvement.
First maxillary molars have a smaller buccal furcation entrance than the mesial and distal entrances5. They have a root trunk ≥ 3 mm11, with an average of 3.5 mm-3.6 mm mesial, 3.5 mm-4.2 mm buccal and 4.1 mm-4.8 mm distal12. In this study the average root trunk for the first molar was 3.4 mm on the buccal aspect, 3.9 mm on the mesial aspect and 3.3 mm on the distal aspect. Knowing these data about the root trunk allows us to predict the development or predisposition to furcation involvement. Molars with short root trunks are more vulnerable to furcation exposure but have a better prognosis after treatment (they provide easier access and use of instruments) when the tooth does not have severe periodontal destruction. These teeth have a smaller area for periodontal adherence13. Short trunks are associated with long roots and thus facilitate resective therapy13.
In the onset of periodontal disease, molars with long root trunks have a better prognosis as the furcation position is protected; but if the disease progresses, the prognosis is not favorable13. Long trunks are associated with short roots and therefore are not candidates for resective therapy, and tend to have greater loss of periodontal support and furcation invasion2.
Regarding mandibular molars, we found an average buccal root trunk of 2.2 mm, and of 2.8 mm on the lingual aspect. These data are similar to those of Santana et al.14 (2.8 mm and 3.5 mm on the buccal and lingual aspects respectively). Root separation and divergence angle were higher in lower second molars; this is favorable because it allows for the use of curettes in the area. As the lingual area has greater dimensions, furcation involvement does not progress; however, once present, access through mechanical instrumentation is limited. According to Marcaccini et al.13, the lingual furcation of mandibular molars has a smaller entrance and a longer root trunk. This suggests a stronger limitation for instrumentation in the area and possibly a worse prognosis for periodontal disease.
Regarding CEPs, they are frequent and difficult to detect in healthy teeth. There is a direct link between them and furcation involvement15. Hou16 found that 63% of molars with furcation involvement had cervical enamel projections, which shows that they are more prevalent in first and second molars. They are considered a cofactor in furcation involvement. Master8 found a 28.6% incidence on mandibular molars and 17% in maxillary molars, finding a correlation in the development of furcation involvement in mandibular molars. However, Leib17 did not find such correlation. In this study we found a low CEP frequency. The most common type was class I on the buccal aspect in maxillary and mandibular first molars.
Conclusion
The root trunk of mandibular molars is larger lingually than on the buccal aspect, as is the palatal area of maxillary molars. The divergence angle in the buccal area of mandibular molars was 24.5° and in maxillary molars it was 22°. In maxillary molars, the greatest angle appeared at the entrance of the distal furcation, making this the best entrance to start using mechanical instruments. We found no enamel pearls, and class I cervical enamel projections were the most frequent ones, mainly on first molars
Referencias
1. American Academy of Periodontology. Glossary of periodontal terms. 3rd ed. Chicago: AAP, 1992. 56p. [ Links ]
2. Al-Shammari KF, Kazor CE, Wang HL. Molar root anatomy and management of furcation defects. J Clin Periodontol. 2001; 28 (8): 730-40. [ Links ]
3. Marcaccini AM, Pavanelo A, Nogueira AV. Morphometric study of the root anatomy in furcation area of mandibular first molars. J Appl Oral Sci. 2012; 20 (1):76-81. [ Links ]
4. Grados SP, Castro YR, Bravo FC. Consideraciones clínicas en el tratamiento quirúrgico periodontal. 1era ed. Caracas: AMOLCA; 2014. 241p. [ Links ]
5. Bower RC. Furcation morphology relative to periodontal treatment. Furcation root surface anatomy. J Periodontol. 1979; 50 (7): 366-74. [ Links ]
6. Chiu BM, Zee KY, Corbet EF, Holmgren CJ. Periodontal implications of furcation entrance dimensions in Chinese first permanent molars. J Periodontol 1991; 62 (5): 308-11. [ Links ]
7. Cattabriga M, Pedrazzoli V, Wilson TG Jr. The conservative approach in the treatment of furcation lesions. Periodontol 2000. 2000; 22: 133-53. [ Links ]
8. Masters DH, Hoskins SW. Projection of cervical enamel into molar furcations. J Periodontol. 1964; 35 (1): 49- 53. [ Links ]
9. Mardam-Bey W, Majzoub Z, Kon S. Anatomic considerations in the etiology and management of maxillary and mandibular molars with furcation involvement. Int J Periodontics Restorative Dent. 1991; 11 (5): 398-409. [ Links ]
10. Moskow BS, Canut PM. Studies on root enamel (1). Some historical notes on cervical enamel projections. J Clin Periodontol. 1990; 17 (1): 29- 31. [ Links ]
11. Carlsen O. Dental morphology. 1est ed. Copenhagen: Munksgaard,1987.194p. [ Links ]
12. Gher MW, Dunlap RW. Linear variation of the root surface area of the maxillary first molar. J Periodontol. 1985; 56 (1): 39-43. [ Links ]
13. Marcaccini AM, Pavanelo A, Nogueira AV, Souza JA, Porciúncula HF, Cirelli JA. Morphometric study of the root anatomy in furcation area of mandibular first molars. J Appl Oral Sci. 2012; 20 (1):76-81. [ Links ]
14. Santana RB, Uzel MI, Gusman H, Gunaydin Y, Jones JA, Leone CW. Morphometric analysis of the furcation anatomy of mandibular molars. J Periodontol. 2004; 75 (6): 824-9. [ Links ]
15. DeSanctis M, Murphy KG. The role of resective periodontal surgery in the treatment of furcation defects. Periodontol 2000. 2000; 22: 154-68. [ Links ]
16. Hou GL, Tsai CC. Relationship between periodontal furcation involvement and molar cervical enamel projections. J Periodontol 1987; 58 (10): 715-21. [ Links ]
17. Leib AM, Berdon JK, Sabes WR. Furcation involvements correlated with enamel projections from the cement enamel junction. J Periodontol 1967; 38 (4): 330-4. [ Links ]
Received: July 01, 2017; Accepted: November 29, 2017
 Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
