ARCHIVOS DEL INSTITUTO DE NEUROLOGÍA
Absceso intramedular cervical en paciente inmunodeprimido
Intramedullary abscess of the cervical spinal cord in an
immunodepressed patient
Dra. Viviana Cabrera
Residente de Neurocirugía del Hospital Maciel. Facultad de Medicina. UdelaR. Montevideo.
Dr. Edgardo Spagnuolo
Neurocirujano, Jefe de Servicio de Neurocirugía del Hospital Maciel. Facultad de Medicina. UdelaR. Montevideo.
Dr. Edgar Nicoli
Neurocirujano. Servicio de Neurocirugía del Hospital Maciel. Facultad de Medicina. UdelaR. Montevideo.
Recibido: 17/04/15 – Aceptado: 07/07/15
Trabajo del Servicio de Neurocirugía del Hospital Maciel (ASSE). Unidad Docente Asociada, Escuela de Graduados, Facultad de Medicina (UdelaR). Montevideo, Uruguay
Correspondencia: Dr. Edgardo Spagnulo. Servicio de Neurocirugía del Hospital Maciel (ASSE). 25 de mayo 174, Montevideo, Uruguay. Correo electrónico: spagjohn@yahoo.com
RESUMEN: Arch Med Interna 37(2): 98-100
Los abscesos intramedulares son lesiones poco frecuentes. Su incidencia es muy baja, lo que determina que su diagnóstico sea dificultoso. Se caracterizan por síndromes neurológicos variados, que están dominados por dolor vertebral y déficit neurológico, por lo general en presencia de fiebre. Se los vincula a focos infecciosos de vecindad y otras veces a diseminación hematógena. Son mas frecuentes en pacientes que presentan alguna inmunodepresión o afecciones sistémicas que favorezcan las infecciones en topografías poco habituales. Los autores presentan un caso de un paciente inmunodeprimido, con historia de dolor vertebral y posteriormente un severo déficit neurológico y en quien se diagnosticó un absceso intramedular, asociado a una espondilodiscitis. No se comprobó por los estudios ni en la cirugía continuidad entre las lesiones. Se hace un análisis del caso clínico y de la escasa bibliografía publicada al respecto
Palabras clave: Absceso intramedular. Espondilodiscitis.
ABSTRACT: Arch Med Interna 37(2): 98-100
Intramedullary spinal cord abscesses are infrequent lesions. Its incidence is very low, what determines that its hand held is a difficult one. Clinically they are characterized by varied neurological syndromes, which are dominated by vertebral pain and neurological deficits, associated with fever. The origin of these abscesses is usually related to neighbourhood foci, or to hematogenous dissemination from a distant focus. They are more frequent in patients qho are immunosuppressed or systemic conditions that promote infection in unusual topographies. The authors report a case of an inmunocompromised patient in whom an intramedullary cervical spinal cord abscess associated to spondylodiskitis was found. Neither in the image studies nor in surgery, was a continuity between both lesions confirmed. There is an analysis of the clinical case and the little literature published on the subject.
Key words: spinal cord abscess. Surgery.
INTRODUCCIÓN
Las infecciones que comprometen el Sistema Nervioso Central (SNC) son poco frecuentes, si no se tienen en cuenta las infecciones extra-axiales. Predominan ampliamente los abscesos cerebrales, pero su incidencia ha descendido en las últimas décadas debido a la detección y tratamiento precoz de focos infecciosos (sobre todo de la esfera otorrinolaringológica). Dentro de las infecciones del SNC, las infecciones intramedulares tienen una incidencia muy baja. Pero mucho más infrecuentes son las infecciones intramedulares(1-9). Se plantea que las infecciones medulares se dan en forma secundaria a un foco infeccioso de vecindad, como por ejemplo una infección discovertebral (espondilodiscitis, osteomielitis vertebral) o que pueden ser secundarias a infecciones a distancia sembradas a nivel medular, por vía hematógena(10,11). Los abscesos intramedulares, son por lo tanto afecciones de muy baja incidencia, que se plantea deben darse en pacientes con inmunodepresión o con afecciones de fondo que favorezcan las infecciones y su diseminación (por ejemplo diabetes de difícil control). De todas maneras, es poco frecuente que un paciente con una infección a distancia, desarrolle exclusivamente como localización secundaria un absceso intramedular. Esto teniendo en cuenta la mala y escasa irrigación medular. Por esto, el mecanismo que más se acepta es el secundario a infecciones vecinas. Lo raro en estos casos es que generalmente se da una colección supurada intramedular y sin abscesos epidurales o meningitis asociados o como única lesión. Cabe también destacar que las anteriores son infecciones más frecuentes, pero no se acompañan de una diseminación medular. Se pueden ver extensas colecciones epidurales, pero la duramadre es siempre una barrera infranqueable para la infección. También son muy escasas las publicaciones de infecciones intradurales por el mismo motivo.
Los autores presentan el caso de un paciente joven, portador de un absceso intramedular. Se hace un análisis del caso clínico, su imagenología, su resolución quirúrgica y se hace una revisión de la escasa bibliografía existente al respecto.
CASO CLÍNICO
Paciente de 20 años, sexo masculino, HIV positivo de 2 años de diagnóstico, en control médico irregular. Comienza 1 mes antes del ingreso con dolor cervical sin irradiación que fue haciéndose progresivamente más intenso. Dos semanas después agrega fiebre y odinofagia. En la semana previa al ingreso nota parestesias y disestesias en ambos miembros inferiores, agregando luego impotencia funcional la que progresivamente se transformó en una paraparesia, que el día del ingreso le impide mantenerse de pie. Dos días previos había agregado parestesias con disestesias en ambos miembros superiores y pérdida de fuerzas en ambas manos. El día del ingreso refiere “adormecimiento” desde el cuello hacia abajo. No orinó en las últimas 36 hs. Al examen del ingreso: mal aspecto general. Adelgazado, palidez cutáneo mucosa. Febril, 39ºC axilar. Mala perfusión periférica, hipotensión arterial, taquicardia. En lo neurológico: cuadriparesia severa a predominio crural, donde tiene fuerzas M1 en la escala del British Medical Council. Reflejos vivos con Babinski bilateral. Hipoestesia con nivel desde T1 y anestesia desde T3. Globo vesical que obliga a colocación de sonda vesical.
Se decide la intervención de emergencia para evacuar el absceso intramedular. Se realiza una mínima hemilaminectomía a nivel de C5, con apertura dural y punción. Se realiza pequeña apertura de duramadre y punción con trocar fino evacuándose varios centímetros cúbicos de pus fétido. A posteriori y luego de 48 hs. de intenso tratamiento para estabilización hemodinámica se realizó abordaje anterior, se evacuó el absceso prevertebral, posteriormente se siguió con corporectomía C5 y C6, con discectomía y estabilización raquídea con instrumentación anterior. Desde el ingreso se comenzó con tratamiento antibiótico empírico. A las 72 hs. de la segunda cirugía fallece en shock séptico. En el material purulento evacuado se encontraron abundantes leucocitos polimorfonucleares, pero el cultivo fue negativo para identificar germen.
DISCUSIÓN y comentarios
Desde la primera descripción de un absceso intramedular, hecha por Hart en 1830, son escasas las publicaciones sobre el tema(9). Por ejemplo, en una revisión de 2009, Kurita y cols. encuentran unos 120 casos publicados de abscesos intramedulares(9,12-14). La mayoría de las publicaciones son reportes de caso, salvo una serie con tres casos(12). El mismo autor también destaca la extrema rareza de la patología y de la importancia de hacer un diagnóstico precoz, ya que tienen una alta incidencia de mortalidad y de secuelas invalidantes entre los sobrevivientes. Le da gran importancia al uso de antibióticos adecuados, y que los mismos han incidido y en forma significativa en la evolución posterior de estos pacientes.
En general se hace hincapié en la rareza de la patología, de su mal pronóstico vital y funcional si no se diagnostica precozmente y se trata adecuadamente(1,3,4,13). Se discuten según los diferentes autores las distintas técnicas quirúrgicas para evacuar el absceso, e incluso el tratamiento empírico con antibióticos sin cirugía(4,9,10,14). La mayoría de las publicaciones hacen referencia a que el absceso intramedular es secundario a una lesión previa del SNC y sobre todo de la médula: abscesos secundarios a heridas de arma de fuego, a cirugías intramedulares por otra causa, a senos dérmicos, etc(5-7,10,11,14). Vora publica en el 2004 un caso secundario a una toracotomía por un carcinoma de esófago(13).
Otros autores relacionan la aparición de un absceso intramedular a la existencia de un tumor intramedular, como por ejemplo un ependimoma, mientras que hay también quienes han publicado casos relacionados con afecciones hematológicas, que determinan una isquemia crónica medular, con estasis circulatoria, que en presencia de un foco infeccioso a distancia pueden favorecer la formación de un absceso intramedular(2,5,7,8).
El diagnóstico de absceso intramedular se plantea por la clínica y se confirma con la imagenología. La clínica de nuestro paciente es comparable con lo mencionado en la revisión realizada por Kurita de que la fiebre, el síndrome neurológico deficitario y los trastornos esfinterianos dominaron la clínica(9). También es compatible en que en un elevado número de casos había antecedentes de un foco infeccioso de vecindad.
En cuanto a la imagenología, el estudio que permite el diagnostico de absceso intramedular es la RM. Se puede ver la lesión y su vinculación o no con focos de vecindad(7). La confirmación del germen se obtiene con la cirugía, aunque los cultivos pueden ser negativos, ya que no se recomienda esperar el cultivo para comenzar el tratamiento antibiótico dada la gravedad que supone este tipo de lesión.
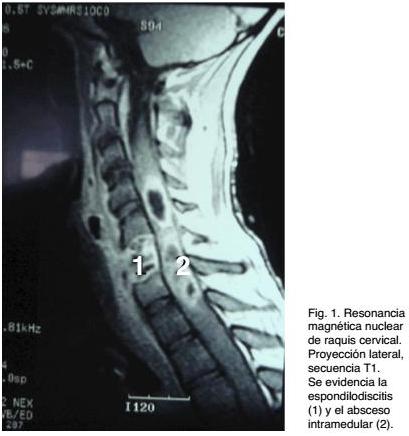
Si bien se reportan casos en los que no había foco infeccioso demostrable ni de vecindad ni a distancia, en el caso analizado en esta presentación había un foco infeccioso de vecindad (espondilodiscitis). En el mismo, la imagenología simple (RX de columna cervical) y la Tomografía Computada de raquis fueron positivas en demostrar una lesión discovertebral, con las características de una espondilodiscitis C5-C6, con alteraciones vertebrales, secundarias a osteomielitis. Estas lesiones explican el cuadro doloroso de semanas de evolución, tipificado como dolor raquídeo y el síndrome toxi-infeccioso de los días previos al ingreso. Por el déficit neurológico, que evolucionó rápidamente, se solicitó una RM de raquis, que evidenció una extensa lesión medular, con aspecto de un absceso multilobulado asociado a edema y ensanchamiento medular cervical. Se destaca que no había compromiso epidural ni subdural. El proceso patológico medular estaba centrado en la topografía de la lesión discovertebral, pero no había evidencia imagenológica de continuidad. La terapéutica quirúrgica requirió dos intervenciones, una de emergencia para evacuar el absceso, dado lo severo del déficit neurológico y una segunda a las 48 hs y ya estabilizado el paciente, donde se realizó la corporectomía y posterior instrumentación raquídea. A pesar del tratamiento quirúrgico y del tratamiento empírico con antibióticos instituido desde el ingreso, la evolución no fue buena. A las 72 hs. de la segunda cirugía fallece, dado que había evolucionado a un cuadro infeccioso generalizado con repercusión multisistémica (shock séptico).
Respecto a los gérmenes, el Staphilococcus aureus es el que predomina, pero se han encontrado a gérmenes agresivos poco comunes, hongos, micobacterias, etc. También hay casos de cultivo negativo(13).
Predominan en el sexo masculino y la topografía más frecuente en altura a nivel medular es dorsal o a nivel terminal medular. Menos frecuentes son las lesiones a nivel cervical
Por último se los divide también en cuanto al tiempo de evolución de los síntomas en agudos, subagudos y crónicos. Los dos primeros por lo general se vinculan a gérmenes comunes, mientras que los crónicos se ven más frecuentemente en infecciones específicas como micobacterias.
El tratamiento de los abscesos medulares ha variado con los años. Hasta no hace muchos años se planteaba la necesidad de una extensa laminectomía y evacuación completa de la colección supurada. En la actualidad y dependiendo de la situación clínica se puede plantear desde una mínima cirugía, con punción y evacuación de material purulento, hasta aquellos que plantean que si la situación clínica lo permite y si la evolución no muestra agravación de la signología, se podría hacer tratamiento exclusivamente antibiótico. Hay reportes de curación exclusivamente con este tratamiento(1,2,4,9,11,14).
1. Blacklock B, Hood T, Maxwell, R. Intramedullary spinal cord abscess. Case Report. J Neurosurg 1982;57:270-273.
2. Brasme C, Peruzzi P, Bertault R. Intramedullary abscess of the spinal cord in a patient with a right tolift shunt. Case Report. Clin Infect Dis 1997;24:89-90.
3. Byrne R, Van Roem K, Whisler W. Intramedullary abscess: a report of two cases. Neurosurgery 1994;35:321-326.
4. Chan C, Gold W. Intramedullary abscess of the spinal cord in the antibiotic era. Clin Infect Dis 1998;27:619-623.
5. Desai K, Muzundar D, Goel A. Holocord intramedullary abscess. Spinal Cord 1999;37:866-870.
6. Gerlach R, Zimmermann M, Hermann E, Kieslich M, Weidauer S, Seifert V. Large intramedullary abscess of the spinal cord associated with an epidermoid cyst without dermal sinus. Case report. J Neurosurg Spine 2007;7:357-361.
7. Jungreis C, Rothfus W, Latchaw R. Tumors and infections of the spine and spine cord. In: Latchaw R, editor. MRI and CT imaging of the head, neck and spine.
8. Koppel B, Daras M, Duffy K. Intramedullary spinal cord abscess. Neurosurgery 1990;26:1441-1446.
9. Kurita N, Sakuray Y, Tanguchi M, Terao T, Takahashi H, Mannen T. Intramedullary spinal cord abscess treated with antibiotic. Case report. Neurol Med Chir (Tokyo) 2009;49: 262-268.
10. Maldonado L, Soloaga E, Veltri M. Absceso intramedular en paciente con Enfermedad de Rendu Osler Weber. Medicina (B. Aires) 2007;67:2-6.
11. Murphy K, Brunberg J, Quint D. Spinal cord infection: myelitis and abscess formation. AJNR 1998;19:341-348.
12. Tacconi L, Johnston F, Thomas D. Intramedullary spinal cord abscess. Neurosurgery 1995;37:817-819.
13. Vora A , Raad I, McCutcheon E. Intramedullary abscess from group F Streptococcus. Surg Infect (Larchmt) 2004;5(2):200-204.
14. Wright RL. Intramedullary spinal cord abscess. Report a case secondary to stab wound with good recovery following operation. J Neurosurg 1965;23: 208-210.