Estudio prospectivo de trombofilia y gestación en el Hospital de Clínicas. Período abril 2004 - febrero 2010.
Dra. Inés Sevrini
Profesora Adjunta de Clínica Médica y Hematóloga. Facultad de Medicina. UdelaR. E. Mail: isevrini@adinet.com.uy Montevideo.
Dra. Cecilia Carrizo ]]> Profesora Adjunta de Clínica Médica y Hematóloga. Facultad de Medicina. UdelaR. Montevideo.
Ricardo Robaina
Ayudante de Clase del Departamento de Métodos Cuantitativos. Facultad de Medicina. UdelaR. Montevideo.
Dra. Andrea Monteiro
Residente de Ginecotología. Facultad de Medicina. UdelaR. Montevideo.
Lic. Natalia Trías
Licenciada en Laboratorio.
Dr. Rodrigo Giorgetta
Residente de Ginecotología. Facultad de Medicina. UdelaR. Montevideo.
Dr. Víctor Machín ]]> Profesor Adjunto de Ginecotología. Facultad de Medicina. UdelaR. Montevideo.
Dra. Natalia Pérez
Residente de Ginecotología. Facultad de Medicina. UdelaR. Montevideo.
Dra. Rosario San Martín
Asistente de Laboratorio. Facultad de Medicina. UdelaR. Montevideo.
Dr. Marcelo De Agostini
Asistente de Ecografía de Ginecotocología. Facultad de Medicina. UdelaR. Montevideo.
Dra. Karina Lamela
Hematóloga. Facultad de Medicina. UdelaR. Montevideo.
Dr. Fernando Taranto ]]> Residente de Ginecotología. Facultad de Medicina. UdelaR. Montevideo.
Dr. Pablo López
Residente de Laboratorio. Facultad de Medicina. UdelaR. Montevideo.
Dra. Natalia García
Residente de Laboratorio. Facultad de Medicina. UdelaR. Montevideo.
Dra. Mariela Descia
Residente de Laboratorio. Facultad de Medicina. UdelaR. Montevideo.
Dra. Ana María Otero
Profesora Agregada de Hematología. Facultad de Medicina. UdelaR. Montevideo.
]]>
Resumen
Antecedentes: el estado de hipercoagulabilidad fisiológica del embarazo asociado a una trombofilia, no sólo puede determinar enfermedad tromboembólica, sino que puede interferir en la circulación placentaria ocasionando manifestaciones obstétricas vinculables a trombofilia (MOV): pérdidas recurrentes del embarazo, desprendimiento prematuro de placenta (DPP), la restricción del crecimiento fetal intrauterino (RCIU), el óbito fetal y la preeclampsia. El tratamiento con heparinas de bajo peso molecular (HBPM) ha cambiado la evolución del embarazo de estas pacientes. Objetivo: conocer la prevalencia de las trombofilias en la población de embarazadas con sospecha de trombofilia y lograr recién nacidos vivos sanos. Material y métodos: Pacientes con trombofilia o con alta sospecha de trombofilia por sus antecedentes personales de trombosis o sus antecedentes obstétricos vinculables a trombofilia. Se realizaron estudios etiológicos para trombofilias adquiridas y congénitas y se indicó un tratamiento y seguimiento personalizado según un protocolo de seguimiento y tratamiento preestablecido. Resultados: De un total de 207 pacientes que culminaron el embarazo, se confirmó trombofilia en el 63,3% de las pacientes. Se logró obtener recién nacidos vivos en un 90,3% de las pacientes. Sólo en un 9,7% se presentaron abortos u óbitos fetales. Conclusión: Mediante controles clínicos y paraclínicos estrictos y con ajustes del tratamiento según la etiología y seguimiento, se obtuvo alto porcentaje de recién nacidos vivos y sanos en pacientes con trombofilia o con MOV.
Palabra clave: trombofilia, gestación, pérdida recurrente de embarazo.
Summary
Background: The physiological hypercoagulable state of pregnancy associated with thrombophilia can not only determine thromboembolic disease but may interfere with placental circulation causing obstetric events be linked to thrombophilia (MOV): recurrent pregnancy loss, premature separation of placenta, intrauterine fetal growth restriction, the stillbirth and preeclampsia. Treatment with low molecular weight heparins has changed the course of pregnancy in these patients. The objective of this program is to determine the prevalence of thrombophilia in the population of pregnant women with suspected thrombophilia and achieve healthy newborns. Methods: Patients with thrombophilia or high suspicion of thrombophilia by their personal history of thrombosis or obstetric history be linked with thrombophilia. Etiological studies were performed for acquired and congenital thrombophilia and prescribed a treatment and as a personal follow up and treatment protocol preset. Results: Of a total of 207 patients who completed the pregnancy, thrombophilia was confirmed in 63.3% of patients. It was possible to obtain healthy live births and in 81.3% of patients, only by 9.7% were abortions or stillbirths. Conclusion: With strict clinical and laboratory controls and settings according to the etiology and treatment monitoring, we obtained high percentage of healthy newborns and in patients with thrombophilia or MOV.
Keywords: thrombophilia, pregnancy, recurrent pregnancy loss.
]]>
Recibido: 01/07/10 – Aceptado: 14/04/11
Correspondencia: Dra. Inés Sevrini, E. Mail: isevrini@adinet.com.uy
INTRODUCCIÓN
El sistema hemostático interviene de forma relevante durante el proceso reproductor. Durante la gestación normal se produce un estado de hipercoagulabilidad fisiológica(1). El buen desarrollo del embarazo depende entre otros factores, de una adecuada circulación placentaria.
La pérdida recurrente de embarazo (PRE) de 2 o más embarazos consecutivos es causada por diferentes enfermedades bien conocidas y otras en estudio: 7% se debe a anormalidades cromosómicas, 10% a anormalidades anatómicas, 15% son de causa hormonal (estrógenos, progesterona, diabetes, hormona tiroidea) y un 53-62% se debe a anomalías en la hemostasis(2). En la población general, la PRE se ve en un 2% de mujeres en edad reproductiva mientras que en mujeres con trombofilia conocida previamente al embarazo, menos de un 25% llegan tener un embarazo a término con feto vivo(3). La trombofilia puede ser de causa adquirida o genética. La trombofiia adquirida es el síndrome antifosfolipídicos (SAF) y las tromboflias genéticas más reconocidas son: por genes mutantes: Factor V Leyden (FVL), Protrombina G20210A (Prot.G20210A), metiltetrahidrofolatoreductasa (MTHFR) (4,5); por déficit de inhibidores de la coagulación ATIII, Proteína C y Proteína S; por exceso de FVIII; por alteraciones de la fibrinólisis: exceso de Inhibidor del activador del plasminogeno (PAI); aumento de la lipoproteína ”a” y aumento de la homocisteinemia. Cada vez se encuentran más evidencias que las pacientes con pérdidas recurrentes de embarazo y trombofilia, se ven beneficiadas con el tratamiento y el seguimiento multidisciplinario para poder culminar su embarazo en forma satisfactoria con un recién nacido vivo y sano (6,7). La aparición de las heparinas de bajo peso molecular (HBPM) ha cambiado en forma notoria el manejo de las pacientes con riesgo trombótico o con trombosis durante el embarazo (8). La combinación de defectos trombofílicos aumenta el riesgo de pérdida fetal como la demostró el estudio European Prospective Cohort on Thrombophilia (EPCOT) (9). Datos emergentes en los últimos 5 años, sugieren que la trombofilia manifiesta pueda corresponder entonces a un desorden multigenico (9). El estudio EPCOT demostró que el riesgo de pérdidas fetales está aumentado en las pacientes con trombofilia, siendo mayor para pérdidas fetales con un riesgo relativo (RR) 3.6, que para abortos con RR 1.3, y mayor para defectos combinados que para defectos aislados (RR 14.3). La mutación de la Protrombina 20210 también fue asociada a pérdidas fetales tardías (RR 3.3).
Existen diferencias entre los múltiples estudios, meta-análisis y revisiones realizadas en los últimos años, por presentar variados criterios de inclusión, número de embarazos perdidos previamente, dispersión en el “N” y en los tipos de trombofilia, así como análisis de pérdidas tempranas y/o tardías del embarazo, con un espectro variado en los tratamientos y dosis. Esto dificulta el análisis de los datos y el poder concluir en recomendaciones basadas en evidencia científica, si bien existen múltiples estudios internacionales y nacionales que avalan esta hipótesis.
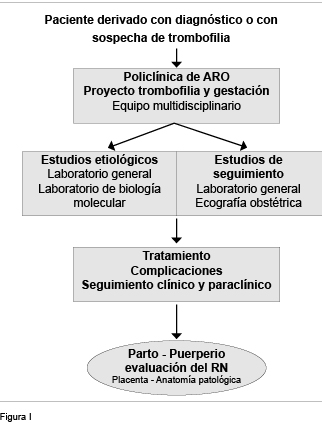
]]> En abril de 2004, se forma el grupo de “Trombofilia y Gestación”. La meta, lograr recién nacidos vivos y sanos. Este grupo trabajó como equipo multidisciplinario en el ámbito de la Policlínica de Alto Riesgo Obstétrico (ARO) del Hospital de Clínicas, con médicos ginecólogos de la Cátedra de Ginecotocología “B” Prof. Dr. Raúl Medina e integrantes del Departamento de Medicina, internistas docentes de las Clínicas Médicas “A” y “B”, hematólogos, personal de enfermería, así como colaboradores del Departamento de Laboratorio Clínico del Hospital de Clínicas y del Departamento Básico de Medicina. Se crea un programa de trabajo (Figura I), integrándose al equipo docentes pertenecientes al Departamento de Métodos Cuantitativos de la Facultad de Medicina de la Universidad de la República (UdelaR).
Objetivos
a) Determinar el tipo de trombofilia y su asociación b) Evaluar complicaciones maternas y perinatales c) Evaluar la vitalidad y el peso de los recién nacidos d) Evaluar las fallas terapéuticas.
MATERIAL y MÉTODOS
]]>
Estudio longitudinal prospectivo, entre abril de 2004 y febrero de 2010. Las pacientes fueron asistidas en la policlínica de ARO del Hospital de Clínicas los días miércoles, por un equipo multidisciplinario integrado por obstetras, hematólogas e internistas, personal de enfermería y de servicio, archivera y dama rosada que trabajan en la policlínica. Control con el equipo de ecografía ginecotocológica, los exámenes complementarios se realizaron por el Departamento de Laboratorio Clínico del Hospital de Clínicas y por Departamento Básico de Medicina de la Facultad de Medicina.
Criterio de inclusión: 1) Antecedentes familiares de patología trombótica con trombofilia conocida o alta sospecha de trombofilia. 2) Antecedentes personales de trombosis 3) Antecedentes personales de complicaciones obstétricas, como las manifestaciones vinculables a trombofilia (MOV): PRE, preeclampsia, eclampsia, RCIU, abortos a repetición, óbito fetal, decolamientos placentarios (DPP). 4) Trombofilia diagnosticada. Se descartaron otras posibles causas de MOV.
Se realizaron los estudios diagnósticos para investigación de tromboflia adquirida: anticuerpos anticardiolipinas (ACA), inhibidor lúpico (IL) y beta2 glicoproteína I (β2GPI) y de trombofilias congénitas MTHFR, FVL, Prot.G20210A; siendo las dosificaciones de ATIII, PC, PS, FVIII realizadas luego de finalizado el puerperio.
Se realizó seguimiento con d-dímeros, ecografía y ecodoppler obstétrico a partir de las 24 semanas de gestación, en forma mensual o según necesidad. No se realizó dosificación de lipoproteína “a” ni de homocisteinemia.
Se realizó tratamiento con HBPM a dosis 3.800 UI a 16.000 UI anti Xa, ácido acetil salicílico y ácido fólico, de acuerdo a pautas preestablecidas basándose en consensos nacionales de trombofilias adquiridas y/o recomendaciones internacionales.
RESULTADOS
]]>
a. De un total de 207 pacientes asistidas que terminaron el embarazo, 90,3% (187/207) tuvieron nacidos vivos. (Figura 2)
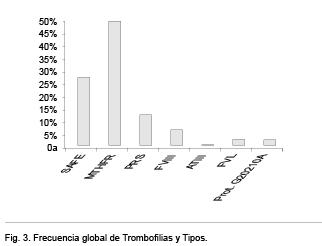
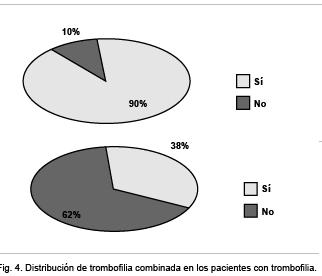
b. Se diagnosticó trombofilia en el 63,3% (131/207), teniendo en cuenta que puede presentarse más de una tipo de trombofilia en la misma paciente y que no se pudieron realizar los estudios etiológicos en todas las pacientes. Se encontró que de las trombofilias estudiadas, las más frecuentes fueron: la SAF en el 27% (51): 15% (29) ACA IgG, 5% (9) ACA IgM, 4% (8) IL, 3% (5) β2GPI y dentro de las trombofilias congénitas estudiadas: la MTHFR en 49,5% (91) (40% he y 9,5% ho), Déficit de Proteína S 12% (22 casos), aumento de FVIII 6% (11 casos), el FVL 2,5% (5) y la mutación del gen de las Protrombina G 20210 A en 2,5% (5) ATIII 0,5% (1) (Figura 3). El 38,2% (50/131) de las pacientes presentaron trombofilia combinada (Figura 4).
c. De las pacientes que culminaron su embarazo, las complicaciones vinculadas a la presencia de una trombofilia fueron: 25% presentaron amenaza de aborto, 18% RCIU, 2,9% Preeclampsia/Eclampsia, 1% DPP. (Figuras 5 y 6). No se presentaron complicaciones hemorrágicas, trombocitopenia inducida por heparina, ni muerte materna. Una paciente que no cumplió con el tratamiento indicado presentó TVP en el puerperio. No existieron complicaciones por sangrados ni trombosis fetales y hubo 3 casos de malformaciones fetales no vinculable a la trombofilia ni al tratamiento.
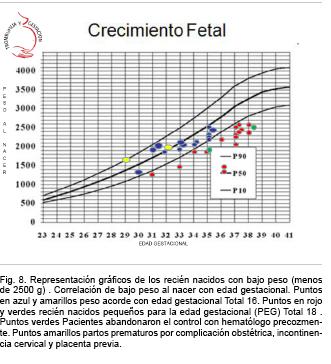
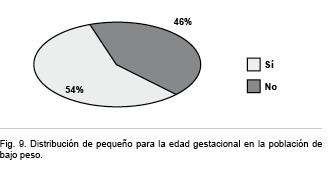
d. Estado de salud del recién nacido. El 90,3% (187/207) fueron recién nacidos vivos. El 81,3% (152 /187) presentó APGAR igual o mayor a 9/9. El peso de recién nacido fue entre 1.032 g y 4.284 g con una media de 2.960 g. Relacionando el peso con la semana gestacional se vió que 81,3% (152/187) fueron > o igual 2.500 g y que el 18,7% (35/187) tuvieron bajo peso al nacer. El 54,3% (18/35) de los de bajo peso fueron Pequeños para la Edad Gestacional (PEG) (Figuras 7, 8 y 9). De los PEG, en dos casos se abandonó precozmente el control y tratamiento con el hematólogo. Dentro de los recién nacidos de bajo peso pero no PEG, 2 fueron prematuros por causa obstétrica: uno por incontinencia de cuello uterino y otro por placenta previa, causas no vinculables a trombofilia.
e. El 9,7% (20/207) fueron resultados adversos: 7,7% (16/207) fueron abortos y 1,9% (4/207) óbitos fetales.
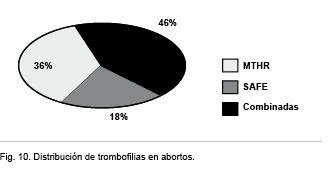
- A 62,5% (10/16) de los abortos se les tipificó trombofilia: 36% (4) MTHR he, 18% (1) SAF, y a los 46% (5) restantes trombofilias combinadas (1 MTHFR con FVL; 2 MTHFR con déficit de PRS; 1 SAFE (IL) con déficit PRS; y 1 MTHFR he con Prot.G20210A) (Figura 10).
- En 100% (4/4) de los óbitos fetales se encontró trombofilia (2 MTHR he; 1 MTHFR ho; y 1 SAF (ACA).
]]>
DISCUSIÓN Y COMENTARIOS
]]>Se diagnosticó trombofilia en 63,3% de las pacientes-; de éstas 38,2% fueron trombofilia combinada. De completarse los estudios etiológicos en todas las pacientes, el porcentaje seguramente sería aún mayor. El dato que casi el 40 % de las pacientes presenten trombofilia combinada nos obliga a realizar una reflexión: cuando tenemos clínica acorde con compromiso vascular placentario es importante estudiar a las pacientes en forma completa pues puede presentar trombofilia combinada(9).
También se diagnosticó trombofilia en todos los óbitos fetales y en el 62,5% de los abortos. Este dato es importante pues de presentarse pacientes con pérdida de embarazo sin causa aparente, deben ser estudiadas en forma completa y así prevenir nuevas pérdidas de embarazo. Resultados similares se observaron en un estudio nacional publicado por la Dra Ana M. Otero en 2004, donde se diagnosticó trombofilia en 65% de la población seleccionada y 20% en la población control (8).
Consideramos como éxito terapéutico el haber logrado un 90,3% de recién nacidos vivos en una población de pacientes seleccionadas por presentar complicaciones obstétricas. El haber tenido 81,3% con buen peso al nacimiento y sólo 18,7% con bajo peso al nacimiento, de los cuales sólo la mitad fueron PEG, nos indica que la terapeútica también favorece el buen crecimiento fetal.
CONCLUSIONES
El tratamiento instituido fue eficaz, lo que quedó demostrado por el elevado porcentaje de recién nacidos vivos con pesos adecuados para la edad gestacional.
Se puede concluir que con control y seguimiento estricto –tanto clínico como paraclínico–, determinando los ajustes necesarios del tratamiento, se obtienen buenos resultados en pacientes con manifestaciones obstétricas vinculables a trombofilia, independientemente de su confirmación.
Agradecimientos
Al personal de enfermería de la Policlínica de Alto Riesgo Obstétrico: Lic. Rubita Neumachinow, Lic. Elida Hernández y todas las licenciadas en enfermería que trabajan en la policlínica, así como las Sras. Magalí Mederos y Angélica Lasida (archivera), cuya colaboración fue muy importante en controles, aspectos psicológicos y en la instrucción para la autoinyección de las pacientes.
Al personal del laboratorio: Licenciados de laboratorio Alicia Olivera, Daniel Raposo y Carmen Trombotti y a las Dras. Rossana Rodriguez, Mitila Robatto, Florencia Sundberg, Prof. Adj. Cecilia Guillermo y Prof. Agda. Graciela Pedreira.
A la Dirección del Hospital de Clínicas, en particular a la Dra. Graciela Ubach y al Dr. Daniel Alonso.
]]>
BIBLIOGRAFÍA
1. J. Gilabert, A. Estellés, F. España, S. Grancha, J. Aznar Modificaciones de la hemostasis en obstetricia. Cuaderno de Trombosis -1997.
2. Stirrat GM. Recurrent miscarriage. Lancet 1990; 336(8716):673-675.
3. E. Pons,AM Otero, R Pou. Consenso Uruguayo sobre SAF del embarazo.Montevideo. Agosto 2002;18-19.
]]>4. Lens D, Brugnini A, Trías N y col. Association between recurrent pregnancy loss and prothrombotic gene polymorphisms. 19th Congress of the International Society of Thrombosis and Haemostasis. Birmingham. UK. 15th July 2003. J Throm Haem 2003;1(Suppl 1 ): 0951.
5. Lens D, Otero AM, Brugnini A y col. Prevalence of factor V Leiden, prothrombin 20210A and the thermolabile MTHFR in the uruguayan population. Poster presentado en el 18th Congress of the International Society of Thrombosis and Haemostasis. París. J Throm Haem July 2001;668.
6. Kupferminc M.,MD,Eldor A,MD, Steinman N,MD, Many A,MD,Bar-Am A, MD,Jaffa A, MD, Fait G, MD, and Lessing J,MD. Increased frequency of genetic thrombophilia in women with complications of pregnancy.January 7, NEJM 1999;340:9.
7. Otero A.M, Pou Ferrari R, Dellepiane M, Muxi P,De Lisa E, Attarian D,Pierri S,Lens D. Pregnancy outcome in women with recurrent pregnant loss treated with enoxaparine. Trombosis and Haemostasis. Suppl. July 2001 SIN 0340-6245.
8. Otero AM,Pou R,Pons E,Lens D y col.Trombofilia y pérdida recurrente de embarazo. Rev.Med Uruguay 2004;20:106-113.
]]>9. Preston FE, Rosendaal FR et al Increased fetal loss in woman with heritable thrombophilia. Lancet 1996; 348:913.
]]>