GUÍAS ESQUEMATIZADAS DE TRATAMIENTO DE LOS TRASTORNOS DE LA PERSONALIDAD PARA PROFESIONALES, DESDE EL MODELO DE YOUNG, KLOSKO Y WHEISHAR (2003)
SCHEMATIC-GUIDES FOR PROFESSIONALS TO TREAT PERSONALITY DISORDERS, FROM THE MODEL OF YOUNG, KLOSKO AND WHEISHAR (2003)
Andrés Fernando López Pell
Universidad Católica de Santa Fe y FUNSALED, Argentina
Jordi Cid Colom
International Society of Schema Therapy
Julio Obst Camerini
UAI y C.A.T.R.E.C.
Juan M. Rondón
Universidad Católica de Santa Fe, Argentina
Silvina M. Alfano
Universidad Católica de Santa Fe, Argentina
Universidad Católica de Santa Fe, Argentina
Resumen: Los tratamientos psicológicos para Trastornos de la personalidad todavía no alcanzan un grado de protocololarización específico como para describir las intervenciones para cada sesión. Esto podría deberse, entre otras cuestiones, a la heterogeneidad de los casos que dificultaría la posibilidad de diseñar un protocolo. Los tratamientos entonces se basan en conceptualizaciones de caso sustentadas teóricamente que después determinan los objetivos y las intervenciones a realizar. La dificultad para conceptualizar desde determinado modelo puede que sea una razón por la que a los psicoterapeutas les costaría realizar el tratamiento más adecuado. Para afrontar este problema hemos construido ‘Guías esquematizadas para profesionales’ para mejorar la práctica clínica. Estas guías son de una carilla para tenerlas a la vista durante las sesiones a fin conceptualizar los casos y guiar más fácilmente las intervenciones desde el modelo de Young, Klosko y Wheishar (2003). Este artículo describe el proceso de construcción de las guías.
Palabras clave: personalidad, trastornos, tratamiento, terapia de esquemas.
Abstract: Psychological treatments for personality disorders have not yet reached a level of protocol as specific as to describe interventions for each session. This could be due, among other factors, to the heterogeneity of cases that make it difficult to design a protocol. Treatments are then based on case conceptualizations supported by theories that determine the objectives and interventions performed. The difficulty to conceptualize from a particular model may be a reason why psychotherapists find problems to make the most appropriate treatment. Addressing this problem, we have designed a set of ‘Professional schematic-guides’ to improve the clinical practice. These one-page-guides were created to have them in front of you during the sessions, and help to conceptualize cases and easily guide the interventions from the model of Young, Klosko y Wheishar (2003). This article describes the process of building guidelines.
Keywords: personality, disorders, treatment, schema therapy.
Recibido: 02/2011
Revisado: 04/2011
Aceptado: 05/2011
Correspondencia: Andrés López Pell. Universidad Católica de Santa Fe (UCSF) y FUNSALED, Argentina. Correo Electrónico: alopezpell@funsaled.org.ar.
Nada ha demostrado ser más eficaz que la aplicación de un protocolo psicoterapéutico científicamente validado. Sin embargo ¿qué hacer cuando el paciente tiene varios trastornos?, o ¿cuándo no hay un protocolo validado para tratar el trastorno que sufre? En tales circunstancias, una opción es basar el tratamiento en una conceptualización de sus problemas guiada por un marco teórico. La dificultad para conceptualizar desde determinado modelo puede que sea una la las tantas razones del por qué a los psicoterapeutas les cueste más seguir las pautas descriptas para el abordaje de estas alteraciones. Otra cuestión de suma importancia es que son pacientes muy difíciles de mantener en tratamiento por lo cual se requiere de mucha flexibilidad por parte del terapeuta. Esto, sumado a la heterogeneidad de los casos, dificulta la posibilidad de diseñar un protocolo de tratamiento de alta especificidad delineado para cada sesión como existe para otros trastornos (e.g., depresivo mayor, de angustia, ansiedad generalizada, etc.) ya que cada tratamiento, si bien es guiado por la misma base teórica, termina adquiriendo una forma particular.
En busca de enfrentar la problemática planteada, en artículos anteriormente publicados en esta revista, propusieron el concepto de Guías esquematizadas para profesionales (López Pell, Rondón, Alfano, & Cellerino, 2010; López Pell, Rondón, Cellerino & Alfano, 2010). En aquella ocasión, las guías se hicieron para los modelos de Theodore Millon y de Beck, Freeman, Davis y otros (2005). En esta oportunidad, utilizando el mismo concepto, se realizarán para el modelo que vienen desarrollando Young, Klosko y Wheishar (2003).
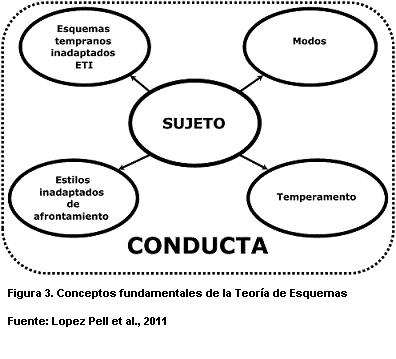
Las Guías esquematizadas para profesionales están diseñadas para mejorar la práctica de la psicoterapia para los trastornos y alteraciones de la personalidad. Fueron realizadas en una carilla cada una con la idea que los psicoterapeutas las tengan a la vista durante las sesiones y que de esta manera puedan conceptualizar sus casos y guiar más fácilmente sus intervenciones. Atento a estas cuestiones, en este artículo se presentan los conceptos centrales que deben guiar la praxis desde el modelo de Young, Klosko y Wheishar (2003) de una manera simple y comprensible a fin de facilitar la transferencia del conocimiento al set psicoterapéutico.
TEORÍA DE LA PERSONALIDAD
Se ha desarrollado en los últimos años dentro del paradigma cognitivo conductual un modelo de abordaje terapéutico denominado Terapia de Esquemas (TE). Ésta es una forma de psicoterapia integrativa, que combina elementos cognitivos, conductuales, psicodinámicos, de las relaciones objetales y humanistas/existenciales (Young, Klosko & Wheishar, 2003). Surge a partir de los conceptos teóricos desarrollados por Beck, especialmente en el área de los trastornos de personalidad, los esquemas, las estrategias y los modos (Alford & Beck, 1997; Beck, 1996; Beck, Freeman, Davis y otros, 2005). La TE ha sido desarrollada por Jeffrey Young (1990; 1993) para tratar a pacientes que reciben un diagnóstico de trastornos de la personalidad o aquellos con problemas psicológicos que se consideran difíciles de tratar, porque suponen un reto desde la perspectiva del terapeuta. La TE se desarrolla para tratar problemas psicológicos graves, arraigados, de larga duración, y que presentan dificultades por generar y mantener la estabilidad sintomática, recaídas constantes, problemas interpersonales o rigidez de patrones conductuales (Young, 1993). Si bien inicialmente fue conceptualizada como una terapia para los Trastornos de la personalidad, en la actualidad se la utiliza y con eficacia para lo que en el DSM-IV TR serían los trastornos del Eje I (American Psychiatric Association, 2002), dentro de los cuales esta ansiedad, depresión, trastornos alimentarios.
1. Dificultades en la identificación de sentimientos y cogniciones. Es bien conocido que las personas con problemas de personalidad bloquean sus emociones y pensamientos. Muchos tienen una tendencia afectiva de evitar las emociones.
2. Problemas para el cumplimiento de las tareas para casa. La colaboración y la motivación para trabajar entre sesión y sesión es difícil de obtener en los TP. Las tareas y/o deberes que se asignan habitualmente en la terapia se tornan de difícil seguimiento.
3. Imposibilidad de definir y clarificar los problemas de la vida. Presentan problemas difusos, vagos que no saben definir como objetivos del tratamiento.
4. Resistencias a una relación terapéutica colaboradora. No es tarea fácil aplicar ni encontrar el empirismo colaborador en el que se fundamenta la terapia cognitiva. Muestran dificultades en sus relaciones interpersonales, tienen problemas para tener una buena alianza terapéutica. En el tratamiento se va a necesitar manejar estas dificultades de manera activa.
Conceptos básicos
Para este modelo de abordaje, Young y Klosko (2007) definen una subcategoría de esquemas: los Esquemas Tempranos Inadaptados (ETI). Estos son patrones disfuncionales -auto-saboteadores- de pensamiento y emoción que se iniciaron en temprana edad y se reiteran a lo largo de la vida. Según esta definición, las conductas inadaptadas no son componentes de los esquemas, sino que son las respuestas a estos. Las conductas son causadas por los esquemas, pero no son parte de los mismos. Sin embargo, Cid (2009) prefiere denominarlos ‘Esquemas Precoces Desadaptativos’, definiéndolos como temas amplios y persistentes formados por recuerdos, emociones, pensamientos y sensaciones corporales que hacen referencia al análisis de uno mismo y de las relaciones con los demás. Estas se originan durante la infancia y se van elaborando a lo largo de la vida del individuo, siendo disfuncionales en grado significativo.
Los ETI se originan en representaciones basadas en la realidad y en su comienzo pueden generar respuestas adaptadas a éstas. Su disfuncionalidad se muestra más tarde en la vida, cuando esas percepciones o apreciaciones ya nos son ajustadas a la realidad. Los mecanismos humanos de supervivencia, en particular el impulso a la consistencia cognitiva -o a evitar la disonancia cognitiva-, generan la poderosa energía que los defiende ante todo intento de modificarlos, forzando a las otras percepciones a ajustarse a ellos (Young & Klosko, 2007).
Pero estos esquemas pueden tener distintos grados de gravedad y de rigidez o resistencia al cambio. La gravedad puede definirse por la cantidad de situaciones que los activan. La mayor o menor severidad y resistencia al cambio dependerán de lo temprano -o tardío- de la edad en que se generaron, de la cantidad de figuras significativas que lo generaron y de la cantidad -o duración- de las situaciones que lo generaron. Por ejemplo, será más severo y rígido un esquema generado por ambos progenitores, desde la edad de 4 o 5 años y durante toda la infancia, que uno generado por un solo progenitor, o solamente por un maestro, en un episodio único, cuando tenía 12 años de edad (Young & Klosko, 2007).
En resumen, las características más relevantes de los ETI son las siguientes:
1. Son verdades a priori acerca de uno mismo y del ambiente, estructuras centrales del auto-concepto.
2. Se auto-perpetúan y son resistentes al cambio; es decir, no se modifican y se mantienen a lo largo del tiempo.
3. Son disfuncionales o desadaptativos: con consecuencias auto-destructivas y/o daño significativo para los demás. Interfieren de forma significativa en la satisfacción de las necesidades nucleares de autonomía, unión con los demás, auto-expresión, límites, gratificaciones y autoestima necesarias para una calidad de vida saludable.
5. Son el resultado de la interacción del temperamento con las experiencias nocivas o interacciones dolorosas y disfuncionales con los miembros de la familia o cuidadores en la infancia.
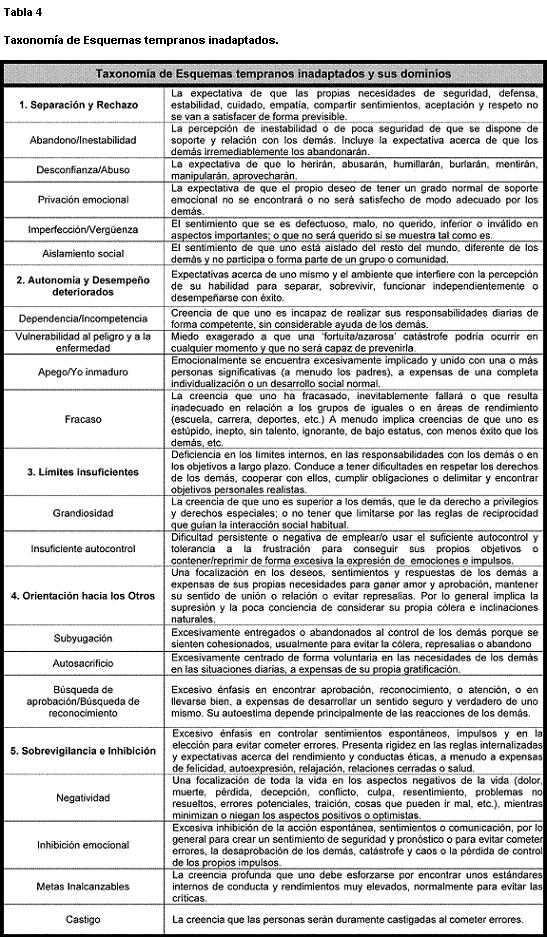
Finalmente, se nombrarán y describirán brevemente los 18 esquemas tempranos inadaptados propuestos por Young y Klosko (2007) que se relacionan con las necesidades básicas que se exponen más adelante, cuando estas no han sido satisfechas adecuadamente. Estos esquemas a su vez se agrupan, en cinco dimensiones o dominios (véase Tabla 4):
1) Desconexión y rechazo
1. Abandono/Inestabilidad. La percepción de inestabilidad o de poca seguridad, de que se dispone de soporte y relación con los demás.
3. Privación emocional. La expectativa de que sus deseos propios de tener un grado normal de soporte emocional (i.e., cuidado, empatía o protección) no se satisfacerán adecuadamente con los otros.
4. Defectuosidad/Vergüenza. El sentimiento que uno es defectuoso, malo, no querido, inferior o inválido en aspectos importantes; o de que uno sería no querido de forma significativa por los demás si se muestra tal como es.
5. Aislamiento social/Alienación. La sensación de que uno está aislado del resto del mundo, diferente de los demás y no participa o forma parte de un grupo o comunidad.
2) Trastornos de autonomía y rendimiento
6. Dependencia/Incompetencia. Creencia de que uno es incapaz de realizar sus responsabilidades diarias de forma competente, sin considerable ayuda de los demás.
7. Vulnerabilidad al peligro. Miedo exagerado a que una ‘fortuita/azarosa’ catástrofe podría ocurrir en cualquier momento y que no será capaz de prevenirla. Los miedos son médicos, emocionales, naturales/fobia.
8. Apego inmaduro independiente. Emocionalmente se encuentra excesivamente implicado y unido con una o más personas significativas -a menudo los padres-, a expensas de una completa individualización o un desarrollo social normal.
9. Fracaso. La creencia de que uno ha fracasado, inevitablemente fallará o que fundamentalmente resulta inadecuado en relación a los grupos de iguales, en áreas de rendimiento (e.g., escuela, carrera, deportes, etc.).
3) Límites insuficientes
10. Grandiosidad. La creencia de que uno es superior a los demás, que le da derecho a privilegios y derechos especiales; o no tener que limitarse por las reglas de reciprocidad que guían la interacción social habitual.
11. Insuficiente autocontrol. Dificultad persistente o negativa de emplear o usar el suficiente autocontrol y tolerancia a la frustración para conseguir sus propios objetivos, o contener/reprimir de forma excesiva la expresión de sus emociones e impulsos.
4) Focalización en los otros
12. Subyugación. Excesivamente entregados/abandonados al control de los demás porque uno se siente cohesionado: usualmente para evitar la cólera, represalias o el abandono. Las dos formas más importantes son la subyugación de necesidades y de emociones.
13. Autosacrificio. Excesivamente centrado de forma voluntaria en las necesidades de los demás en las situaciones diarias, a expensas de su propia gratificación.
14. Búsqueda de aprobación/Búsqueda de reconocimiento. Excesivo énfasis en encontrar aprobación, reconocimiento, o atención en los demás, o en llevarse bien, a expensas de desarrollar un sentido seguro y verdadero de uno mismo. Su autoestima depende principalmente de las reacciones de los demás más que de sus propias inclinaciones naturales.
15. Negatividad -eventos controlables-. Una penetrante focalización de toda la vida en los aspectos negativos de la cotidianeidad, mientras minimizan o niegan los aspectos positivos u optimistas, o una exagerada expectativa de que las cosas saldrán seriamente mal.
16. Inhibición emocional. Excesiva inhibición de la acción espontánea, sentimientos o comunicación, por lo general para crear un sentimiento de seguridad y pronóstico; o para evitar cometer errores, la desaprobación de los demás, catástrofe y caos, o la pérdida de control de los propios impulsos.
17. Metas inalcanzables. La creencia profunda que uno debe esforzarse por encontrar unos estándares internos de conducta y rendimientos muy elevados, normalmente para evitar las críticas.
18. Castigo. La creencia que las personas deben ser duramente castigadas al cometer errores, incluso él mismo.
Orígenes y clasificación de los esquemas
Según este modelo, los ETI se originan en necesidades emocionales insatisfechas en la infancia. Éstas son necesidades básicas que todo niño tiene que tener cubiertas y debe aprender a compensarlas con sus padres, familia y el grupo de pares, con el fin de conseguir un óptimo desarrollo y funcionamiento adaptativo a lo largo de la vida. Estas cinco necesidades universales según Young y Klosko (2007) se enuncian como:
· Pertenencia. Integrada por: Seguridad, Estabilidad, Afecto, cariño, Aceptación
· Autonomía, competencia y sentido de identidad.
· Libertad para expresar emociones y deseos válidos.
· Espontaneidad y juego.
· Límites realistas y autocontrol.
Finalmente, es importante señalar que Young y Klosko, (2007) han observado que existen cuatro tipos de experiencias vitales que promueven la aparición de los esquemas. La primera es la que denominan frustración tóxica de las necesidades que se produce cuando el niño recibe ‘muy poco de algo bueno’ y adquiere esquemas tales como la Privación emocional o Abandono/Inestabilidad, debido a ciertas deficiencias en su ambiente temprano. De esta manera, el ambiente del niño está perdiendo estabilidad, comprensión o amor. El segundo tipo de experiencia tóxica temprana hace referencia a la traumatización; en este sentido, el niño es dañado, criticado, controlado o victimizado. Estas experiencias llevan a que desarrolle esquemas tales como Abuso/Desconfianza, o Vulnerabilidad al peligro. Con respecto al tercer tipo de experiencia tóxica, el niño recibe demasiado de algo bueno, es decir, los padres brindan al niño demasiado de algo que, en moderación, es saludable para él mismo, lo que a su vez contribuye a generar esquemas tales como Dependencia funcional o Grandiosidad. Por último, el cuarto tipo de experiencia tóxica consiste en la interiorización selectiva o identificación con otros significativos. Con respecto a este tipo de experiencia, el niño se identifica de manera selectiva e interioriza los pensamientos, las sensaciones y las experiencias de sus padres, en otras palabras, el niño lo que hace es interiorizar los esquemas de sus padres, lo que da lugar a que se origine, por ejemplo, el esquema de Vulnerabilidad.
Los estilos y respuestas de afrontamiento
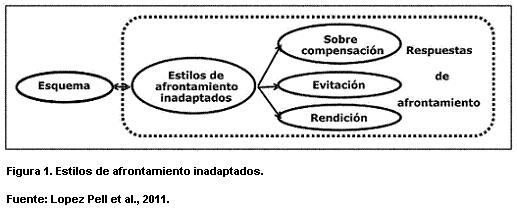
Existen tres estilos desadaptativos de afrontamiento ante la frustración de las necesidades emocionales que mencionamos anteriormente. Se los puede definir como formas de hacer frente a las necesidades básicas, a los conflictos y a las situaciones estresantes, que refuerzan y mantienen a los ETI, y que empiezan de manera temprana para permitir una adaptación a los esquemas, para no experimentar las intensas y arrolladoras emociones que estos engendran (Young & Klosko, 2007). Los tres estilos de afrontamiento desadaptativos hacen referencia a las tres respuestas básicas ante la amenaza: la lucha, la huída y el quedarse inmóvil; específicamente lucha es sobrecompensación, huida es evitación y quedarse inmóvil es rendición. Es importante tener en cuenta que si bien estos estilos de respuesta fueron posiblemente funcionales y útiles en la infancia, en la edad adulta podrían resultar disfuncionales porque no permiten adaptarse de una manera saludable y, por lo tanto, impiden la satisfacción de las necesidades básicas de todos los seres humanos (Young & Klosko, 2007). Los pacientes suelen referirse a estas cosas como ‘lo que nos hacen tropezar una y otra vez, con la misma piedra’. Los tres estilos de afrontamiento descritos por Young y Klosko (2007) son:
1. Sobre-compensación. Hace referencia a conductas, pensamientos y sentimientos con los que el sujeto intenta superar y hacer frente a un esquema. Muchas veces se pueden manifestar como conductas o estilos de funcionamiento totalmente contrarios a los que esperamos según el esquema en cuestión o el esquema predominante. Son intentos parciales de hacerle frente al mismo y a las emociones que generaría su activación, aunque como son excesivos o exagerados, habitualmente terminan en la activación del esquema. Entonces, si una persona fue sometida en la infancia, ahora es desafiante; si fueron controlados, desafían toda forma de influencia sobre ellos; tener un estilo de vida completamente autosuficiente y aparentando que nunca necesita nada, puede ser un intento de compensar sentimientos y creencias de incompetencia.
3. Rendición. Consiste en aceptar plenamente y favorecer el cumplimiento o confirmación del esquema. Los pacientes buscan las relaciones que reiterarán las situaciones generadoras del esquema o reaccionan con excesiva intensidad emotiva ante disparadores del esquema. Por ejemplo, reiteran parejas abusivas o descalificadoras o generan reacciones negativas en otros y responden con exacerbado resentimiento o depresión ante esas reacciones.
Finalmente, se denomina respuestas de afrontamiento a las conductas concretas que se desarrollan de acuerdo a los esquemas y a los estilos de afrontamiento de cada paciente (Young & Klosko, 2007). Para una mejor comprensión de los conceptos antes descriptos, en la Figura 1 se los esquematiza.
Operaciones de los esquemas
Young y Klosko (2007) reagruparon los estilos de afrontamiento desadaptativos en dos operaciones básicas de los esquemas:
1. La perpetuación. Incluye todo lo que hace el paciente (i.e., pensamientos, emociones o conductas) que sostiene y perpetúa al esquema.
2. La sanación. Incluye todo lo que haga el paciente que produzca la disminución de cualquiera de los componentes del esquema. Este sería el objetivo de la terapia, que implica disminuir la intensidad de los recuerdos conectados con el esquema, la carga emocional, la intensidad de las sensaciones corporales y las cogniciones desadaptativas. Esto también conlleva un cambio de la conducta, donde el paciente reemplaza los estilos de afrontamiento desadaptativos por patrones conductuales adaptativos.
Las personas no tienen sus esquemas permanentemente activos, sino que éstos se activan en determinados momentos. A su vez, las personas disponen de diversos estilos de afrontamiento, pero no siempre los están utilizando. Frente a determinados disparadores la persona activa alguno(s) de sus esquemas. A su vez los esquemas activos despliegan alguno de los varios estilos de afrontamiento característicos de la persona, concretado en cada caso en una de las conductas posibles dentro de ese estilo. Sin embargo, podemos observar que ciertos esquemas y estilos de afrontamiento se disparan juntos. A estos esquemas y/o estilos de afrontamiento agrupados se les ha denominado modos (véase Figura 2). Los Modos hacen referencia a partes del sí mismo que contienen ETI y sus respectivos estilos de afrontamiento, los cuales no han sido integrados en una personalidad consistente. Los Modos consisten así en pensamientos, emociones y conductas relacionadas que forman parte de un patrón recurrente en la vida del sujeto. Los Modos son temporales y se activan ante determinados estresares (Young, Klosko & Wheishar, 2003).
Las personas cambian sus modos en diversos momentos y ante diversas circunstancias. Asimismo, el concepto de modos en cierta forma se relaciona con un grado de disociación, siendo sus ejemplos más extremos el trastorno de personalidad múltiple y el trastorno de personalidad límite. Por su parte, las personas saludables, aunque exhiben diferentes modos, estos no son muy diferentes entre sí, generalmente son la combinación de varios, y en ellas el sentido de una única identidad permanece intacto.
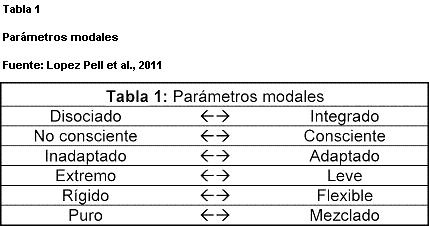
En general podemos decir que los modos en cada persona pueden variar en sus características dentro de los siguientes parámetros (Young & Klosko, 2007) que se presentan en la Tabla 1.
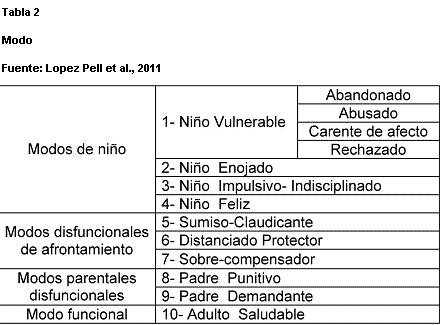
Los 10 modos descriptos por Young y Klosko (2007) se muestran en la 0 2.
Según este modelo, podemos pensar que los Modos de niño son innatos y representan el campo emotivo de los seres humanos (Young & Klosko, 2007). Describirían el estilo emocional del paciente, y se le presupone influencia de variables temperamentales. Si bien los acontecimientos o circunstancias de la infancia pueden reducir, anular o incrementar los modos de niño, todas las personas nacen con la capacidad de manifestarlos.
- El modo Niño Enojado surge como respuesta a la necesidad de un tratamiento justo no obtenido o a situaciones que activan esquemas de abandono, abuso, sometimiento o falta de afecto. En este modo el paciente se enfurece, grita o reacciona violentamente (e.g., el niño que tiene una ‘rabieta’ al no obtener algo).
- El modo Niño Impulsivo o Indisciplinado exhibe poca tolerancia a la frustración o poca capacidad de postergación, realizando cualquier deseo o ‘necesidad’ sin previsión de consecuencias, sin límites ni consideración hacia los demás. Este modo suele aparecer junto con esquemas del dominio III, como el de ‘Derechos/Grandiosidad’ o el de ‘Insuficiente Auto-control o Autodisciplina’.
- El Niño Feliz es el modo propio de una saludable ausencia de activación de esquemas inadaptados.
os Modos de Estilos de Afrontamiento Desadaptativos se entienden como los estilos de afrontamiento que se van aprendiendo para hacer frente a los Modos de niño, y hacen referencia a cómo las personas resuelven las situaciones conflictivas y manejan las emociones asociadas (Young & Klosko, 2007). Asimismo se corresponden con los tres estilos inadaptados de afrontamientos descriptos con anterioridad:
- El modo Sumiso corresponde al estilo ‘rendición’. La persona se muestra pasiva, hace todo lo que otras personas desean que haga y puede ser obediente hasta el grado de permitir el abuso o la descalificación, para conservar la relación o evitar reacciones negativas o venganzas.
- El modo Distanciado corresponde al estilo ‘evitación’. La persona adopta conductas de retraimiento, evitación de situaciones, desconexión de emociones, aislamiento, etc.
- El modo Sobre-compensador corresponde al estilo de ‘sobre-compensación’. En este modo las personas obran como si fuera verdad todo lo opuesto a su esquema inadaptado. Si se creen defectuosos, actúan como perfectos o superiores a otros; si se creen culpables, acusan a los otros.
Los ‘Modos disfuncionales parentales’ surgen cuando el paciente incorpora las conductas disfuncionales de sus padres. Sería la voz internalizada de los padres, que correspondería a enseñanzas o mandatos de los padres que en la vida adulta no permiten una adecuada adaptación. Las dos formas más comunes son:
- El padre demandante, que no castiga sino que pretende la perfección, los máximos niveles de realización, y se desilusiona o se muestra defraudado cuando no se cumplen, generando culpa o vergüenza en el niño.
Estos modos parentales disfuncionales suelen encontrarse en casos de severa depresión y en trastornos obsesivo-compulsivos.
Por último, dentro del ‘Modo funcional’:
- El modo Adulto saludable correspondería a todas las cosas buenas del autoconcepto del paciente, que permite generar una sensación de autoeficacia en las propias habilidades, autoestima para poder avanzar y compasión para poder aceptar las experiencias vitales negativas. En las personas saludables, este modo se activa con mayor frecuencia, está casi siempre presente y tiene fuerza suficiente para moderar a los otros modos cuando aparecen.
El temperamento
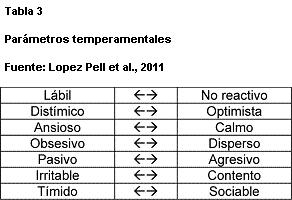
Como ya se hizo referencia, los modos de niño están influenciados por variables temperamentales. En este sentido, cada niño desde su nacimiento tiene un temperamento distinto, una forma innata de reaccionar emotivamente, de origen biológico y muy estable a través de toda la vida o muy difícil de modificar. Este temperamento interacciona con los acontecimientos de la vida, tanto en la determinación de la respuesta ante determinadas situaciones, favoreciendo ciertas emociones y conductas, como en la generación de las mismas situaciones. Asimismo, el temperamento de cada persona puede definirse de acuerdo a siete parámetros en puntos intermedios entre los dos extremos de cada uno.
A su vez, el temperamento influye en el estilo de afrontamiento que cada persona desarrolla ante sus esquemas y es un componente importante en la determinación de la forma en que una persona responderá a su entorno. Un estilo de temperamento no es ni bueno ni malo cada estilo tiene tanto ventajas como desventajas. El temperamento es muy resistente al cambio. Sin embargo, el paciente puede aprender a moderar sus respuestas emotivas y a modificar o hasta suprimir algunas conductas disfuncionales favorecidas por su temperamento (Young & Klosko, 2007).
ESTRATEGIAS DIAGNÓSTICAS
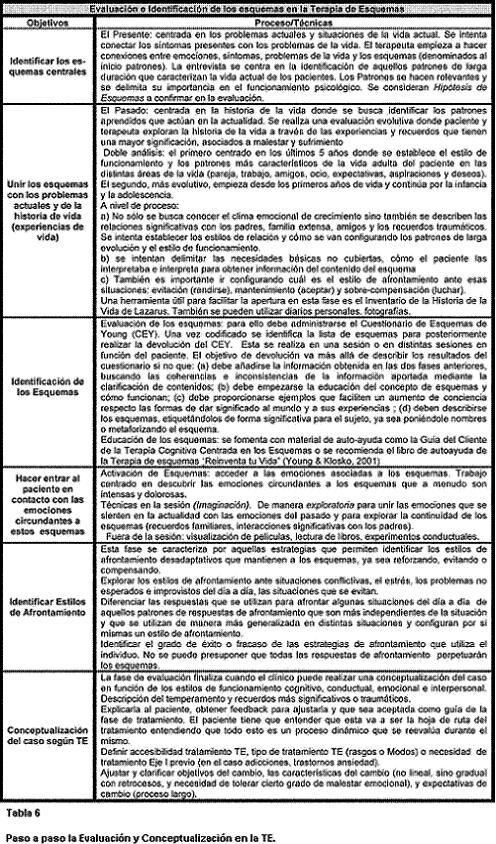
Dentro del tratamiento de los trastornos de personalidad, la primera etapa es la de evaluación, cuyos objetivos según Young (1996) son:
1. Identificar los esquemas centrales de la vida del paciente, hacerlos relevantes en la conciencia, y delimitar su importancia en el funcionamiento psicológico.
2. Unir los esquemas con los problemas actuales y de la historia de vida o experiencial.
3. Hacer entrar al paciente en contacto con las emociones circundantes a estos esquemas.
4. Identificar los estilos de afrontamiento disfuncionales que refuerzan los esquemas.
La evaluación es un proceso de concientización, que implica una construcción conjunta donde terapeuta y paciente identifican cuales son los temas que definen la experiencia -que es dolorosa y que causa sufrimiento emocional-, se acceden a los recuerdos que van configurando las maneras de dar significado al sí mismo -la continuidad y persistencia del sufrimiento-, y se explicitan los estilos de afrontamiento que se utilizan para funcionar en la vida
-consecuencias y refuerzo del sufrimiento-. Para lograr esto, muchos son los recursos con los que se cuenta. Entre ellos, los más frecuentes son:
Los cuestionarios
- Cuestionario de Esquemas de Young (Young Schema Questionnaire, 2001): Es el instrumento más conocido y consiste en un inventario auto-administrado que evalúa qué Esquemas Tempranos Inadaptados tiene probablemente un paciente. Este cuestionario tiene una versión larga -compuesta por 205 ítems- y una versión corta -de 75 ítems- y sus diferentes versiones han sido adaptadas a numerosas lenguas, tales como holandés (Rijkeboer & van den Bergh, 2004), castellano (Cid, Tejero & Torrubia, 1997; Cid & Torrubia, 2003), coreana (Baranoff, Oei, Seong & Seok-Man, 2006), Portugués (Gouveia, Chaves, Oliveira, Dias, Gouveia & Andrade, 2003), etc.
- Inventario de Estilos Parentales de Young (Young Parenting Inventory, 1994b): Inventario auto-administrado de 72 ítems que identifica el origen probable de cada esquema para un paciente en particular.
- Inventario de Evitación de Young y Ryght (Young-Ryght Avoidance Inventory, 1994): Inventario auto-administrado de 40 ítems que mide el grado en que el paciente utiliza diversas formas de evitación del o los esquemas.
- El Inventario de Compensación de Young (Young Compensation Inventory, 1995): Inventario auto-administrado de 48 ítems que mide las formas más comunes que un paciente utiliza para sobrecompensar sus esquemas.
- Historia Multimodal de vida (Lazarus, 2000). Cuestionario auto-administrado que tiene por objetivo la construcción detallada de la historia clínica del sujeto. Se le solicita a la persona que describa conflictos familiares y características vinculares, entre otros hechos de su infancia y adolescencia.
Los ejercicios de imaginación
Los ejercicios en que el paciente revive emotivamente situaciones perturbadoras han demostrado gran utilidad. El generar nuevamente las emociones propias de las situaciones originales, es el recurso más sólido que disponemos para acceder a los pensamientos que las generan (Young & Klosko, 2007). Aunque en el ejercicio la situación no esté sucediendo realmente, las emociones son reales, y si las emociones son reales es porque están presentes las cogniciones que las generan. Dicho en pocas palabras: el ejercicio de imaginación dispara el esquema en el consultorio. Imaginar la situación permite tener la emoción y la cognición correspondientes en la misma sesión y disponibles en ese momento para la observación del terapeuta y el paciente.
En la práctica, esto se puede instrumentar de muchas formas. Por ejemplo, una forma de frecuente utilidad consiste en hacer que el paciente primero reviva en imaginación la situación que le generó la respuesta disfuncional o la emoción disfuncional actual. Luego, se le pide recordar situaciones anteriores, hasta llegar a una experiencia de su infancia en que sintió lo mismo. Esto suele conectar al paciente con la situación traumática que dio origen al esquema temprano inadaptado. El reconocimiento de esa situación, la comparación y diferenciación de la actual, la resignificación de la situación primitiva y otros ejercicios de fuerte contenido emotivo, característicos del psicodrama, suelen superar en eficacia a los simplemente cognitivos tradicionales.
El obstáculo más frecuente a este recurso parece ser el estilo evitativo, que se manifiesta cuando el paciente presenta dificultades, se resiste o ‘no puede’ hacer estos ejercicios (Young & Klosko, 2007). En primer lugar, esta dificultad es útil para conocer su estilo y también puede superarse, lentamente, con la discusión del problema y/o con ejercicios menos comprometidos al comienzo.
Las preguntas y los reportes
Las preguntas directas al paciente y los informes del paciente solicitados y presentados de diversas maneras, son también un recurso válido para conocer su temperamento, sus esquemas, sus modos, estilos de afrontamiento, etc.
La conducta en la terapia
La observación de la conducta del paciente en la terapia, en su relación con el terapeuta, en las tareas asignadas, etc. es otra forma natural y válida de conocer su temperamento, sus esquemas, sus modos, estilos de afrontamiento, etc. Su relación con el terapeuta muestra sus modos, de la misma manera que puede mostrar los modos del terapeuta.
La historia del paciente, los hechos que le sucedieron, la forma en que reaccionó, cómo reaccionaron los otros, incluyendo los principales acontecimientos de su infancia, y especialmente los traumáticos, son otra forma posible de acceder a sus esquemas, modos, etc. Por eso, esta es una información importante en esta etapa.
Otros recursos
Existen muchos recursos posibles, ya que el modelo no descarta ninguno. Entre otros posibles, se encuentra el relato -o representación- de los sueños, especialmente los reiterados y/o con mucho contenido emotivo. El contenido de la Tabla 6 servirá para poder integra estos recursos a la conceptualización del caso.
SÍNTESIS DEL TRATAMIENTO PROPUESTO POR YOUNG, KLOSKO Y WHEISHAR (2003)
Luego de haber llevado a cabo, junto con el paciente, una adecuada evaluación de los aspectos centrales antes planteados, tendrá lugar una segunda fase denominada proceso de cambio (Young & Klosko, 2007). Esta etapa tiene como objetivo principal de tratamiento un cambio en los esquemas y estilos de afrontamiento identificados, lo que significaría en mayor o menor grado: (a) un cambio en la forma de verse a sí mismo; (b) una consecución de unos patrones de vida más flexibles -modificación de estilos de afrontamiento-; (c) una adaptación más óptima a su medio y (d) una disminución del malestar psicológico. Esto implica, por lo general, utilizar diferentes estrategias según los diferentes componentes de los esquemas. Para ello, el terapeuta despliega una amplia gama de técnicas y recursos que debe intentar mezclar de una forma flexible y creativa, de acuerdo a cada caso y paciente en particular. Estas técnicas y recursos, hacen referencia a estrategias cognitivas, experienciales, conductuales, e interpersonales que se describen a continuación:
Las Estrategias Cognitivas
Según lo expuesto por Young y Klosko (2007) el objetivo de la utilización de estrategias cognitivas es desarrollar una voz saludable para crear una distancia. Es decir, se trata de poner a prueba lo inadecuado del esquema desde la distancia cognitiva. Para ello es necesario conocer qué experiencias están asociadas al esquema aportando evidencias que mantienen al mismo. Las técnicas que se utilizan mayoritariamente provienen de la terapia cognitiva, siendo las más utilizadas:
Revisar las evidencias o argumentos a favor y en contra del esquema. Hacer las listas de ellas y discutirlas.
Discutir y evaluar nuevas interpretaciones posibles de las evidencias presentadas a favor del esquema, de acuerdo a puntos de vista más maduros y amplios.
Role-play de diálogos entre el ‘lado del esquema’ y el ‘lado sano’, cambiando roles con el terapeuta.
Escribir y disponer de tarjetas de afrontamiento (i.e., flashcards) donde se pueden leer los argumentos y pensamientos apropiados para enfrentar el esquema cuando se activa.
Utilizar el Registro Diario de Esquemas (Young, 1993) donde el paciente registra los siguientes datos: disparador, emoción, pensamiento, conducta real, esquemas, punto de vista saludable, consideraciones realistas, sobre-reacciones, conducta saludable.
Las Estrategias Experienciales
Técnicas de imaginación -o dramatizaciones-:
Las actuaciones, usando los recursos del psicodrama (Moreno, 1975) (Blatner, 1996) (Blatner & Blatner, 1988) permiten la implicación emotiva necesaria para actuar sobre los esquemas.
- Diálogos. Pueden ser con las personas que originaron sus esquemas disfuncionales. Además, puede ser útil para expresar sentimientos, por ejemplo, la ira puede servir para confirmar sus derechos, pero en un segundo paso se recomienda seguir con este recurso para lograr la integración, la comprensión de la situación, la liberación de la culpa y mejorar el nivel de auto estima del paciente.
- Re-actuación parental. En esta estrategia, el terapeuta solicita entrar en la escena imaginada y así brinda la contención o reparación desde el lugar del padre o simplemente desde el ‘adulto saludable’. Luego lo hará el mismo cliente, intercambiando roles, inicialmente con la ayuda del terapeuta. Estos diálogos del paciente ‘niño’ con el paciente ‘adulto’, o del paciente con ‘el anciano sabio’ han sido largamente utilizados por el psicodrama y por otras escuelas como la gestalt, durante más de 50 años con excelentes resultados.
- Modificación de patrones. Imaginarse actuando en formas alternativas, diferentes a sus pautas disfuncionales es una preparación, un ensayo de menor riesgo, para poder hacerlo luego con mayor nivel de riesgo en la vida real. Primero la imaginación, luego la dramatización y finalmente la vida real, son grados crecientes de ‘riesgo’ para lograr vencer progresivamente el miedo a las nuevas conductas.
Otras tareas y técnicas
- Escribir una carta. Una técnica experiencial frecuentemente útil es escribir una carta -o varias- a uno de los padres o a la persona que haya generado la situación traumática o el esquema temprano inadaptado. La carta podría incluircómo se sintió el cliente ante esas situaciones y lo que no pudo decir. Es un ejercicio menos difícil que la fantasía de estar enfrente a la persona y suele brindar similares beneficios. Esto no incluye, y en general no se recomienda, enviar la carta realmente a la persona, a menos que se hayan evaluado bien las posibles consecuencias y asegurado de que serán positivas -lo cual es poco probable en la mayoría de los casos-, y porque el objetivo se logra sin necesidad de esto.
Más opciones: Medicación, trabajo corporal, etc.
Cuando se encuentran dificultades, se puede recurrir a recursos adicionales, como la medicación para disminuir
-pero nunca suprimir- la ansiedad ante las nuevas tareas. También hay muchos recursos como las técnicas de relajación y otros propios de las técnicas corporales, desarrollados por la terapia gestalt (Kepner, 1987), por el análisis de la relación (Lapierre & Aucouturier, 1990), y por otras escuelas, que pueden ser útiles con ciertos pacientes para ayudar al proceso de cambio requerido en esta etapa.
Las estrategias conductuales
Luego de realizados los pasos anteriores, el terapeuta se avoca a modificar los patrones de conducta o estilos de afrontamiento inadaptados que perturban al cliente. En esta etapa se trabajará para modificar las conductas disfuncionales pertenecientes a los estilos de rendición, evitación o sobre-compensación del paciente, para que puedan ser reemplazados por estilos de afrontamiento más saludables.
Cuando el terapeuta considera que su cliente ha aprendido a reconocer sus esquemas inadaptados cuando son disparados, a entender sus orígenes y a entablar con ellos las discusiones para vencerlos, racional y emotivamente, puede entonces encarar esta etapa final de modificación de sus respuestas inadaptadas, la cual se lleva a cabo de la siguiente manera:
- Elegir la conducta a modificar. Ordenadamente se decidirá cuál será la primera conducta a abordar en primer lugar. Como guía general se recomienda elegir primero una conducta claramente determinada, en vez de plantear ‘cambios generales de vida’. También es aconsejable comenzar con la que mayores problemas cause al cliente, la que más interfiere con sus metas o deseos, la que mayores deseos o motivos tenga para cambiar. Esto siempre que no resulte demasiado difícil o extenuante para este cliente el trabajo de modificarla.
- Generar la motivación necesaria. Sin la motivación necesaria el paciente no realizará el esfuerzo. Para lograrla paciente y terapeuta pueden trabajar en realizar una lista de ventajas y desventajas de seguir con la misma conducta y de cambiar la conducta.
- Implementar los recursos de cambio más eficaces. Para este proceso existen todos los recursos conocidos y habituales de las terapias cognitivas conductuales. Algunos de los más eficaces suelen ser: las tarjetas de afrontamiento (i.e., flash cards), el ensayo de la nueva conducta en ejercicios de imaginación -o en dramatizaciones-, la asignación permanente al final de cada sesión de tareas a realizar y la revisión de la realización de esas tareas al comienzo de la siguiente sesión.
- Trabajar con los obstáculos. Cuando el paciente no hace las tareas, lo fundamental es investigar los motivos para vencerlos. Puede haber causas externas, como acontecimientos imprevistos, una planificación poco clara o precisa, tareas excesivamente difíciles, etc. Pero también puede haber causas internas, como pensamientos, supuestos, esquemas, etc. del paciente referentes a la tarea, a la terapia o a sí mismo que fueron subestimadas o no tenidas en cuenta.
Si la causa es externa, corresponde modificar la tarea, hacerla menos difícil para ir paso a paso, o bien reemplazarla por otra. En algunos casos, si la modificación de la conducta elegida resulta demasiado difícil en esta etapa, o si no se puede lograr suficiente motivación para el esfuerzo de cambiarla, puede elegirse comenzar por otra conducta, dejando la anterior para más adelante.
Finalmente, cabe mencionar que para modificar las conductas disfuncionales, se utilizarán estrategias que provienen de las técnicas de la terapia de conducta tales como: entrenamiento en relajación, entrenamiento en asertividad, estrategias de autocontrol, exposición graduada a las situaciones temidas, etc.
Las estrategias interpersonales
La relación terapéutica es un elemento de gran importancia en este tipo de trastornos. Young et al (2003) consideran que en la relación terapeuta-paciente de la Terapia de los Esquemas hay dos elementos característicos:
- La confrontación empática. Debatir los conceptos y puntos de vista del paciente desde un punto de vista empático, entendiendo sus motivos, sintiendo lo que él siente, ‘poniéndonos en su lugar’. Es decir, la confrontación empática implica expresar la comprensión de las razones por las que mantienen el esquema los pacientes, mientras que simultáneamente se les confronta la necesidad de cambio.
- La re-actuación parental limitada. Actuar en la forma que hubiera necesitado ese paciente que actúen sus padres y cuya falta consideramos que es la causa de sus esquemas disfuncionales. En otras palabras, brindarle al paciente dentro de la relación terapéutica las necesidades emotivas insatisfechas de la infancia causantes de sus esquemas tempranos inadaptados. En este sentido, puede decirse que el terapeuta se convierte en una figura parental transitoria, pero distinta a la original con respecto a las características causantes del trauma. El terapeuta tratará de actuar de manera claramente diferente a la causante del esquema., tratando así de desarrollar antídotos ante la activación de los esquemas. Finalmente cabe aclarar que hay que estar preparado para la hostilidad del paciente, el criticismo, los enfados, la desgana, la inhibición, etc.
En síntesis, la fase de cambio es un proceso centrado en la relación terapéutica, en el cual se intenta crear una cierta distancia, primero cognitiva y después emocional, que permita realizar una re-valoración del sí mismo o autoconcepto, y a su vez, dé lugar al aprendizaje y uso de estrategias que posibiliten un manejo emocional y conductual de las necesidades de la persona que le permitirá una mejor adaptación interpersonal, familiar y social.
GUÍAS ESQUEMATIZADAS PARA PROFESIONALES PARA LOS TRASTORNOS DE PERSONALIDAD DESDE LA TERAPIA DE ESQUEMAS
Los tratamientos psicológicos para los Trastornos de la personalidad todavía no alcanzan un grado de protocololarización tan específico como para describir las intervenciones para cada sesión. Esto podría deberse, entre otras cosas, a la heterogeneidad de los casos que dificultaría la posibilidad de diseñar un protocolo. Los tratamientos entonces se basan en conceptualizaciones de caso sustentadas teóricamente que después determinan los objetivos y las intervenciones a realizar. La dificultad para conceptualizar desde determinado modelo puede que sea una razón por la que a los psicoterapeutas les costaría realizar el tratamiento más adecuado. Para afrontar este problema hemos diseñado unas ‘Guías esquematizadas para profesionales’ para mejorar la práctica de la psicoterapia para los trastornos y alteraciones de la personalidad. Estas guías son de una carilla para tenerlas a la vista durante las sesiones a fin conceptualizar los casos y guiar más fácilmente las intervenciones desde este modelo.
La Terapia de Esquemas define las intervenciones terapéuticas en los Trastornos de la Personalidad (TP) en base a una conceptualización del caso idiosincrásica para cada paciente, que se basa en la identificación de los esquemas precoces desadaptativos y los estilos de afrontamiento desadaptativos. El objetivo de las intervenciones en la TE es la curación de los esquemas, esto implica por un lado, disminuir la intensidad de los recuerdos conectados con el esquema, la carga emocional, la intensidad de las sensaciones corporales, y las cogniciones que llevan a sesgos cognitivos; y por otro lado, un cambio de la conducta, donde el paciente reemplaza aquellos estilos de afrontamiento disfuncionales por patrones conductuales más adaptativos.
La estructura del de este apartado se basa, en primer lugar, en la identificación de las estrategias de intervención paso a paso de la TE en los TP en el modelo original o donde los esquemas se trabajarían según un modelo de rasgos de personalidad (Young, 1990; 1994a; 2003) y que es aplicable a los TP, que en el DSM-IV TR (APA, 2002) están organizados en el Cluster A y C, y al TP Histriónico y Antisocial (i.e., trabajar sobre ciertos patrones predominantes en cada personalidad). En segundo lugar, se intentará definir los aspectos clave de la evaluación y la intervención de la TE para cada trastorno. Antes de continuar, es importante señalar que este aspecto se opone a la propuesta de la TE ya que lo interesante del modelo de esquemas es que realiza una aproximación basada en los elementos internos y subjetivos de la personalidad y rehúye del diagnóstico de TP. Es sabido que el diagnóstico de TP está fundamentalmente basado en el repertorio conductual que muestra la persona a lo largo de la vida, que presenta problemas de fiabilidad y que difícilmente guía a la intervención psicológica. Por lo tanto, este punto debe considerarse de manera pragmática, como una herramienta tentativa en formato de guía esquematizada para profesionales. La excepción será con respecto al TP Límite (Arntz & van Genderen, 2009) y Narcisista (Behary, 2008) donde se realizará la guía en base a los modos o estados de ánimo de Esquemas y donde la propuesta de intervención será más consistente al haber estudios empíricos (Giesen-Bloo, van Dyck, Spinhoven, van Tilburg, Dirksen, van Asselt, Kremers, Nadort & Arntz, 2006; Nadort, Arntz, Smit, Giesen-Bloo, Eikelenboom, Spinhoven, van Asselt, Wensing & van Dyck, 2009; Nadort, van Dyck, Smit, Giesen-Bloo, Eikelenboom, Wensing, Spinhoven, Dirksen, Bleecke, van Milligenese, van Vreeswijk & Arntz, 2009) y de casos clínicos que avalan la intervención en los modos esquemas.
Estructura y las estrategias de interveción Estructura y las estrategias de intervención generales de la TE en los TP
El modus operandi de la TE en la evaluación e identificación de los esquemas (ver Tablas 1, 2 y 3) es un proceso de concientización que implica una construcción conjunta donde terapeuta y paciente identifican cuáles son los temas que definen la experiencia (i.e., que es dolorosa y que causa sufrimiento emocional), se acceden a los recuerdos que van configurando las maneras de dar significado del sí mismo (i.e., la continuidad y persistencia del sufrimiento) y se explicitan los estilos de afrontamiento que se utilizan para funcionar en la vida (i.e., consecuencias y refuerzo del sufrimiento). La evaluación termina con la conceptualización del caso que se comparte con el paciente y se identifica la idoneidad de una intervención basada en esquemas y del tipo de intervención: modelo original de rasgos o modos de esquemas. En el caso de los TP del Cluster A y C del DSM-IV TR (2002), utilizaremos los modos de esquemas cuando hay un estilo rígido de afrontamiento evitativo o compensatorio, criticismo y autolesiones, confusión como consecuencia de los conflictos internos y fluctuación muy rápida de estados de ánimo y estilos de afrontamiento (Young, 1996). El trabajo de identificación de los modos de Esquemas es más emocional y la intervención tiene que ver con el proceso de manejo de las emociones y de atribución de significados idiosincrásicos desadaptativos en el aquí y ahora (Cid, 2008).
La fase de cambio (ver Tabla 4) es un proceso donde, centrándose en la relación terapéutica, se intenta crear cierta distancia, primero cognitiva y después emocional que permita realizar una revaloración del sí mismo o autoconcepto que permita el aprendizaje y el uso de estrategias para lograr un manejo emocional y conductual de las necesidades de la persona que permitirán una mejor adaptación interpersonal, familiar y social. En el caso del modelo de rasgos, el orden de estrategias de intervención va a ser primero estrategias de cambio cognitivas, después experienciales y conductuales. Las estrategias de relación terapéutica estarán presentes desde el inicio y se utilizarán en la activación de los esquemas, para poder trabajar en la sesión el impacto de éstos en el paciente y el terapeuta. Conviene resaltar el buen uso de la confrontación empática y la re-actuación parental limitada, como se ha explicado en los apartados introductorios.
Terapia de esquemas para los trastornos de personalidad y el intento de protocolarizarla mediante las guías esquematizadas para profesionales
Tal como hemos especificado en la introducción, es un ejercicio arriesgado realizar una aproximación de la TE trastorno por trastorno. Ya que ésta rehúye del diagnóstico de TP (i.e., categorial o dimensional) e intenta operacionalizarlos en función de esquemas, estilos de afrontamiento desadaptativos y modos de esquemas, en base a la experiencia subjetiva de la persona y del proceso de atribución de significados cognitivo-emocionales que presenta. El modelo de trabajo que se ha propuesto para los TP permite flexibilizar y adaptar las intervenciones a cada trastorno y sobretodo al hecho de que es frecuente encontrar en la clínica cotidiana diagnósticos comórbidos de Trastornos de la Personalidad o diagnósticos mixtos. No obstante, la TE a diferencia de otros modelos de psicoterapia ha desarrollado una serie de cuestionarios como el Cuestionario de Esquemas que permite no sólo evaluar clínicamente los constructos que propone el modelo y realizar una evaluación de resultados de la intervención, sino que permite la realización de investigaciones para poner a prueba las propuestas teóricas que van surgiendo de la asociación de esquemas, estilos de afrontamiento y modos de esquemas para cada TP.
Para diseñar las guías esquematizadas para profesionales se ha seguido el procedimiento que se explica a continuación. Para cada TP se han analizado los resultados de las investigaciones realizadas con los Cuestionarios de Esquemas (i.e., en su versiones original y la reducida). Así, en función de los resultados, se describirán los esquemas encontrados en base a resultados de investigación. En los casos en que no se han encontrado resultados empíricos, se describen las propuestas teóricas realizadas por diferentes autores que también se dedicaron al tema de los esquemas en cada Trastorno de la Personalidad. Puede consultarse para más detalles los trabajos de Bernsteisn (2002), Sperry (2006) y Arntz y Van Genderen (2009). Respecto a los Modos de Esquema cabe realizar una aclaración, la investigación en este campo está en sus fases iniciales, la mayoría de los resultados son producto de análisis de correlación entre los Modos de Esquemas y los Trastornos de la Personalidad, evaluados mediante entrevistas estructurada para los TP (Lobbestael, Van Vreeswijk & Arntz, 2007; Lobbestael, Van Vreeswijk & Arntz, 2008). Se incluyen los resultados encontrados en las primeras investigaciones debido a que pueden ser de mucha utilidad en el manejo de los casos.
A partir de lo recopilado por los distintos autores citados en cada una de las guías esquematizadas que se presentan seguidamente, se decidió describir, dentro del Cluster A, el Esquema de Desconfianza/Abuso para el Trastorno de Personalidad Paranoide, el Esquema de Aislamiento Social para el TP Esquizoide, y los Esquemas de Desconfianza/Abuso y Vulnerabilidad al Peligro para el TP Esquizotípico. Dentro del Cluster B, para el TP Histriónico, los esquemas de Privación Emocional y Grandiosidad. En el TP Antisocial, los esquemas de Privación Emocional y Insuficiente Autocontrol. En el TP Límite y TP Narcisista describiremos la fase de cambio basada en los Modos de Esquemas. En el Cluster C, describiremos en el TP Evitativo, los Esquemas de Imperfección, Fracaso y Subyugación. En el TP Dependiente el esquema de Abandono y Dependencia.
En el TP Obsesivo Compulsivo describimos el cambio en los esquemas de Inhibición Emocional y Metas Inalcanzables. En el TP Pasivo-Agresivo describimos el cambio de Desconfianza y Fracaso.
CONCLUSIONES
En síntesis, son muchas las razones por las que son dificultosos los abordajes psicológicos para los Trastornos de la personalidad. La dificultad de protocololarización es sólo una de ellas. Los aportes de Young, Klosko y Wheishar constituyen sin duda una propuesta teórica, con desarrollo de tecnología -tanto para la evaluación como para la intervención- para la praxis clínica con este tipo de pacientes.
La Terapia de esquemas es un tratamiento que partiendo de una conceptualización de caso brinda el sustento para determinar objetivos realistas y dispone de un bagaje de intervenciones para alcanzarlos. En este sentido las ‘Guías esquematizadas para profesionales’ están diseñadas para facilitar la tarea de terapeuta y constituyen un humilde aporte para facilitar la aplicación de la misma.
Es importante aclarar que tanto los trabajos de Tineo y Young (2006) y Tineo, Alén, Chajét, Chajét y Sá (2006); como los de Cid y Torrubia (2003), Cid (2009) y Cid, Tejero y Torrubia (1997) son un gran aporte a la difusión y desarrollo de la Terapia de esquemas en lengua hispana y nos apoyamos en ellos para la realización de esta propuesta.
Addington, J. & Tran, L. (2009). Using the Brief Core Schema Scales with Individuals at Clinical High Risk of Psychosis. Behavioral and Cognitive Therapy. 37 (2),227-231.
Alford, B. & Beck, A.T. (1997). The Integrative Power of Cognitive Therapy. New York: Guilford Press.
American Psychiatric Association (2002). DSM-IV-TR: Manual diagnóstico y estadístico de los trastornos mentales (Texto revisado). Barcelona: Masson.
Arntz, A. & van Genderen, H. (2009). Schema Therapy of Borderline Personality Disorder. Chichester: Wiley.
Arntz, A. (2008). Schema-focused therapy for borderline personality disorder: effectiveness and cost-effectiveness, evidence from a multicenter trial. European Psychiatry, 23 (2),65-66.
Ball, S.A. & Cecero, J.J. (2001). Addicted patients with personality disorders: Traits, schemas, and presenting problems. Journal of Personality Disorders, 15 (1),72-83.
Baranoff, J., Oei, T., Seong, H.C. & Seok-Man, K. (2006). Factor structura and internal consistency of the Young Schema Questionnaire (Short Form) in Korean and Ausltralian samples. ISAD, 93 (1),133-140.
Beck, A.T. (1996). Beyond belief: A theory of modes, personality, and psychopathology. En P. Salkovskis (Ed), Frontiers of Cognitive Therapy (pp. 1-25). New York: Guilford Press.
Beck, A.T., Freeman, A., Davis, D.D. y otros (2005). Terapia cognitiva de los trastornos de personalidad. Buenos Aires: Paidós Ibérica.
Behary, W.T. (2008). Disarming the narcissist: surviving & thriving with the self-absorbed. Oakland, CA: New Harbinger Publications.
Bernstein, D.P. (2002). Cognitive therapy of Personality Disorders in Patients with histories of Emocional Abuse or Neglect. Psychiatric Annals, 32 (10),618-628.
Blatner, A. & Blatner, A. (1988). Foundations of Psychodrama. History, Theory, & Practice. (3° edición). New York: Springer Publishing Company.
Blatner, A. (1996). Acting-in. Practical Applications of Psychodramatic Methods. (3° edición). New York: Springer Publishig Company.
Cid J. & Torrubia R. (2003). What are the clinical meaning and implications for treatment of the schemas assessment using the Schema Questionnaire?. Revue Francophone de clinique comportementale et cognitive, 8 (1),15-25.
Cid, J. (2009). La Terapia de Esquemas. En: L. Fernández de la Cruz L, M.A. Fullana & O. Andión. Actualizaciones de la Societat Catalana de Recerca i Teràpia del Comportament.
Cid, J., Tejero, A., & Torrubia, R. (1997). Adaptación española del Cuestionario de Esquemas de Young (Spanish version of the Young Schema Questionnaire). Manuscrito no publicado.
French, P. & Morrison, A.P. (2004). Early Detection and Cognitive Therapy for People at High Risk of Developing Psychosis: A Treatment approach. New York: John Wiley.
Giesen-Bloo J., van Dyck R., Spinhoven P., van Tilburg W., Dirksen C., van Asselt T., Kremers I., Nadort M., & Arntz A. (2006). One-Year Follow-up of Schema focused therapy and Transference focused psychotherapy for BPD, and the influence of drop-out status, treatment status and medication. Crossing Borders: Theory, Assessment and Treatment in Borderline Personality Disorder, 127-142.
Giesen-Bloo J., van Dyck R., Spinhoven P., van Tilburg W., Dirksen C., van Asselt T., Kremers I., Nadort M. & Arntz A. (2006). Outpatient psychotherapy for borderline personality disorder: randomized trial of schema-focused therapy vs transference-focused psychotherapy. Arch Gen Psychiatry, 63 (9),649-658.
Gouveia, V.V., Chaves, S.S.S., Oliveira, I P., Dias, M.R., Gouveia, R.S.V., & Andrade, P.R. (2003). A utilização do QSG-12 na população geral: Estudo de sua validade de construto. Psicologia: Teoria e Pesquisa, 19 (13),241-248.
Gude, T., Hoffart, A., Hedley, L., & Rø, Ø. (2004). The dimensionality of dependent personality disorder. Journal of Personality Disorders, 18,(6),604-610.
Kepner, J. (1987). Proceso corporal: Un enfoque Gestalt para el trabajo corporal en psicoterapia. México: El Manual Moderno.
Lapierre, A. & Aucouturier, B. (1990) El cuerpo y el Incosnciente en Educación y Terapia. México: Científico-Médica.
Lobbestael, J., Vreeswijk, M.F. van, & Arntz, A. (2008). An empirical test of schema mode conceptualisations in personality disorders. Behaviour Research and Therapy, 46 (7),854-860.
Lobbestael, J., Vreeswijk, M.F. van, & Arntz, A. (2007). Shedding light on schema modes: a clarification of the mode concept and its current research status. Netherlands Journal of Psychology, 63 (3),69-78.
Loper, A.B. (2003). The relationship of maladaptive beliefs to personality and behavioral adjustment among incarcerated women. Journal of Cognitive Psychotherapy, 17 (3),253-266.
López Pell, A.F., Rondón, J.M., Cellerino, C. & Alfano, S.M. (2010). Guías esquematizadas de tratamiento de los Trastornos de la personalidad para profesionales, desde el modelo de Beck, Freeman, Davis y otros (2005). Revista Ciencias Psicológicas, 4 (1),97-124.
López Pell, A.F., Rondón, J.M., Alfano, S.M. & Cellerino, C. (2010). Guías esquematizadas de tratamiento de los Trastornos de la personalidad para profesionales, desde el modelo de Theodore Millon. Revista Ciencias Psicológicas, 4 (2),239-271.
Nadort, M., Arntz, A., Smit, J.H., Giesen-Bloo, J., Eikelenboom, M., Spinhoven, P., van Asselt, T., Wending, M. & van Dyck, R. (2009). Implementation of outpatient schema therapy for borderline personality disorder with versus without crisis support by the therapist outside office hours: A randomized trial. Behaviour Research and Therapy, 47 (11),961-973.
Nadort, M., van Dyck, R., Smit, J.H., Giesen-Bloo, J., Eikelenboom, M., Wensing, M., Spinhoven, P., Dirksen, C., Bleecke, J., van Milligen, B., van Vreeswijk, M. & Arntz, A. (2009). Three preparatory studies for promoting implementation of outpatient schema therapy for borderline personality disorder in general mental health care. Behaviour Research and Therapy, 47 (11), 938-945.
Obst Camerini, J. (2000). El Psicodrama Cognitivo Conductual. Bs. As.: CATREC.
Obst Camerini, J. (2008). La Terapia Cognitiva. Integrada y actualizada. Buenos Aires: CATREC.
Rijkeboer, M. M., van den Bergh, H. & van den Bout, J. (2005). Stability and discriminative power of the Young Schema-Questionnaire in a Dutch clinical versus non-clinical population. Journal of Behavior Therapy and Experimental Psychiatry, 36 (2),129-144.
Simos, G. (2002). Cognitive Behavior Therapy: A Guide for the Practicing Clinician, East Sussex: Brunner-Routledge. Philadelphia, PA: Taylor & Francis.
Sperry, L. (2006). Cognitive behavior therapy of DSM-IV-TR personality disorders: Highly effective interventions for the most common personality disorders (Second edition). New York: Routledge.
Tineo, Lydia (1997). El proceso terapéutico en la terapia centrada en esquemas. En Caro, Isabel (1997). Manual de Psicoterapias Cognitivas. Barcelona: Paidós.
Tineo, Lydia (2008). Trastorno Borderline. Revista de la Asociación de Psicoterapia de la República Argentina, Año 1 (2).
Young, J. & Brown, G. (2001). Young Schema Questionnaire. New York: Schema Therapy Institute.
Young, J. & Klosko, J. (2007). Terapia de esquemas. En J.M. Oldham, A.E. Skodol & D.S. Bender (Eds), Tratado de los trastornos de la personalidad (pp. 289-308). Barcelona: Elsevier Masson.
Young, J. & Ryght, J. (1994). Young-Ryght Avoidance Inventory. New York: Cognitive Therapy Center of New York.
Young, J. (1990). Cognitive therapy for personality disorders: a schema -focused approach. Sarasota-. Fl.: Professional Resource Exchange, Inc.
Young, J. (1993). The Schema Diary. New York: Cognitive Therapy Center of New York.
Young, J. (1994a). Cognitive Therapy for Personality Disorders: A Schema Focused Approach (Revised Edition). Sarasota, FL: Professional Resource Exchange.
Young, J. (1994b). Young Parenting Inventory. New York: Schema Therapy Institute.
Young, J. (1995). Young Compensation Inventory. New York: Cognitive Therapy Center of New York.
Young, J. (1999). Cognitive therapy for personality disorders: A schema focused approach (3 ed.). Sarasota, FL: Professional Resource Press.
Young, J., Klosko, J. & Weishaar, M. (2003). Schema Therapy. A Practitioner’s Guide. New York: Guilford Press.
Young, J., Wattenmaker, D. & Wattenmaker, R. (1996). Schema Therapy Flashcard. New York: Cognitive Therapy Center of New York.
Para citar este articulo: López Pell, A.F., Cid Colom, J., Obst Camerini, J., Rondon, J. M., Alfano, S. M. & Cellerino, C. (2011).
Guías esquematizadas de tratamiento de los trastornos de personalidad para profesionales, desde el modelo de Young, Klosko y Wheishar (2003). Ciencias Psicológicas V (1): 83-115.
{kind=link}
{kind=link}