Artículo original
Prevalencia de alteraciones estructurales y funcionales arteriales en niños y adolescentes uruguayos asintomáticos.
Detección precoz niño-específico de daño aterosclerótico y riesgo cardiovascular relativo
Prevalence of structural and functional arterial abnormalities in asymptomatic Uruguayan children and adolescents. Child-specific early detection of atherosclerotic cardiovascular damage and relative risk
Br. Santiago Curcio1, Dra. Yanina Zócalo1 PhD, Br. Victoria García1,
Dres. Ignacio Farro1, Maite Arana2, Victoria Mattos2, Pedro Chiesa3, Gustavo Giachetto2, Daniel Bia1 PhD
1. Departamiento de Fisiología. Facultad de Medicina. Centro Universitario de Investigacion, Innovación y Diagnóstico Arterial (CUiiDARTE). Universidad de la República, UdelaR.
2. Departamento de Pediatría. Facultad de Medicina. UdelaR.
3. Servicio de Cardiología Pediátrica. Centro Hospitalario Pereira Rossel. ASSE.
Tema libre destacado en el 30 Congreso Uruguayo de Cardiología, 2014.
Correspondencia: Dr. Daniel Bia. Av. Gral Flores 2125. Departamento de Fisiología, Facultad de Medicina. Montevideo, 11800. Uruguay.
Correo electrónico: dbia@fmed.edu.uy
Resumen
Introducción: Los estudios arteriales no-invasivos se emplean en adultos para valoración de daño de órgano blanco, re-clasificación de riesgo cardiovascular y/o detección temprana de alteraciones en estructura y función arterial. Recientemente, se recomendó su empleo en niños, dado que permitirían detectar aquellos con mayor susceptibilidad a daño aterosclerótico y realizar intervenciones específicas tempranas que permitirían reducir el daño arterial, y por tanto el riesgo cardiovascular en la vida adulta. En Uruguay, en 2014 se inició la implementación de un servicio de evaluación arterial no-invasiva, gratuito. En este se aplican integradamente diversos estudios como evaluación de la rigidez arterial regional y local, espesor parietal, reactividad vascular, presión aórtica central, análisis de parámetros de reflexión de ondas de pulso, viabilidad sub-endocárdica, que permiten valorar el estado estructural y funcional arterial.
Objetivo: determinar la prevalencia de alteraciones arteriales en niños y adolescentes asintomáticos evaluados en el nuevo servicio, empleando para ello criterios diagnósticos recientemente propuestos por la Asociación Americana del Corazón (AHA).
Métodos: se incluyeron 365 niños/adolescentes (3-17 años, mediana 12 años) sin enfermedad conocida, en los que se valoraron factores de riesgo cardiovascular y se realizó estudio arterial integral. Se analizó: espesor íntima-media carotideo (CIMT; Ultrasonografía/software específico), rigidez aórtica (velocidad de onda de pulso carótido-femoral, VOP; Tonometría de aplanamiento) y reactividad vascular (RV; vasodilatación mediada por flujo). Se consideró alterado: 1) CIMT o VOP ³ percentil 95 (p95; para edad y sexo, propuesto por AHA), 2) RV <5%. Se cuantificó prevalencia de alteraciones, y relación con sexo y edad (mayores vs. menores de 12 años).
Resultados: la prevalencia de alteración estructural (CIMT»35%) y funcional (RV»25%) fue elevada, así como la de factores de riesgo cardiovascular. La prevalencia se elevó con la edad. No existió diferencia en prevalencia asociadas al sexo.
Conclusión: en los niños/adolescentes evaluados existió elevada prevalencia de niveles de CIMT, VOP y RV, por fuera de niveles de normalidad propuestos por la AHA. Dicha prevalencia, podría estar influenciada por la alta exposición a factores de riesgo. El aumento edad-relacionado en prevalencia de VOP elevada, podría asociarse a mayor tiempo de exposición a factores de riesgo al aumentar la edad (daño acumulado). La prevalencia encontrada podría estar influenciada por inadecuación de los valores de corte propuestos por la AHA para aplicarse en nuestra población. Esto refuerza la necesidad de contar con niveles de referencia/corte nacionales.
Summary
Introduction: non-invasive vascular studies are used in adults for assessment of target organ damage (TOD), cardiovascular risk re-classification and early detection of impairment in both arterial structure and function. Recently, it has been recommended to apply these studies in pediatric population, in order to detect those children with greater risk of developing atherosclerotic arterial disease and design early specific interventions that would allow to reduce arterial damage, and thus cardiovascular risk during adulthood. In 2014, an open access/free center (service) for children arterial evaluation was created in Uruguay. In this center, several studies are applied as an integrated approach to assess arterial structure and function parameters such as: local and regional arterial stiffness, arterial wall thickness, vascular reactivity, central aortic pressure, pulse-wave reflection analysis and sub-endocardial viability ratio. The aim of this study was to determine the prevalence of arterial alterations in children and adolescents evaluated in the new center, using reference values recently proposed by the American Heart Association (AHA). ]]>
Methods: 365 children/adolescents without known disease were included (3-17 years old, median 12 years). Cardiovascular risk-factor exposure was assessed and integrated arterial evaluation was applied. Carotid Intima-Media Thickness (CIMT; Ultrasonography/specific border detection software), aortic stiffness (Carotid-femoral Pulse Wave Velocity, PWV; applanation tonometry) and vascular reactivity (VR; flow-mediated dilation) were analyzed. Arterial impairment was considered when: 1) CIMT or PWV = 95th percentile (for age and sex, reference values from AHA), 2) VR<5%. Vascular impairment prevalence was quantified, and its relationship with age (<12 y.o vs. >12 y.o) and sex.
Results: the prevalence of structural (CIMT» 35%) and functional (VR» 25%) vascular impairment was high, and so was cardiovascular risk-factor exposure. Prevalence increased with age. No sex-related differences were found.
Conclusion: the children/adolescents evaluated showed high prevalence of CIMT, PWV and VR levels outside the reference ranges from the AHA. This prevalence could be partly explained by the high cardiovascular risk-factor exposure. The age-related increase in PWV high levels could be associated with a longer time of risk-factor exposure (accumulated damage). The prevalence found could also be explained by mismatch of the AHA reference values with Uruguayan population, thus enhancing the needs for national reference/normative values.
Key words:
ATHEROSCLEROSIS
EARLY DIAGNOSIS
RISK FACTORS
PREVALENCE
CHILD ]]>
A pesar de que es ampliamente conocido que la EA comienza temprano en la infancia(10), la prevalencia de factores de riesgo cardiovascular (FRCV) en niños es elevada, y el tiempo de exposición a ellos se asocia a cambios estructurales y funcionales arteriales precoces, los estudios arteriales mencionados han quedado relegados a la población adulta. Sin embargo, recientemente la evaluación arterial se ha comenzado a incluir en guías de prevención cardiovascular de niños y adolescentes(11-13) con el objetivo de: (1) detectar tempranamente alteraciones arteriales y valorar su extensión, principalmente en niños expuestos a FRCV (por ejemplo, bajo peso al nacer, sobrepeso/obesidad, dislipemias, hipertensión arterial) y/o (2) evaluar el efecto de intervenciones terapéuticas (no farmacológicas o farmacológicas) en el sistema arterial. Adicionalmente han comenzado a realizarse trabajos destinados a generar valores de referencia/normalidad en población pediátrica para los múltiples parámetros de estructura y función arterial que surgen de los estudios arteriales(12,13), así como destinados a determinar la asociación entre alteraciones y la presencia de FRCV(14).
Se estudiaron 365 niños y adolescentes (200 varones) con edades comprendidas entre los 3 y los 17 años (mediana: 12 años). Los niños incluidos en el trabajo fueron enviados por parte de sus médicos de referencia para valoración arterial de control, en ocasiones por presentar uno o más factores de riesgo cardiovascular. Se excluyeron aquellos que presentaban: patología cardiovascular congénita y/o adquirida, vasculopatías, enfermedad renal crónica, enfermedades neurológicas, enfermedades genéticas, patología oncológica, inmunodeficiencias primarias y/o secundarias, y enfermedades infecto-contagiosas. La realización de los estudios fue aprobada por el Comité de Ética del CHPR. Todos los estudios fueron realizados luego de la obtención del consentimiento informado y escrito por parte de los padres o tutores.
Entrevista clínica
Previo a la realización de cada estudio se llevó a cabo una entrevista clínica con el fin de determinar la presencia de FRCV y recabar datos antropométricos: peso, talla, índice de masa corporal (IMC). Para definir sobrepeso y obesidad se utilizaron tablas elaboradas por la Organización Mundial de la Salud (OMS). Se consideró sobrepeso cuando el IMC es superior al percentil 85 e inferior al percentil 97 para la edad y el sexo; y obesidad IMC mayor o igual al percentil 97 para edad y sexo. Los grupos definidos coinciden con valores de índice Z para IMC (zIMC; valores normalizados) entre +1 y +2 para sobrepeso, y superiores a +2 para obesidad. El valor zIMC es obtenido como: IMC calculado – percentil 50 (para edad y sexo)/desvío estándar. Fueron clasificados como sedentarios aquellos niños que realizaban un nivel de actividad física inferior a una carga de intensidad moderada(15). Se consideraron dislipémicos aquellos niños o adolescentes que tenían el diagnóstico previamente realizado por sus profesionales tratantes.
Estudios arteriales
Previo a la realización de los estudios, los niños y adolescentes guardaron reposo en posición supina por al menos 10 minutos, en un ambiente tranquilo y con una temperatura ambiente controlada (21 °C a 23 °C). Durante la evaluación se midió presión arterial (PA) y frecuencia cardíaca (FC) a intervalos próximos a los 5 minutos mediante la utilización de un sistema oscilométrico (Omron HEM-433INT; Omron Healthcare Inc., Illinois, USA). La PA media (PAM) fue calculada como la PA diastólica (PAD) más un tercio de la presión de pulso (PP = PAS – PAD). Si bien el estudio consistió en la medición de múltiples parámetros de estructura y función arterial, en este trabajo se incluyeron las mediciones de espesor íntima-media carotídeo, velocidad de onda del pulso carótido-femoral y reactividad vascular.
La rigidez aórtica fue estimada mediante el cálculo de la velocidad de la onda de pulso carótido-femoral (VOP). Para ello se utilizó el método transcutáneo de medición “pie a pie” de la onda de pulso(4). Este consiste en la obtención secuencial de la onda de pulso carotídeo y femoral (tonometría de aplanamiento; SphygmoCor, Atcor Medical, Australia), cuantificando el retardo temporal (Dt) entre los pies de las ondas y la distancia entre los sitios de registro (Dx). Los pies de onda fueron determinados utilizando el algoritmo de intersección de tangentes y el Dx fue calculado utilizando la llamada “distancia sustraída”(4). Esta se obtiene de restar la distancia entre el hueco supraesternal (HSE) y el sitio de registro en la carótida, a la distancia entre el HSE y el sitio de registro femoral. La VOP se calcula entonces como Dx/Dt considerando el promedio de al menos tres registros. Cada registro fue considerado como válido si fue calculado para al menos diez latidos y si la desviación estándar fue menor a 10% del valor medio obtenido(4). La VOP se consideró elevada cuando sus valores fueron superiores al percentil 95 según edad y sexo, utilizando los valores de referencia propuestos por la AHA(13).
Reactividad vascular
Se estudió la reactividad vascular (RV) mediante test de vasodilatación mediada por flujo (VMF)(5). Con el niño/adolescente en posición supina se colocó el miembro superior izquierdo en un soporte estereotáxico que cuenta con un sistema de sujeción que permite colocar (y fijar) el transductor ecográfico de 7-12MHz. A su vez, se coloca un manguito (brazalete) de esfigmomanómetro (tamaño pediátrico) a nivel del antebrazo. Este estudio consiste en la visualización de la arteria humeral en un corte longitudinal a partir del empleo de ultrasonido en modo B, y de la determinación de velocidades sanguíneas humerales mediante empleo de la modalidad Doppler (dúplex). Para ello, se obtiene al menos una secuencia de imágenes (videos de al menos 30 segundos de duración) en condición basal, a la vez que registros de velocidad sanguínea, y a continuación (sin dejar de grabar) se insufla el manguito oclusor hasta al menos 50 mmHg por encima de la PAS humeral, de manera de generar isquemia transitoria en el sector distal al mismo (tercio distal de antebrazo y mano) durante 5 minutos. Finalmente, continuando con la adquisición de datos se procede a liberar la oclusión (dando lugar al fenómeno conocido como hiperemia reactiva), adquiriendo datos por al menos tres minutos posliberación. A partir de los datos (videos) adquiridos, y empleando un software específico, se obtienen las variaciones instantáneas de diámetro arterial (variaciones latido-a-latido) y velocidad sanguínea. Posteriormente, la máxima dilatación generada por el estímulo hiperémico alcanzado se cuantifica en términos absolutos y relativos (%; máxima dilatación diastólica alcanzada respecto del diámetro diastólico basal)(5). La RV se consideró disminuida si existió constricción o dilatación mediada por flujo inferior a 5%.
Análisis de datos y procesamiento estadístico
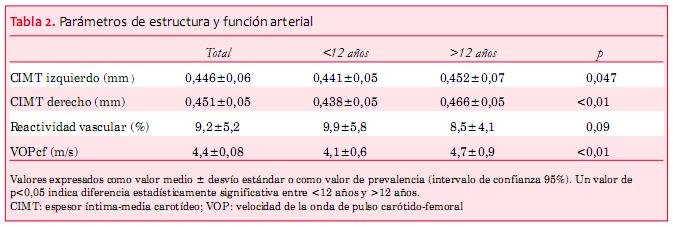
Los datos fueron expresados como media (M) ± desvío estándar (DE) o como porcentaje respecto de la población total o grupo etario específico. En Resultados se describen las variables halladas en la población total y se comparan dos grupos: menores de 12 años y mayores de 12 años.
Primero, empleando los niveles de corte propuestos por la AHA, se determinó una elevada prevalencia de alteraciones en estructura y función arterial evaluados mediante tres de los principales parámetros empleados en valoración arterial: CIMT, VOP y RV. Al respecto, un ~35% y ~22% de los niños y adolescentes evaluados presentaron niveles de CIMT y RV por encima y debajo de los niveles de corte propuestos (tabla 2).
Esta elevada prevalencia, que determina que ~1/3 de los niños/adolescentes estudiados presenten CIMT elevado y ~1/5 niveles reducidos de RV, podría al menos deberse a dos causas. Como primer aspecto, la elevada prevalencia podría relacionarse con la elevada exposición a FRCV que mostró tener la población estudiada, con especial énfasis en los niveles de obesidad. Cabe resaltar que la obesidad infantil se asocia estrechamente con cambios arteriales precoces(14). Al respecto, de la población estudiada ~1/5 presentó sobrepeso, ~1/4 presentó obesidad, ~1/4 presentó cifras elevadas de PA durante el estudio y ~1/2 presentó niveles de actividad física compatibles con la definición de sedentarismo. Consecuentemente, al tratarse de una población con elevada exposición a FRCV, era esperable encontrar que su sistema arterial presentase alteraciones detectables de manera no invasiva.
Es importante señalar que la inclusión de niños y adolescentes consecutivos que asistieron al servicio, sin un muestreo específico, hace que esta serie no sea representativa de la población nacional. Al respecto, en especial los niveles de prevalencia de obesidad fueron mayores que los reportados en trabajos previos. Esto podría haber sido generado por una mayor tendencia, por parte de los profesionales que derivaron a los niños a ser estudiados, a centrarse en aquellos que mostraban evidencias notorias de presentar una alteración por exceso nutricional. A manera de ejemplo, el estudio ENSO, realizado 15 años atrás en nuestro país (año 2000), obtuvo datos de 886 niños/adolescentes de 9 a 12 años de poblaciones urbanas, reportando que el 17% presentaba sobrepeso (IMC: p85-p94,9) y 9% obesidad (IMC > p95), y consecuentemente ~26% presentaba sobrepeso u obesidad(34). Este resultado muestra un muy similar nivel de sobrepeso respecto de esta serie (17% vs 19%), pero una prevalencia mucho menor de obesidad (~9% vs ~26%). Al igual que en esta serie, los autores reportaron reducción significativa en la prevalencia de obesidad al alcanzarse los 12 años de edad, lo que podría estar vinculado al inicio del empuje de crecimiento determinado por la pubertad(34).
Segundo, existió un aumento edad-asociado en la prevalencia de alteraciones arteriales al comparar los grupos de menores y mayores de 12 años de edad. En este sentido, los mayores de 12 años presentaron mayor prevalencia de CIMT elevado (p = 0,02), mayor prevalencia de VOP elevada (p < 0,01) y una mayor proporción de RV disminuida (si bien no alcanzó significancia estadística).
En teoría, estas diferencias podrían ser parcialmente explicadas por un mayor tiempo de exposición a los FRCV en el grupo de mayores de 12 años. Al respecto, en el año 2002, resultados del International Childhood Cardiovascular Cohort (i3C) Consortium (incluyó a más de 40.000 niños) demostraron que a los 6 años de vida en varones y a los 9 en ambos sexos el nivel de exposición a FRCV se asocia con el nivel de EA subclínica (medido por CIMT) en adultos (20-45 años), y que si bien antes de los 9 años la asociación entre FRCV y EA (evaluada por CIMT en adultos jóvenes) es débil, a partir de los 9 años de edad existe una importante asociación entre FRCV del niño/adolescente y el deterioro arterial del adulto(35). En otras palabras, a mayor edad del niño, mayor es su exposición a FRCV, y más estrechamente comienza a existir asociación con el deterioro arterial que tendrá en su vida adulta. Más específicamente, individualmente el colesterol total (a los 12, 15 y 18 años), la PA sistólica (a los 6, 12, 15 y 18 años) y el IMC (a los 9, 12, 15 y 18 años) mostraron asociación con EA (evaluada por CIMT) en adultos (20-45 años)(35). Cuanto mayor sea la edad del niño que presenta FRCV, mayor es la asociación con riesgo cardiovascular elevado al ser adulto(35-38).
Aspectos metodológicos
Importancia biomédica
Los resultados expuestos ponen de manifiesto que la evaluación arterial no invasiva en niños y adolescentes permite detectar precozmente alteraciones estructurales y/o funcionales asociadas a la EA y a un riesgo cardiovascular relativo (para la edad) elevado. Además, es sabido que: (1) la susceptibilidad terapéutica de la EA disminuye conforme aumenta la edad(40) y (2) la aplicación de intervenciones adecuadas en niños y adolescentes permite reducir e incluso revertir dichas alteraciones arteriales(41). Por lo tanto, estos estudios podrían permitir discriminar determinados grupos de niños y adolescentes que se beneficiarían de recibir un seguimiento individualizado y/o de la aplicación de medidas terapéuticas específicas.
Por otra parte, estos resultados permiten evidenciar que la prevalencia de alteraciones arteriales en edades tempranas puede ser elevada y que los FRCV a los que se enfrentan los niños ya pueden estar modificando sustancialmente la estructura y función arterial. En consecuencia, evidenciar que en edades muy tempranas ya el daño se encuentra funcionalmente presente debería fortalecer la puesta en práctica de medidas para reducir la exposición a FRCV, a la vez que emplear estas técnicas a la hora de intentar discriminar/diagnosticar tempranamente aquellos niños que podrían necesitar un refuerzo especial en medidas preventivas.
1. Mancia G, Fagard R, Narkiewicz K, Redon J, Zanchetti A, Böhm M, et al; Task Force for the Management of Arterial Hypertension of the European Society of Hypertension and the European Society of Cardiology. 2013 ESH/ESC Practice Guidelines for the Management of Arterial Hypertension. Blood Press 2014; 23(1):3-16.
2. Perk J, De Backer G, Gohlke H, Graham I, Reiner Z, Verschuren M, et al; European Association for Cardiovascular Prevention & Rehabilitation; ESC Committeefor Practice Guidelines. European Guidelines on cardiovascular diseaseprevention in clinical practice: version 2012. The Fifth Joint Task Force of the European Society of Cardiology and Other Societies on Cardiovascular DiseasePrevention in Clinical Practice (constituted by representatives of nine societies and by invited experts). Eur Heart J 2012;33(13):1635-701.
3. Naghavi M, Libby P, Falk E, Casscells SW, Litovsky S, Rumberger J, et al. From vulnerable plaque to vulnerable patient: a call for new definitions and risk assessment strategies: Part I. Circulation 2003; 108(14):1664-72.
4. Bia D, Zócalo Y. Rigidez arterial: evaluación no invasiva en la práctica clínica Importancia clínica y análisis de las bases metodológicas de los equipos disponibles para su evaluación. Rev Urug Cardiol 2014; 29(1):39-59.
5. Bia D, Zócalo Y. Reactividad vascular: evaluación no invasiva en la práctica clínica. Importancia clínica y análisis de las bases metodológicas de los equipos disponibles para su evaluación. Rev Urug Cardiol 2014; 29:351-68.
6. Santana DB, Zócalo YA, Armentano RL. Integrated e-Health approach based on vascular ultrasound and pulse wave analysis for asymptomatic atherosclerosis detection and cardiovascular risk stratification in the community. IEEE Trans Inf Technol Biomed 2012;16(2):287-94.
7. Santana DB, Zócalo YA, Ventura IF, Arrosa JF, Florio L, Lluberas R, et al. Health informatics design for assisted diagnosis of subclinical atherosclerosis, structural, and functional arterial age calculus and patient-specific cardiovascular risk evaluation. IEEE Trans Inf Technol Biomed 2012; 16(5):943-51.
8. Bia D, Zócalo Y, Farro I, Torrado J, Farro F, Florio L, et al. Integrated evaluation of age-related changes in structural and functional vascular parameters used to assess arterial aging, subclinical atherosclerosis, and cardiovascular risk in uruguayan adults: CUiiDARTE Project. Int J Hypertens 2011; 2011:587303.
9. Zócalo Y, Bia D. Presión aórtica central y parámetros clínicos derivados de la onda del pulso: evaluación no invasiva en la práctica clínica. Importancia clínica y análisis de las bases metodológicas de los equipos disponibles para su evaluación. Rev Urug Cardiol 2014; 29(2):92-107.
10. Berenson G, Srinivasan SR, Bao W, Newman WP 3rd, Tracy RE, Wattigney WA. Association between multiple cardiovascular risk factors and atherosclerosis in children and young adults: The Bogalusa Heart Study. N Engl J Med 1998;338(23): 1650-6.
11. Urbina EM, Williams RV, Alpert BS, Collins RT, Daniels SR, Hayman L, et al; American Heart Association Atherosclerosis, Hypertension, and Obesity in Youth Committee of the Council on Cardiovascular Disease in the Young. Noninvasive assessment of subclinical atherosclerosis in children and adolescents: recommendations for standard assessment for clinical research: a scientific statement from the American Heart Association. Hypertension 2009; 54(5):919-50.
12. Reusz GS, Cseprekal O, Temmar M, Kis E, Cherif AB, Thaleb A, et al. Reference values of pulse wave velocity in healthy children and teenagers. Hypertension 2010;56(2):217-24.
13. Doyon A, Kracht D, Bayazit A, Deveci M, Duzova A, Krmar RT, et al. Carotid artery intima-media thickness and distensibility in children and adolescents: reference values and role of body dimensions. Hypertension 2013;62(3):550-6.
14. Cote AT, Harris KC, Panagiotopoulos C, Sandor GG, Devlin AM. Childhood obesity and cardiovascular dysfunction. J Am Coll Cardiol 2013;62(15): 1309-19.
15. Argentina. Comité Nacional de Medicina del Deporte Infanto-Juvenil. Subcomisión de Epidemiología. Consenso sobre factores de riesgo de enfermedad cardiovascular en pediatría: sedentarismo. Arch Argent Pediatr 2005;103(5):450-63.
16. Stein JH, Korcarz CE, Hurst RT, Lonn E, Kendall CB, Mohler ER, et al; American Society of Echocardiography Carotid Intima-Media Thickness Task Force. Use of carotid ultrasound to identify subclinical vascular disease and evaluate cardiovascular disease risk: a consensus statement from the American Society of Echocardiography Carotid Intima-Media Thickness Task Force. Endorsed by the Society for Vascular Medicine. J Am Soc Echocardiogr 2008; 21(2):93-111.
17. Oren A, Vos LE, Uiterwaal CS, Gorissen WH, Grobbee DE, Bots ML. Change in body mass index from adolescence to young adulthood and increased carotid intima-media thickness at 28 years of age: the Atherosclerosis Risk in Young Adults study. Int J Obes Relat Metab Disord 2003;7(11):1383-90.
18. Freedman DS, Patel DA, Srinivasan SR, Chen W, Tang R, Bond MG, et al.The contribution of childhood obesity to adult carotid intima-media thickness: the Bogalusa Heart Study. Int J Obes (Lond) 2008;32(5):749-56.
19. Ianuzzi A, Licenziati MR, Acampora C, Salvatore V, Auriemma L, Romano ML, et al. Increased Carotid Intima-Media Thickness and Stiffness in Obese Children. Diabetes Care 2004; 27(10):2506-8.
20. Tounian P, Aggoun Y, Dubern B, Varille V, Guy-Grand B, Sidi D, et al. Presence of increased stiffness of the common carotid artery and endothelial dysfunction in severely obese children: a prospective study. Lancet 2001; 358(9291): 1400-4.
21. Baker JL, Olsen LW, Sørensen TI. Childhood body-mass index and the risk of coronary heart disease in adulthood. New Engl J Med 2007; 357(23): 2329-37.
22. Must A, Jacques PF, Dallal GE, Bajema CJ, Dietz WH. Long-term mortality of overweight adolescents: a follow-up of the Harvard Growth Study of 1922 to 1935. New Engl J Med 1992; 327(19):1350-5.
23. Gunnell DJ, Frankel SJ, Nanchahal K, Peters TJ, Davey Smith G. Childhood obesity and adult cardiovascular mortality: a 57-y follow-up study based on the Boyd Orr cohort. Am J Clin Nutr 1998; 67(6):1111-8.
24. Atabek ME, Pirgon O, Kirvak AS. Evidence for association between insulin resistance and premature carotid aterosclerosis in childhood obesity. Pediatr Res 2007; 61(3):345-9.
25. Kim I, Moon SO, Kim SH, Kim HJ, Koh YS, Koh GY. Vascular endothelial growth factor expression of intercellular adhesion molecule 1 (ICAM-1), vascular cell adhesion molecule 1 (VCAM-1), and E-selectin through nuclear factor-kappa B activation in endothelial cells. J BiolChem 2001; 276(10):7614-20.
27. Urbina EM, Khoury PR, McCoy C, Daniels SR, Kimball TR, Dolan LM. Cardiac and vascular consequences of pre-hypertension in youth. J Clin Hypertens (Greenwich) 2011;13(5):332-42.
28. Urbina EM, de Ferranti S, Steinberger J. Observational studies may be more important than randomized clinical trials: weaknesses in US Preventive ServicesTask Force recommendation on blood pressure screening in youth. Hypertension 2014; 63(4):638-40.
29. Huynh QL, Blizzard CL, Sharman JE, Magnussen CG, Dwyer T, Venn AJ. The cross-sectional association of sitting time with carotid artery stiffness in young adults. BMJ Open 2014;4(3):e004384.
30. Urbina EM, Khoury PR, McCoy CE, Dolan LM, Daniels SR, Kimball TR. Triglyceride to HDL-C ratio and increased arterial stiffness in children, adolescents, and young adults. Pediatrics 2013;131(4): e1082-90.
31. Maki KC, Davidson MH, Dicklin MR, Bell M, Witchger M, Feinstein SB. Predictors of anterior and posterior wall carotid intima media thickness progression in men and women at moderate risk of coronary heart disease. J Clin Lipidol 2011;5(3): 141-51.
32. Norata GD, Raselli S, Grigore L, Garlaschelli K, Vianello D, Bertocco S, et al. Small dense LDL and VLDL predict common carotid artery IMT and elicit an inflammatory response in peripheral blood mononuclear and endothelial cells. Atherosclerosis 2009;206(2):556-62.
33. Mora S, Szklo M, Otvos JD, Greenland P, Psaty BM, Goff DC Jr, et al. LDL particle subclasses, LDL particle size, and carotid atherosclerosis in the Multi-Ethnic Study of Atherosclerosis (MESA). Atherosclerosis 2007; 192(1):211-7.
34. Pisabarro R, Recalde A, Irrazabal E, Chaftare Y. ENSO niños I: primera encuesta nacional de sobrepeso y obesidad en niños uruguayos. Rev Méd Urug 2002; 18(3):244-50.
35. Juonala M, Magnussen CG, Venn A, Dwyer T, Burns TL, Davis PH, et al. Influence of age on associations between childhood risk factors and carotid intima-media thickness in adulthood: the Cardiovascular Risk in Young Finns Study, the Childhood Determinants of Adult Health Study, the Bogalusa Heart Study, and the Muscatine Study for the International Childhood Cardiovascular Cohort (i3C) Consortium. Circulation 2010; 122(24):2514-20.
36. Webber LS, Srinivasan SR, Wattigney WA, Berenson GS. Tracking of serum lipids and lipoproteins from childhood to adulthood. The Bogalusa Heart Study. Am J Epidemiol 1991;133(9):884-99.
37. Juonala M, Raitakari M, S A Viikari J, Raitakari OT. Obesity in youth is not an independent predictor of carotid IMT in adulthood: The Cardiovascular Risk in Young Finns Study. Atherosclerosis 2006; 185(2):388-93.
38. Chen X, Wang Y. Tracking of blood pressure from childhood to adulthood: a systematic review and meta-regression analysis. Circulation 2008;117 (25): 3171-80.
39. Nichols W, O’Rourke MF, eds. McDonald’s blood flow in arteries: theoretical, experimental and clinical principles. 5ed. London: Hodder Arnold, 2005.
40. Kavey RE, Allada V, Daniels SR, Hayman LL, McCrindle BW, Newburger JW, et al; American Heart Association Expert Panel on Population and Prevention Science; Council on Cardiovascular Disease in the Young; Council on Epidemiology and Prevention; Council on Nutrition; Council on Physical Activity and Metabolism; Council on High Blood Pressure Research; Council on Cardiovascular Nursing; Council on the Kidney in Heart Disease; Interdisciplinary Working Group on Quality of Care and Outcomes Research. Cardiovascular risk reduction in high-risk pediatric patients: a scientific statement from the American Heart Association Expert Panel on Population and Prevention Science; the Councils on Cardiovascular Disease in the Young, Epidemiology and Prevention, Nutrition, Physical Activity and Metabolism, High Blood Pressure Research, Cardiovascular Nursing, and the Kidney in Heart Disease; and the Interdisciplinary Working Group on Quality of Care and Outcomes Research. J CardiovascNurs 2007; 22(3):218-53.
41. Pahkala K, Heinonen OJ, Simell O, Viikari JS, Rönnemaa T, Niinikoski H, et al. Association of physical activity with vascular endothelial function and intima-media thickness. Circulation 2011; 124(18):1956-63.
{kind=link}