ARCHIVOS DEL INSTITUTO DE NEUROLOGÍA
Caso Clínico de Interés
Síndrome de Lambert - Eaton.
Características clínicas y neurofisiológicas
Lambert Syndrome - Eaton.
Clinical and neurophysiological characteristics
Recibido: 19/08/15 Aceptado: 24/09/15
Institución responsable: Instituto de Neurología. Hospital de Clínicas. Facultad de Medicina. UdelaR. Montevideo, Uruguay.
Correspondencia: Dr. H.Jochen Hackembruch. E-mail: hackembruch@gmail.com
Resumen: Arch Med Interna 37(3):
El síndrome miasténico de Lambert Eaton (LEMS) es una enfermedad de la transmisión neuromuscular pre sináptica poco frecuente e infra diagnosticada, con síntomas clínicos característicos aunque poco específicos pero hallazgos neurofisiológicos muy típicos. En la mayor parte de los casos se presenta como un síndrome paraneoplásico aunque existen formas idiopáticas.
Discutimos la fisiopatología del trastorno, estableciendo, como hecho fundamental la presencia de anticuerpos contra los canales de calcio voltaje dependientes pre sinápticos, siendo este hecho fundamental para la comprensión del tratamiento sintomático planteado.
Repasamos las características que se asocian a mayor riesgo de neoplasia oculta y planteamos la estrategia de seguimiento para despistarla precozmente.
Palabras claves: Eaton Lambert. Síndrome miasténico. Síndrome paraneoplásico.
Abstract: Arch Med Interna 37(3):
Lambert Eaton myasthenic syndrome (LEMS) is an uncommon neuromuscular joint disease, usually infra diagnosed, with characteristic but nonspecific clinical symptoms but very typical neurophysiological findings. In most cases it is a paraneoplastic syndrome although idiopathic forms also exist.
We describe the case of a patient with typical clinical presentation and neurophysiological findings that allowed the diagnosis. The initial screening for hidden malignancy was negative, but the follow up is essential to rule it out given its strong association. The evolution was satisfactory with symptomatic treatment.
We review the features that are associated with increased risk of hidden malignancy and propose a follow-up strategy to throw it off early.
Key words: Eaton Lambert. Myasthenic síndrome. Paraneoplastic syndrome.
INTRODUCCIÓN
El síndrome miasténico de Lambert - Eaton (LEMS) es un defecto de la transmisión neuromuscular sináptica, de tipo presináptico, autoinmune y adquirido. Se caracteriza por la presencia clínica de debilidad muscular espinal y con evolución fluctuante. Como hecho clínico característico no compromete la musculatura craneal en su inicio. Se acompaña de síntomas autonómicos, síntomas sensitivos no sistematizables y arreflexia. Es considerado un síndrome neurológico paraneoplásico clásico, pero puede ser idiopático (1-4).
CASO CLÍNICO
Paciente de 41 años de sexo masculino sano que presenta una historia de 1 año de evolución de síntomas sensitivos no sistematizables que se relatan como parestesias en 4 miembros. Además debilidad muscular fluctuante que se acentúa con el ejercicio fisco y mejora con el reposo. Refiere disfunción eréctil y eyaculación precoz. En la evolución el cuadro permanece estable y sin agregar síntomas o signos de participación craneal. Niega síntomas extraneurológicos, antecedentes de tabaquismo o enfermedad neoplásica. Niega repercusión general.
Al examen físico presenta pares craneales normales. No cefaloparesia. A nivel espinal no se observa amiotrofia o actividad muscular espontánea visible. Tono normal. Paresia generalizada, leve, a predominio proximal y de miembros inferiores sin fenómeno de apokamnosis. Arreflexia de los cuatro miembros. Cutáneo plantar en flexión. Coordinación normal y sensibilidad normal. Examen de piel, mucosas y faneras normal. Linfoganglionar normal. Pleuropulmonar normal. Abdomen y fosas lumbares normales.
Se realiza estudio de neuroconducción sensitivo - motora, electromiograma y estudio de transmisión neuromuscular repetitiva a baja y alta frecuencia.
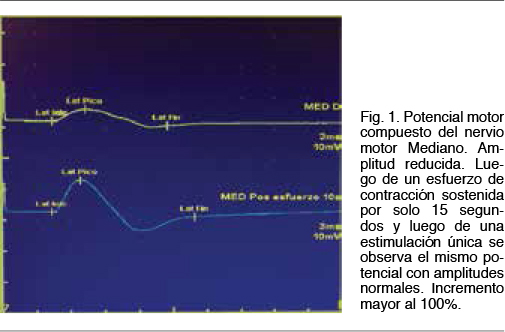
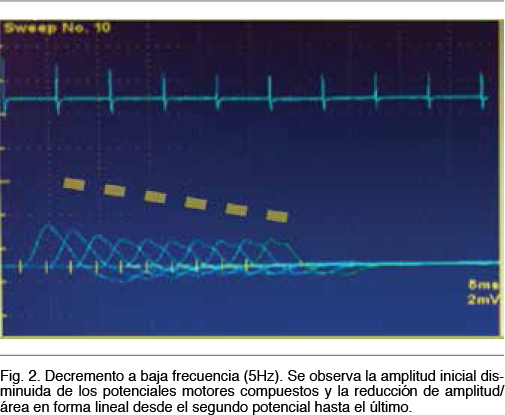
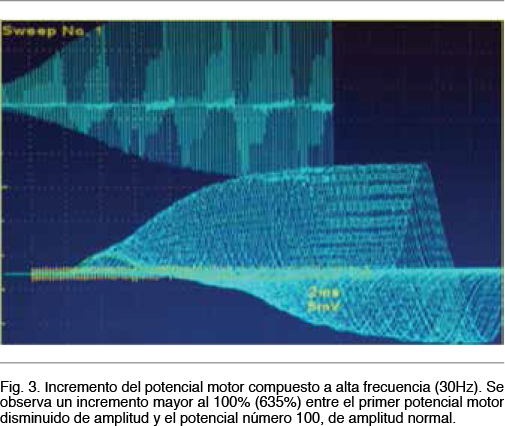
Se observa una neuroconducción sensitiva con latencias distales, amplitudes y velocidades de conducción normales. El electromiograma fue normal. Del estudio de neuroconducción motora destacamos la presencia de potenciales motores bien configurados, de latencias normales, con velocidades de conducción motora normales y sin bloqueos de la conducción, pero con amplitudes reducidas en 4 miembros. Se realiza una breve contracción isométrica de 15 segundos y se procede a la estimulación motora nuevamente, observandose un incremento de la amplitud a rangos normales. El incremento de amplitud obtenido fue > 100% para nervio motor Mediano (Figura 1). En el estudio de transmisión neuromuscular repetitiva realizado en el nervio motor Cubital se observa un decremento en el tren de potenciales obtenidos a baja frecuencia (5Hz) en un 33% entre el primer potencial y el cuarto potencial y con una morfología del tren en descenso lineal (Figura 2). El cociente de decremento tardío / decremento temprano fue de 102%. A alta frecuencia (30Hz) se observo un incremento de la amplitud de un 635% entre el primer potencial y el potencial número 100 (Figura 3).
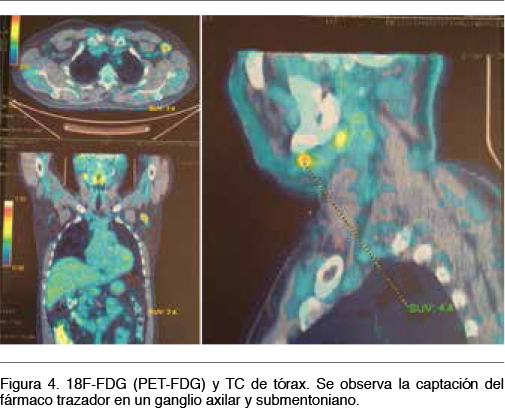
]]>Se realiza así el diagnóstico clínico - electrofisiológico de Síndrome Miasténico de tipo presináptico y dentro de este subgrupo por sus características clínicas el de un LEMS. Se calculó un Delta p- Score de 1. Hemograma, VES y enzimograma hepático normal. PEF normal. Se solicitó Rx de tórax y tomografía de cuerpo entero. No se observan imágenes sugestivas de una neoplasia. Se realiza a continuación tomografia por emisión de positrones con 18F-FDG (PET-FDG) observando adenopatías múltiples (regiones cervicales, axilares, de mediastino y retroperineales), algunas de ellas hipermetabolicas (axilar izquierda, submaxilar derecha e inguinales bilaterales a predomionio izquierdo), donde se destaca por su tamaño y nivel de captación la axilar izquierda (Figura 4). Se envía al paciente para realización de biopsia diagnóstica del ganglio más accesible. No se realizo dosificación de los anticuerpos anti canales voltaje dependientes de calcio (VGCC tipo P/Q o tipo N) por no disponer de dicha técnica en nuestro país.
El paciente recibe como tratamiento sintomático Piridostigmina 60 mg v.o. en tres tomas diarias, con mejoría sintomática del cuadro de debilidad. No es posible obtener en nuestro país la 3-4 Diaminopiridina como tratamiento de elección. Se mantiene en control para la búsqueda de neoplasia oculta.
DISCUSIÓN
El LEMS es una de las enfermedades de la unión neuromuscular probablemente más subdiagnósticada, es poco frecuente, con una incidencia estimada en 0,5 casos por millón/año y una prevalencia de 3,4 casos por millón (1). Fue descripta por Eaton y Lambert en el año 1957. Es un defecto de la transmisión neuromuscular de tipo presináptico, de origen autoinmune, donde la existencia de anticuerpos anti canales voltaje dependientes de calcio impiden la entrada de este ión a la terminal presinaptica axonal (1-4). El influjo normal de calcio ocurre cuando el potencial de acción de membrana arriba a la terminal axónica y genera la apertura de estos canales voltaje dependientes. El calcio ingresa al axón distal y promueve, con su unión a una serie de proteínas citoplasmáticas, la liberación de Acetilcolina. La Acetilcolina asegura así la depolarización de la membrana postsináptica muscular (neurotransmision quimica). Debemos destacar que el egreso de Acetilcolina se realiza de dos formas: 1) desde un compartimiento de movilización inmediata, pronto para su liberación y 2) desde una reserva no disponible en forma inmediata pero de mayor cantidad de Acetilcolina (5, 6). Es esta última movilización de Acetilcolina la cual no se produce en el LEMS generando una falla en la neurotransmisión que explican los hallazgos clínicos y electrofisiológicos. La estimulación a alta frecuencia o la contracción voluntaria y sostenida de breve duración permiten una mayor entrada de calcio en la terminal presináptica resolviendo transitoriamente el defecto mencionado (5,6). La debilidad muscular afecta típicamente el sector espinal, al inicio a predominio de miembros inferiores, en su sector proximal y de forma simétrica. No comienza con una afectación craneal, pero este sector puede verse afectado en la evolución y en casos severos (1,4). Pacientes con LEMS pueden presentar hipo o arreflexia. Una manifestación típica pero presente en solo un 40% de los pacientes (nuestro paciente no lo presentaba) es la aparición de los reflejos ostetendinosos y mejoría de la fuerza muscular pos-ejercicio (1).
El síndrome no es solo motor y también ocurren síntomas a nivel autonómico. Los síntomas más frecuentes son la boca seca y la disfunción eréctil en el hombre. Otros síntomas menos comunes descriptos son: constipación, hipotensión ortostática, ojos secos, alteraciones en la sudación y disfunción en la micción (1). La exploración clínica y electrofisiológica sensitiva somática es normal.
El diagnóstico de LEMS es difícil, debido a su forma de presentación y evolución lentamente progresiva. Los diagnósticos erróneos incluyen desde miopatías hasta patología degenerativa de columna como la estenosis del canal lumbosacro. Cuando la afectación ya compromete el sector craneal el diagnostico de Miastenia Gravis suele ser otro de los errores más comunes. Cabe destacar además en este último caso, que la estimulación repetitiva a baja frecuencia en ambas patologías demuestran un decremento del tren de potenciales motores, por lo cual su mala interpretación puede colaborar al diagnóstico erróneo si solo se analiza este hecho (2). En la Miastenia Gravis los potenciales motores no son de baja amplitud y el perfil de descenso en la transmisión repetitiva a baja frecuencia es diferente y no hay anormalidades en la transmisión repetitiva a altas frecuencias como en el LEMS (2).
Para el diagnostico de LEMS es útil pero no imprescindible la dosificación de anticuerpos VGCC tipo P/Q si bien estos pueden encontrarse en otras patologías paraneoplásicas, aunque paradójicamente su presencia no siempre indica un riesgo de neoplasia asociada (1, 4, 7).
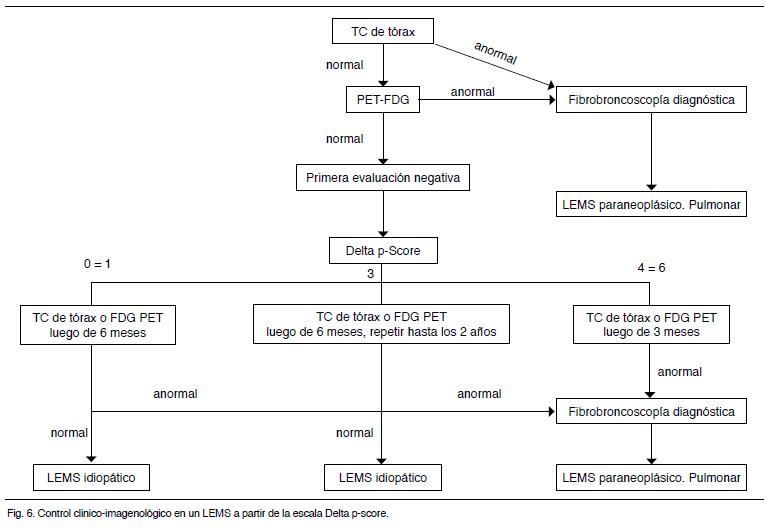
El LEMS es clásicamente un síndrome paraneoplásico, pero puede ser idiopático en el 40% de los casos. El tumor más frecuente es el pulmonar a células pequeñas. Se reportan casos secundarios a síndromes linfoproliferativos (1,8). El riesgo de un LEMS paraneoplásico de origen pulmonar aumenta en mayores de 50 años y tabaquistas. En estos casos pueden encontrarse como asociación otros anticuerpos como el Hu. El ¨Delta p-score¨ es un puntaje que se calcula en un paciente con LEMS para determinar la probabilidad de presentar una neoplasia pulmonar asociado al momento del diagnóstico (Figura 5) (1). La evaluación imagenológica consiste en una tomografía de cuerpo entero y si esta es normal la realización de un PET - FDG (1,9). Si en la primera evaluación de búsqueda de neoplasia es negativa, deberá realizarse un seguimiento durante los siguientes 5 años, siendo los dos primeros años donde se registra la mayor incidencia de estudios positivos. La frecuencia con que se repetirán dichos estudios podrá sistematizarse mediante el Delta p-score (Figura 6).
El tratamiento es sintomático y etiopatogénico. En los sintomáticos se utiliza la piridostigmina via oral que promueve la inhibición de la enzima acetilcolinesterasa, o la 3,4 diaminopiridina via oral que promueve la inhibición de canales de potasio presinápticos que provocan mayor liberación de vesículas de acetilcolina. Ambos tratamientos aumentan la disponibilidad de acetilcolina en la terminal postsináptica. En cuanto al tratamiento etiopatogénico este subyace en la remoción de los anticuerpos a través de inmunoglobulinas o plasmaferesis. También pueden utilizarse inmunosupresores para inhibir la producción de los mismos. El tratamiento oncoespecífico se realizará una vez detectado la neoplasia en las formas de LEMS paraneoplásicas.
La evolución y pronostico dependerán de si se trate de un LEMS idiopático o paraneoplásico.
Las formas severas requieren un tratamiento con inmunosupresores e IG o plasmaféresis y en general se relacionan a formas paraneoplásicas siendo habitualmente suficiente con el tratamiento sintomático en los casos idiopáticos como en el paciente descrito.
CONCLUSIONES
El LEMS es una enfermedad poco frecuente y subdiagnósticada. Se presenta bajo la asociación de síntomas y signos motores y autonómicos. La neurofisiología es una de las herramientas más útiles en su diagnóstico por los hallazgos característicos más aún cuando las técnicas de detección de anticuerpos contra los canales voltaje dependiente de calcio no están disponibles. Es una enfermedad neurológica paraneoplásica típica, existiendo casos idiopáticos y su seguimiento debe ser no menor a 5 años para la exclusión de una neoplasia, dentro de las cuales se impone el carcinoma pulmonar a células pequeñas.
BIBLIOGRAFIA
1. Titulaer MJ, Kang B, Verschuuren JJ. Lambert - Eaton myasthenic syndrome: from clinical characteristics to therapeutic strategies. Lancet Neurol 2011; 10: 1098-1107.
2. Sanders D, Cao L, Massey J, Juel V, Hobson-Webb L, Guptill J. Is the decremental pattern in Lambert - Eaton syndrome different from that in myasthenia gravis. Clin Neurophysiol. 2014;125:1274-7
3.
4. Zhang K, Liu W, Li Y, Zhang K, Gao X, Wang J. Mediastinal small cell cancer associated with Lambert-Eaton myasthenic syndrome: A case report. Exp Ther Med. 2015; 10: 117-120.
5.
6. Cherian A, Baheti N, Lype T. Electrophysiological study in neuromuscular junction disorders. Ann Indian Acad Neurol. 2013; 16: 34–41.
7. Bekircan-Kurt C, Çiftçi E, Kurne A, Anlar B. Voltage gated calcium channel antibody-related neurological diseases. World J Clin Cases 2015; 3: 293-300.
8. Graus F, Ariño H, Dalmau J. Paraneoplastic neurological syndromes in Hodgkin and non-Hodgkin lymphomas. Blood 2014; 123: 3230–38.
9. Braatz V, Kay C, Lorenzoni P, Ludwig B, Junior MM, Ioshii S, et al. Fluoro-2-deoxy-D-glucose positron emission tomography/computed tomography imaging in the investigation of Lambert Eaton myasthenic syndrome. Arq Neuropsiquiatr. 2013; 71: 643-644.
{kind=link}
{kind=link}