Caso Clínico de Interés
Abscesos de hipófisis: presentación de dos casos clínicos y revisión de la literatura
Pituitary abscess: two cases assisted and review of the literature is presented
Dr. Diego Graña
Asistente Clínica Médica.
Residente Medicina Interna.
Dra. Mercedes Perendones
Profesor Adjunto Clínica Médica.
Dr. Carlos Dufrechou
Profesor Clínica Médica
Institución responsable: Clínica Médica 2 (Facultad de Medicina - UdelaR). Hospital Pasteur.
Correspondencia: Dr. Diego Graña. Hervidero 2932. Montevideo, Uruguay. CP 11700. Correo electrónico: diegograna@adinet.com.uy
Resumen: Arch Med Interna 37(3):
El absceso de hipófisis es una enfermedad poco frecuente, constituye menos del 1% de la patología selar, con alta dificultad diagnóstica, clínica poco orientadora,
imagenología inespecífica y necesidad de cirugía diagnóstico-terapéutica en gran
número de casos. Se denominan primarios cuando asientan en una glándula sana, y secundarios cuando la misma tiene una enfermedad preexistente. La infección se
desarrolla por vía hematógena, por contigüidad o por mecanismos no evidentes. La
Palabras clave: Absceso de hipófisis, infección intracraneana.
ABSTRACT: Arch Med Interna 37(3):
Pituitary abscess is a rare disease, is less than 1% of the sellar pathology, with high
diagnostic difficulty, little clinical counselor, nonspecific imaging and diagnostic-
therapeutic need surgery in many cases. Are called primary when seated in a healthy, and secondary when the same side gland has a preexisting condition. The infection develops through the blood, contiguous or non-obvious mechanisms. The resolution must be urgently because the course is rarely. Two cases assisted in the course of a year and review of the literature is presented.
Introducción
El absceso de hipófisis o absceso selar se define como un proceso infeccioso dentro
de la silla turca con reacción inflamatoria aguda o crónica. Es infrecuente y representa el 1% de las patologías selares. Pocos cientos de casos han sido reportados en la literatura internacional.
Se plantean tres orígenes posibles para su desarrollo: 1) complicación de lesiones preexistentes 2) por extensión directa o por vía hematógena 3) sin fuente de infección clara. Los abscesos selares se clasifican en primarios cuando se desarrollan sobre una glándula sana, y secundarios cuando lo hacen sobre una glándula con patología subyacente.
Las manifestaciones clínicas remedan otras afecciones hipofisarias, con signos y
síntomas de compresión quiasmática y disfunción glandular.
La Tomografía Axial Computarizada (TAC) de cráneo es poco específica y sensible, aunque la calidad de las imágenes ha mejorado con los nuevos tomógrafos disponibles.
La Resonancia Nuclear Magnética (RNM) es el estudio de elección frente a la sospecha de una lesión selar, ya que puede identificar una anomalía intraselar hiperintensa en T2 que sugieren la presencia de una lesión quística contaminada, realzando en anillo en la periferia al administrar gadolinio. La interpretación de las imágenes se dificulta aún más si existe un tumor subyacente o cirugías selares previas. De todos modos no existen características definidas dada la poca experiencia en esta patología.
El tratamiento debe ser urgente dado que la evolución es impredecible pudiendo
ocasionar un rápido deterioro del estado de conciencia, falla endocrina, ruptura del absceso al espacio subaracnoideo y espasmo de la carótida interna en el seno
Frente al hallazgo del absceso o si existe sospecha previa, deben asociarse antibióticos de amplio espectro y soporte endocrinológico.
La tasa de mortalidad es alta, cercana al 28% cuando no asocia meningitis y se eleva a 45% cuando si la asocia.
Se describen dos casos clínicos de abscesos hipofisarios asistidos en un período de
un año. El caso clínico 1 fue asistido en una institución privada (CASMU) y el caso clínico 2 en un hospital público (Hospital Pasteur). A partir de los mismos se realiza una revisión de la literatura.
Caso 1
Paciente de sexo femenino, 66 años, sin antecedentes personales a destacar.
decaimiento y un episodio de pérdida de conocimiento catalogado como sincopal.
Sin cuadro febril previo. No presenta cefalea, trastornos visuales ni síntomas
neurológicos deficitarios. El examen físico al momento del ingreso es normal.
De la valoración paraclínica se objetiva una hiponatremia mantenida de 119
mEq/l con natriuresis de 203 mEq/24hs y osmolaridad plasmática de 280 mOsm/kg.
Con planteo de síndrome de secreción inadecuado de hormona antidiurética (SIADH) se realiza TAC de cráneo que evidencia en la silla turca un proceso sólido,
redondeado, de contornos netos de aproximadamente 15 mm de diámetro,
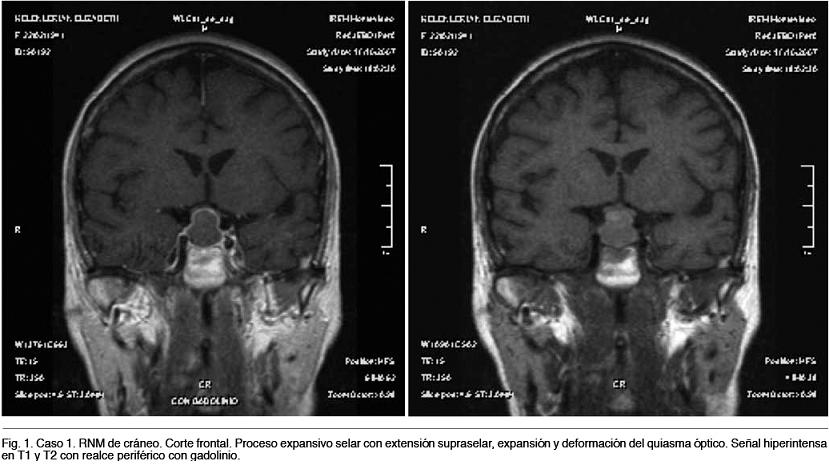
heterogéneo de mayor densidad que el parénquima encefálico. La RNM de cráneo
deformación del quiasma óptico que deforma el piso de la silla turca. Presenta señal
hiperintensa en T1 y T2, que luego de la administración del medio de contraste
evidencia realce a nivel de la cápsula (Figura 1).
La campimetría evidenció un denudamiento de la mancha ciega en ambos ojos.
El estudio hormonal para la valoración endocrinológica de la glándula mostró que las hormonas folículo estimulante (FSH), adrenocorticotrofa (ACTH) y estimulante de la tiroides (TSH) estaban dentro de rangos normales, mientras que la prolactina era de 31,3 ng/mL (levemente aumentada).
Del resto de la paraclinica se destaca una velocidad de eritrosedimentación (VES) 73 mm/1er hora, proteína C reactiva (PCR) 41,1 mg/l, plaquetas 660.000/mm3,
En función de los hallazgos se planteó adenoma hipofisario no secretante.
En cuanto al tratamiento se corrigió la natremia mediante aporte de sodio intravenoso y restricción hídrica, normalizándose la misma a los pocos días.
Se realiza resección quirúrgica por abordaje transesfenoidal clásico, obteniéndose a través de la incisión de la duramadre del piso selar en forma espontánea material purulento, se toman muestra para cultivo y se procede a lavar la zona quirúrgica.
El diagnóstico definitivo intraoperatorio fue de absceso hipofisario, dando inició a tratamiento antibiótico empírico con Ceftriaxona 2gr i/v cada 24 hs y Metronidazol 500mg i/v cada 8 hs que se mantienen por 6 semanas.
Los cultivos del absceso y los hemocultivos no desarrollaron bacterias.
El ecocardiograma transesofágico no mostro vegetaciones ni imágenes compatibles con endocarditis.
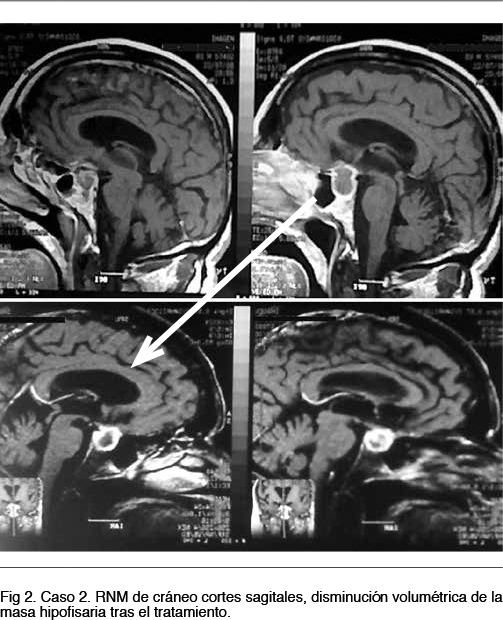
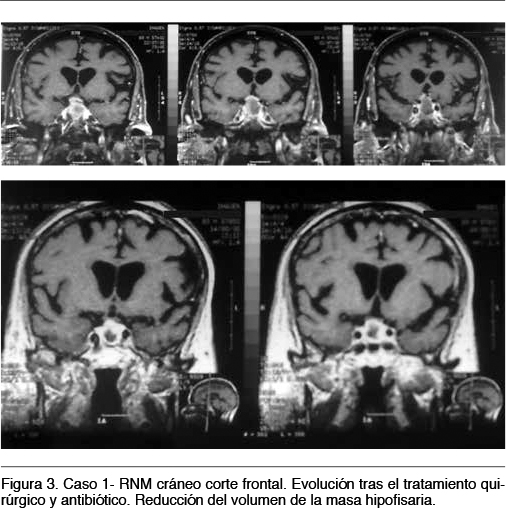
Al finalizar el tratamiento, se asistió a un descenso de los parámetros reactivos al proceso infeccioso con VES de 54mm/1era hora, plaquetas de 166.000/mm3. Asimismo se normalizó el valor de prolactina (8,6 ng/mL) y la RNM de cráneo evidenció drenaje de la colección intraselar con realce periférico de la glándula de tamaño habitual, sin evidencia de colecciones intraselares (Figura 2 y 3).
Caso 2
Paciente de 83 años, sexo masculino, antecedentes personales: diabetes mellitus tipo 2 en tratamiento con Metformina 850 mg/día, con buena adherencia y buen control metabólico. Consulta por cuadro de una semana de evolución dado por tos,
estertores crepitantes en cara posterior de hemitórax derecho, confirmándose con la radiografía de tórax un foco de condensación en lóbulo inferior derecho.
Con planteo de neumonía comunitaria se realizan hemocultivos que resultan negativos y se inicia tratamiento antibiótico con Ampicilina –sulbactam 1,5 gr i/v cada 6hs y Claritromicina 500mg v/o cada 12hs.
A las 48 horas del ingreso instala cefalea holocraneana, náuseas y vómitos reiterados. El examen neurológico muestra un paciente lúcido, bien orientado en tiempo y espacio, sin alteraciones de las funciones simbólicas, sin alteraciones de los pares craneanos, sin rigidez de nuca y sin alteraciones del sector espinal.
Tras la búsqueda de esta situación clínica se realiza glucemia, ionograma azoemia,
creatininemia y hemograma que son normales.
El análisis del líquido cefalorraquídeo (LCR) muestra: aspecto turbio, pandy+++,
glucosa: 0,53 mg/dl, proteínas: 3,5g/dl, glóbulos rojos: 20/mm3 conservados, glóbulos blancos: 7/mm3. Cultivo bacteriológico del líquido sin desarrollo. PCR para grupo herpes virus negativo. VDRL negativo
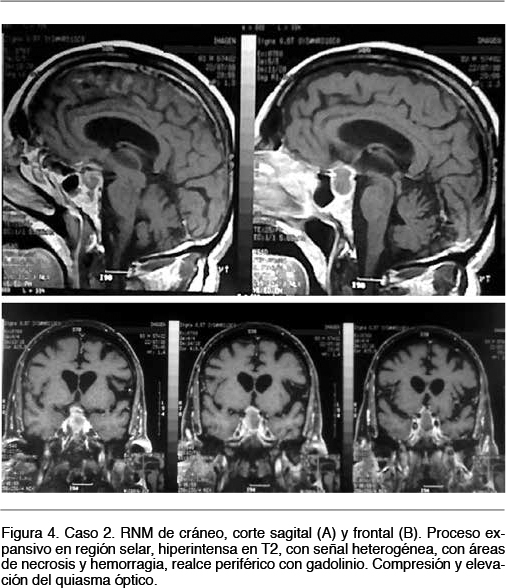
Frente a este hallazgo de proceso inflamatorio intracraneano se procede a realizar TAC de cráneo que mostro silla turca ocupada por proceso redondeado de 4mm. Se completo valoración con RNM de cráneo que evidencia voluminoso proceso expansivo que ocupa la silla turca que determina elevación y compresión del quiasma óptico. La intensidad de la señal del proceso es heterogénea con áreas de necrosis hemorrágica y realce más intenso en su periferia (Figura 4).
Por las características imagenológicas y el contexto inflamatorio-infeccioso se planteó como diagnostico primario un absceso hipofisario.
La valoración endocrinológica mostró TSH 0,17 mUI/mL (normal 0,23 - 4,20), T4 1,55 ng/dl (normal 0,85 -1,70), ACTH, FSH, LH, y prolactina en rango normales.
Ampicilina 3gr i/v cada 6hs por 6 semanas.
El paciente presenta mejoría de los síntomas a partir del quinto día de tratamiento, sin nuevas manifestaciones neurológicas.
Al finalizar el tratamiento antibiótico se realiza control de las hormonas tiroideas que son normales y RNM de cráneo que muestra franca reducción del proceso selar.
Discusión
Los abscesos de hipófisis son una entidad poco frecuente que comprende menos del
1% de la patología hipofisaria y menos del 0,27% de los tumores hipofisarios (1 - 2), descrito por primera vez por Simmonds en 1914 y definido como la localización intraselar de un proceso supurativo (3).
Entidad de alta dificultad diagnóstica, por presentarse con una clínica ambigua donde sólo un tercio de los pacientes evidencian signos y síntomas sugestivos de infección, donde las imágenes no son patognomónicas del proceso y los cultivos tienen tan sólo un rendimiento del 50% (1). Es sin embargo una patología con una mortalidad no despreciable lo que implica una tenaz consideración y sospecha diagnóstica junto con la valoración oportuna mediante RNM como técnica “gold standard” sabiendo que de todas formas la amplia mayoría de las veces la confirmación únicamente se da tras el procedimiento quirúrgico que obtiene la muestra purulenta (4) tal como ocurrió en el primer caso clínico.
Si bien la clásica tríada sintomática de cefalea, alteraciones visuales y fiebre (5) no fue objetivada en ninguno de los pacientes, el síntoma aislado más frecuente es la
cefalea, presente en el 60% de los casos (1), típicamente de evolución prolongada, de escaso alivio con analgésicos comunes y topografía bitemporal. Los síntomas de
hipertensión endocraneana como vómitos y náuseas junto con los de irritación
meníngea (fotofobia, acusofobia y limitación en la flexión de nuca) están presentes en el 25% de los pacientes (2,4). Estos últimos junto a la presencia de cefalea,
estuvieron presentes en el segundo caso clínico, siendo el hilo conductor para llegar al diagnóstico del proceso intracraneano.
La meningitis recurrente es una forma de presentación rara de esta enfermedad con pocos casos reportados hasta la fecha (6) y de muy difícil diagnóstico ya que habitualmente el líquido cefalorraquídeo resulta aséptico por la implementación precoz de tratamiento antibiótico (6).
Las alteraciones visuales presentes en hasta el 50% de los casos se deben al
compromiso del quiasma óptico y porciones proximales de los nervios ópticos (2,4).
Nuestros pacientes coincidían en la compresión objetivada por imágenes del quiasma óptico sin otra expresión clínica que el denudamiento de la mancha ciega bilateral observada en la campimetría en el primer caso clínico.
En las primeras descripciones, los abscesos selares eran secundarios a cuadros sépticos graves, pero en la actualidad esta situación es muy poco frecuente; siendo consecuencia de procesos primarios a partir de tres circunstancias (3):
a) Como extensión secundaria a la silla turca de infecciones de vecindad (sinusitis, meningitis e infecciones postoperatorias de abordajes transesfenoidales).
b) Como infecciones aparecidas en una silla turca comprometida por una lesión preexistente como adenoma de hipófisis, craneofaringiomas o quistes de la bolsa de Rathka.
c) Sin lesiones previas ni infecciones vecinas o sistémicas en actividad, constituyendo el grupo de abscesos primarios, algunos de los cuales cursan en inmunodeprimidos.
Proponemos por tanto que el primer caso se trata de un absceso primario ya que no se detectó un origen claro, y el segundo caso sea un absceso secundario con diseminación hematógena ya que estaba cursando una infección pulmonar aguda.
Los desórdenes endocrinológicos más frecuentes son: la amenorrea y el
panhipopituitarismo, presentes en hasta el 30-50% de los casos (2,4). Tal como se
describe en los dos casos clínicos, el primero presentó un aumento de la prolactina consecuente con la interrupción del eje de retroalimentación por compresión del tallo y el segundo paciente presentó únicamente descenso de la TSH, ambos casos mejoraron con el tratamiento del absceso hipofisario. En términos de frecuencia se afecta en primer lugar la secreción de hormona del crecimiento seguida por la de las hormonas sexuales, la TSH y la ACTH (2).
La presencia de manifestaciones sistémicas o marcadores de actividad infecciosa están presentes únicamente en el 24-33% de los pacientes (2,4), tal como observamos en los casos descritos donde únicamente el segundo paciente estuvo febril y fue en contexto del proceso infeccioso respiratorio.
realce en anillo o una masa isodensa con realce homogéneo en la silla turca (1), siendo sin embargo su principal aporte la valoración del compromiso de las estructuras óseas adyacentes. La RNM de cráneo es la técnica de elección para la valoración tanto de la morfología glandular como de los procesos infecciosos abscedados, podrá mostrar imágenes quísticas, con eventual extensión supraselar hipo o isointensas en T1, iso o hiperintensas en T2 con realce periférico tras la administración de gadolinio.
Clásicamente son imágenes que presentan restricción de la difusión, siendo éste un dato de importancia para el diagnóstico diferencial (4) principalmente y por frecuencia con el adenoma hipofisario. Éste fue el planteo diagnóstico inicial en el primer caso clínico siendo el diagnóstico definitivo de absceso hipofisario en el intra- operatorio al obtener material purulento, apoyando entonces lo descrito en las series internacionales en cuanto a la poca especificidad y certeza de la imagenología, ya que las imágenes descritas no son exclusivas del absceso hipofisario, además de ser variables en cuanto a su densidad e intensidad de realce en función de la cantidad de proteínas que contenga y la presencia de hemorragia.
En los próximos años la TAC con gallium-67 puede ser de ayuda para aproximar el diagnóstico (1), siendo actualmente de baja disponibilidad en nuestro medio.
Los cultivos desarrollan principalmente cocos gram positivos como Staphlococcus
aureus y Streptococcus pyogenes. Pseudomonas, Klebsiella, Bacteroides,
Acinetobacter, Candida albicans, gérmenes anaerobios, Entamoeba hystolitica, y
Brucella completan la amplia gama de gérmenes identificados (7); sin embargo el 50% de los cultivos resulta sin desarrollo lo que puede ser atribuido a la mala técnica de cultivo de agentes micóticos y anaerobios así como el inicio de antibiótico previo a la realización de la muestra (1,4). Algunos autores proponen, sin embargo, que esta entidad no sería infecciosa sino parte de una reacción tisular frente a un infarto de adenoma explicando con ello la escasa detección de gérmenes, la similitud clínica y la microbiología más prevalente siendo los cultivos positivos en mayor número de cirugías trans-esfenoidales frente a trans-craneales, sospechándose contaminación de la muestra (8).
Frente a la sospecha clínico- imagenológica de esta patología, la conducta quirúrgica frente a una conducta expectante ofrece beneficios en términos de prevención de progreso y deficiencia hormonal a largo plazo (2).
El tratamiento del absceso hipofisario incluye técnicas quirúrgicas, idealmente con
abordaje trans-esfenoidal tal como se practicó en el primero de los casos comentados, con evacuación, irrigación del lecho con soluciones con antibiótico y mantenimiento de drenaje de ser requerido con beneficio en cuanto a decompresión de quiasma óptico. La consideración integral de la situación biológica del segundo paciente condujo al equipo tratante a optar por una conducta menos invasiva que derivó afortunadamente en excelentes resultados.
El tratamiento quirúrgico en combinación con la antibioticoterapia sistémica dirigida
empíricamente contra los gérmenes planteados más frecuentes y ajustada según
resultado de cultivo y técnicas de resolución de procesos locales (en caso de
colecciones) son los pilares que sustentan una terapia combinada para esta patología compleja. Los antimicrobianos tienen indicación inicialmente de 2 a 6 semanas (1,9). En ambos reportes se realizó antibioticoterapia por seis semanas, con un excelente evolución tanto en lo sintomático como en lo imagenológico con resolución objetivada de ambos hechos.
Actualmente la mortalidad se ha reducido a menos del 10% (8). EL seguimiento debe ser estrecho y a largo plazo por el riesgo de recurrencia (2).
Conclusiones
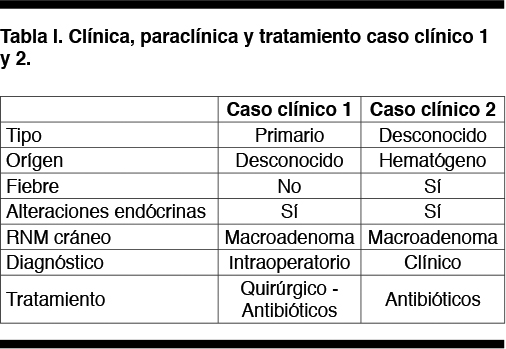
Los abscesos de hipófisis son una patología de muy baja incidencia y difícil diagnóstico tal como podemos entender a partir de los dos casos clínicos descritos.
La imagenología es poco específica, lo que determino la decisión de intervención
quirúrgica con el planteo de adenoma hipofisario en el caso 1, surgiendo el diagnóstico en el intra-operatorio. En el caso 2 la situación clínica y los hallazgos
imagenológicos realizaron la sospecha diagnóstica. En la tabla 1 se presentan las
como ocurre en más de la mitad de los casos. El tratamiento antibiótico prolongado
permitió la resolución del proceso. La evolución fue favorable con recuperación total de síntomas y de las alteraciones hormonales presentes, aún para el paciente que recibió un tratamiento conservador.
Agradecimientos
Al Profesor Agregado Dr. Alvaro Díaz Berenguer por su generosidad y experiencia.
1- Su YH, Chen Y, Tseng SH. Pituitary abscess. J Clin Neurosci. 2006; 13: 1038-41.
2- Dalan R, Leow MK. Pituitary absess: our experience with a case and a review of the literature. Pituitary. 2008;11: 299-306.
3- Wilson E, Aboal C. Absceso intraselar primario. Arch Inst Neuro. 2000; 3: 102-105.
4- Shuster A, Gunnarsson T, Sommer D, Miller E. Pituitary abscess: an unexpected diagnosis. Pediatr Radiol. 2010; 40: 219-22.
5- Altas M, Serefhan A, Silav G, Cerci A, Coskun KK, Elmaci I. Diagnosis and management of pituitary abscess: a case series and a review of the literature. Turk
Neurosurg. 2013, 23: 611-16.
6- Walia R, Bhansali A, Dutta P, Shanmugasundar G, Mukherjee KK, Upreti V, et al. An uncommon cause of recurrent pyogenic meningitis: pituitary abscess.
BMJ Case Rep. 2010; 2010.
7- Carpinteri R, Patelli I, Casanueva FF, Giustina A. Pituitary tumours: Inflammatory and granulomatous expansive lesions of the pituitary. Best Pract Res Clin Endocrinol Metab. 2009; 23:639-50.
8- Galicia I, Orea I, Abad A, Aragón A, García-Durruti P, Ley L, et al. Abscesos
hipofisarios: estudio de siete casos. Endocrinol Nutr. 2005; 52: 152-6.
9- Zhu H, Gu XM, Hong J, Shen FX. Successful treatment of pituitary abscess with intravenous antibiotics: a case report and literature review. Genet Mol Res. 2014;
13: 10523-28.
{kind=link}