










Servicios Personalizados
Revista

Articulo
 texto en
texto en  Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
Links relacionados
Compartir

 Permalink
PermalinkEnfermería: Cuidados Humanizados
versión impresa ISSN 1688-8375versión On-line ISSN 2393-6606
Enfermería (Montevideo) vol.12 no.2 Montevideo 2023 Epub 01-Dic-2023
https://doi.org/10.22235/ech.v12i2.3329
Original Articles
Realistic simulation as a training strategy for the health team
1
 http://orcid.org/0000-0001-8593-4539
http://orcid.org/0000-0001-8593-4539
2
http://orcid.org/0000-0001-9862-6279
3
http://orcid.org/0000-0002-6043-9301
1 Universidade Estadual de Londrina, Brasil, kelenmitie.ms.ue@gmail.com
2 Universidade Estadual de Londrina, Brasil
3 Universidade Estadual de Londrina, Brasil
4 Universidade Estadual de Londrina, Brasil
5Universidade Estadual de Londrina, Brasil
To assess realistic simulation as a training strategy for nursing technicians and ambulance drivers in the primary assessment of trauma cases
.A quasi-experimental study, before-and-after design, with a quantitative approach, conducted between December 2021 and March 2022. The study population consisted of 98 professionals from 14 municipalities within the Northern region of the State of Paraná, who are part of the Regulatory Complex of the Mobile Emergency Care Service. A knowledge test consisting of 10 questions was administered before and after the simulation. Data were analyzed in terms of central tendency and dispersion. Pre-test and post-test correct answers were compared as percentages. The mean and standard deviation of correct answers were assessed using the Shapiro-Wilk test to determine whether the data followed a normal distribution. The Wilcoxon test was also employed to identify differences in mean correct answers between the research phases, with a significance level of 0.050.
Among the proposed questions, those related to trauma kinematics, stages of primary victim assessment, treatment planning, victim immobilization, assessment during care, and recognition of shock achieved a 90% correct response rate after the training. Questions about primary patient assessment and airway management also yielded significant results
.The assimilation of knowledge through realistic simulation led to a significant improvement in correct answer rates for the questions
Keywords: simulation training; training; trauma; licensed practical nurses; ambulance drivers
Objetivo:
Avaliar a simulação realística como estratégia de capacitação de técnicos de enfermagem e condutores de ambulância na avaliação primária dos traumas.
Método:
Estudo quase experimental, tipo antes e depois, abordagem quantitativa, desenvolvido entre dezembro de 2021 a março de 2022. A população constitui-se de 98 profissionais de 14 municípios que compõem o Complexo Regulador do Serviço de Atendimento Móvel de Urgência, da região norte do Estado do Paraná. Foi aplicado um teste de conhecimento, com 10 questões, antes e depois da simulação. Os dados foram avaliados em relação à medida central e dispersão. Os acertos, no pré e pós-teste, foram comparados por percentual. A média e desvio padrão dos acertos foram avaliados empregando o teste de Shapiro-Wilk para identificação da distribuição normal, ou não, dos dados. Também foi realizado o teste de Wilcoxon para identificação de diferença entre as médias de acertos entre os momentos de pesquisa. Empregou-se o índice de significância de 0,050.
Resultados:
Das perguntas propostas, aquelas sobre cinemática do trauma, estágios da avaliação primária da vítima, planejamento do atendimento e imobilização da vítima de trauma, atendimento na avaliação e presença de choque atingiram 90% das respostas corretas esperadas após o treinamento. As perguntas sobre avaliação primária do paciente e manejo das vias aéreas também produziram resultados significativos.
Conclusão:
A assimilação de conhecimento através da simulação realística promoveu um incremento importante de acertos das questões.
Palavras-chave: treinamento por simulação; capacitação; trauma; técnicos de enfermagem; condutores de ambulância
Objetivo:
Evaluar la simulación realista como estrategia de formación de técnicos de enfermería y conductores de ambulancias en la valoración primaria del trauma.
Método:
Estudio cuasiexperimental, tipo antes y después, enfoque cuantitativo, desarrollado entre diciembre de 2021 y marzo de 2022. La población está compuesta por 98 profesionales de 14 municipios que componen el Complejo Regulador del Servicio de Atención Móvil de Emergencia de la región norte del Estado de Paraná. Se aplicó una prueba de conocimientos, con 10 preguntas, antes y después de la simulación. Los datos fueron evaluados en relación con la medida central y dispersión. Las respuestas correctas, en el pre y postest, fueron comparadas por porcentaje. La media y la desviación estándar de las respuestas correctas se evaluaron mediante la prueba de Shapiro-Wilk para identificar la distribución normal o no de los datos. También se realizó la prueba de Wilcoxon para identificar la diferencia entre las medias de aciertos entre los momentos de la investigación. Se utilizó un índice de significación de 0.050.
Resultados:
De las preguntas propuestas, aquellas sobre cinemática del trauma, etapas de la valoración primaria de la víctima, planificación del cuidado e inmovilización de la víctima del trauma, atención en la valoración y presencia de shock alcanzaron el 90 % de respuestas correctas esperadas después el entrenamiento. Las preguntas sobre evaluación primaria del paciente y control de la vía aérea también arrojaron resultados significativos.
Conclusión:
La asimilación de conocimientos a través de la simulación realista promovió un aumento importante en las respuestas correctas a las preguntas
Palabras clave: entrenamiento simulado; capacitación; trauma; enfermeros no diplomados; conductores de ambulancia
Introduction
Car accidents rank as the 9th leading cause of death globally, with trauma being the primary contributor, accounting for approximately 4% of worldwide fatalities. According to a 2018 report by the World Health Organization (WHO), in 2016, an estimated 1.35 million people lost their lives due to car accidents worldwide, equating to one death every 23 seconds. 1 In Brazil, trauma stands as a critical public health concern due to its significant impact on morbidity, mortality, and its ripple effects on the economy and society as a whole. As such, it warrants careful attention and comprehensive care at all levels of the healthcare system. 2)
Trauma refers to physiological disruptions or disorders resulting from the exchange of energy between the body and the environment. Throughout history, traumatic injuries have been documented in wartime scenarios, and as societies have progressed, other forms of trauma have emerged, marked by their severity and complexity. Examples include car accidents, pedestrian accidents, falls from heights, slips and falls, physical assaults, burns, and bicycle accidents. These incidents can lead to fatalities at different intervals, underscoring the importance of early intervention, which can significantly impact a patient's chances of survival. 3
The pre-hospital care service (PHC) delivers mobile medical assistance, equipped with the necessary materials and tools to respond to emergencies on public roads, in residences, businesses, on highways, and other locations outside the hospital setting. The PHC team must be well-versed in care protocols, possess the necessary skills, exhibit agility, and be prepared to address the diverse scenarios that arise in pre-hospital settings. Their role is to ensure the preservation of vital functions and provide emotional support until the patient reaches the hospital. 4
A study conducted by Farias et al. 5 shed light on the vulnerabilities of primary care nursing and medical teams when it comes to managing urgent and emergency situations. Many of them felt unprepared and not accountable for such demands, largely due to their PHC units being based in Basic Health Units (UBS) with inadequate and unsuitable infrastructure. This situation leads to an increased burden on healthcare facilities when faced with highly complex cases.
In the realm of pre-hospital care, professionals must possess the necessary knowledge, skills, and critical thinking abilities to facilitate effective decision-making and enhance the survival prospects of trauma victims. Providing essential care in pre-hospital settings is paramount, as trauma can shatter lives, often extinguishing dreams and productive years while imposing significant social and economic burdens on victims and their families. Consequently, the professionals working in pre-hospital care sometimes hold the responsibility for extending or curtailing the life expectancy and productive years of a trauma patient. 6
Continuing in-service education emerges as a crucial strategy to address the lack of preparedness and uncertainty among these professionals. They must remain ready and poised to deliver optimal care in various urgent and emergency situations. 7 When selecting educational strategies, the use of realistic simulation has gained recognition among researchers due to its applicability in healthcare training. These simulations contribute to various aspects, including clinical competence, cognitive and psychomotor development, knowledge reinforcement, technical skill acquisition, and the cultivation of critical thinking and self-reflection among professionals who undergo simulation-based training. 8,9
With this conceptual foundation, this study aims to assess the effectiveness of realistic simulation as a training strategy for nursing technicians and ambulance drivers in the primary pre-hospital assessment of trauma.
Method
For the development of this research, a two-phase intervention was conducted with a quantitative approach. To document this research, a quasi-experimental pre-test and post-test design was employed, following the guidelines outlined in the Consolidated Standards of Reporting Trials (CONSORT) framework. 10 The study was carried out at Pole B of a SAMU Regulatory complex in the northern region of the state of Paraná, comprising 14 municipalities. Approximately 60 professional nursing technicians and 60 ambulance drivers, who worked in small hospitals within these municipalities and provided urgent and emergency care, including trauma cases on the roads surrounding the municipalities, were invited to participate. A total of 98 professionals, consisting of 50 nursing technicians and 48 ambulance drivers, took part in the study, which occurred between December 2021 and March 2022.
The training program, titled "Realistic Simulation: A Tool for Primary Trauma Care Training," was initially introduced via telephone communication to the municipal managers, where the training project was briefly outlined. Subsequently, a formal invitation and schedule were sent to the managers via institutional email.
Each manager submitted the names of the participants, who were then scheduled based on their personal availability. Eight training sessions were conducted in separate sessions, each lasting eight hours per training day with a two-hour break in between. The sessions consisted of a pre-briefing, during which essential guidelines and necessary items for each phase were presented, a review of the trauma care protocol, and simulation exercises. Each session accommodated a maximum of 20 participants. Professionals who had registered but missed the training sessions were considered as losses.
The training program adhered to the principles of realistic simulation as proposed by Jeffries 11 and followed the three key stages. The first stage, the briefing, involved providing participants with basic instructions, including a description of the scenario or case, before they commenced their role in the simulated scenario. The simulated scenario itself was the phase in which the designated case was acted out. Participants were required to administer care, and the facilitator (researcher) provided guidance when necessary. The outcome of the case was contingent upon the participant's intervention. The debriefing stage was the final phase, taking place after the simulation, during which the facilitator guided participants in reflecting on the care provided. Participants assessed their resourcefulness and identified positive and negative aspects, areas for improvement, and elements to maintain concerning their care.
At all the training sessions, the researcher presented the research objectives, provided instructions on how to complete the Free and Informed Consent Form to participate in the study, and collected data with the assistance of a team of ten previously trained professionals. Data collection occurred in two stages: 1) Sociodemographic and professional characterization, involving the completion of a form containing variables such as gender, age, marital status, cohabitation, municipality of origin, educational background, work regime, and prior participation in a trauma care course; 2) Following the completion of this form, the knowledge assessment pre-test was administered.
The knowledge test was based on a bibliographic survey and the American College of Surgeons’ international protocols - Pre-Hospital Trauma Life Support (PHTLS) 6 and Advanced Trauma Life Support (ATLS), 12 with the most up-to-date data collection. "The knowledge assessment instrument, originally developed by Almeida 13 and initially administered to undergraduate nursing students, underwent modifications to accommodate mid-level professionals due to the complex nature of certain content-related terms. To adapt this assessment tool, a panel of experts was assembled using intentional sampling, following Pasquali's guidelines (14), which recommend a minimum of six experts. These experts were required to possess specialized knowledge within their respective fields, ensuring their comprehensive understanding of the content being analyzed. The selection process also required an 80% agreement rate among the panel members regarding the content. The expert panel comprised two Ph.D. nurses in nursing, a master's-level nurse in nursing, a master's student in nursing, and an intensive care nursing resident- all seasoned professionals in pre-hospital care and specialists in Urgency and Emergency. They made minor adjustments to the phrasing of the questions without altering the underlying content.
The knowledge assessment/pre-test was administered individually via a questionnaire featuring ten multiple-choice questions pertaining to primary trauma care content. The questions were designed to evaluate the following aspects in alignment with the PHTLS primary trauma assessment protocol mnemonic: 1) trauma kinematics: an essential criterion for assessing and recognizing potential injuries; 2) primary assessment of the trauma patient: comprehension of the trauma care protocol.; 3) stages of the primary assessment: the professional's ability to correctly sequence the assessment steps based on the XACDE mnemonic; 4) planning for the care of the trauma victim: the professional's actions to ensure safe care; 5) control of exsanguinating hemorrhage: the assessment of injuries, blood loss evaluation, and decision-making regarding hemorrhage control; 6) airway control: understanding when to assess the airway and how to ensure control and patency; 7) immobilization of the trauma patient: assessing and determining the need for spinal movement restriction; 8) care for suspected chest trauma: recognizing and addressing chest trauma based on assessment findings, signs, and symptoms; 9) care in the assessment and presence of shock: identifying signs of shock and managing bleeding; 10) Assessment of neurological dysfunction in the trauma victim: the correct application of the Glasgow Coma Scale. Each question carried a value of one (1) point, with a maximum achievable score of 10 points for professionals providing all correct answers. Additionally, professionals were asked to indicate their level of confidence in their answers before the intervention.
After applying the knowledge test/pre-test, in the first stage of the pre-briefing, the group took part in theoretical and practical training, using the XABCDE mnemonic, presented in the PHTLS, for the primary assessment of trauma care: X = exsanguinating hemorrhage, A = airway, B = breathing, C = circulation, D = neurological dysfunction and E = exposure of the victim. In the sequence of the letters, each one corresponds to the assessment of the victim to be carried out by the participant. After this stage, the participants were given a two-hour break. 6
The pairs of participating professionals -an ambulance driver and a nursing technician- were grouped by affinity or place of work and then took part in the simulation.
In the second stage, the briefing, each pair of professionals was given the situation of the incident in a separate room, as if they were at the base, i.e., the report of the case that would be attended to in the simulation. They were then told that the team had 10 minutes to carry out the service. The pair went to the simulated scenario, which was set up on the sports field of a school where the training was held.
A standardized patient was employed to portray the trauma victim at the scene, following a predetermined script, and was trained to adapt to potential variations in care scenarios. In the simulation, the victim was depicted lying beside a motorcycle, unresponsive, exhibiting noisy breathing caused by a partial airway obstruction simulated with artificial blood, sporting a hematoma behind the left ear, a periorbital hematoma resulting in raccoon eyes, pallid skin, an open wound on the left hemithorax, and several minor bloody abrasions distributed across the body (make-up was utilized to replicate diverse injury types). This portrayal necessitated the application of primary trauma care.
Following their participation in the simulation, each professional pair proceeded to the third phase, the debriefing, which lasted for 20 minutes. During this session, each participant had the opportunity to share their experiences, elaborate on their successes, identify areas for potential improvement in their performance, and express any uncertainties related to the primary trauma care simulation. Drawing from the "good judgment" model 15, participants were encouraged by the facilitator to articulate their emotions that influenced their actions during the simulation. In instances where participants encountered challenges, they received support to help them reframe their emotional responses for future care scenarios.
Subsequently, all participants in the simulation underwent a post-test to assess their knowledge. This post-test was conducted individually and featured 10 multiple-choice questions identical to those from the pre-test. The post-test was administered in a private setting, with supervision provided by an internal support person.
Throughout the training process, which encompassed lectures, simulation exercises, and debriefing sessions, a total of 99 participants initially engaged in the lectures. However, only 98 ultimately participated in the simulation and debriefing, as one participant dropped out of the realistic simulation training process.
The data were analyzed using measures of central tendency and dispersion for continuous variables, as well as absolute and relative values for categorical variables. We compared the percentage of correct answers in both the pre-test and post-test. To assess the mean and standard deviation of correct answers at both survey time points, we employed the Shapiro-Wilk test to determine whether the data followed a normal distribution. Finally, we utilized the Wilcoxon test to identify differences in the average number of correct answers between the survey time points. A significance level of ≤ 0.050 was applied.
This research received authorization from all participating municipalities and obtained approval from the Research Ethics Committee (CEP) of a public university in Paraná. The approval was granted under Opinion No. 4.880.119 and CAE No. 28941520.3.1001.5231, version 3.
Results
A total of 98 health professionals who provided Basic Life Support (BLS) in ambulances in the 14 municipalities took part in the study. Of this total, 48 were nursing technicians and 50 were ambulance drivers.
Table 1 shows the sociodemographic and professional characterization of the participants.
Table 1: Sociodemographic and professional characterization of the participants
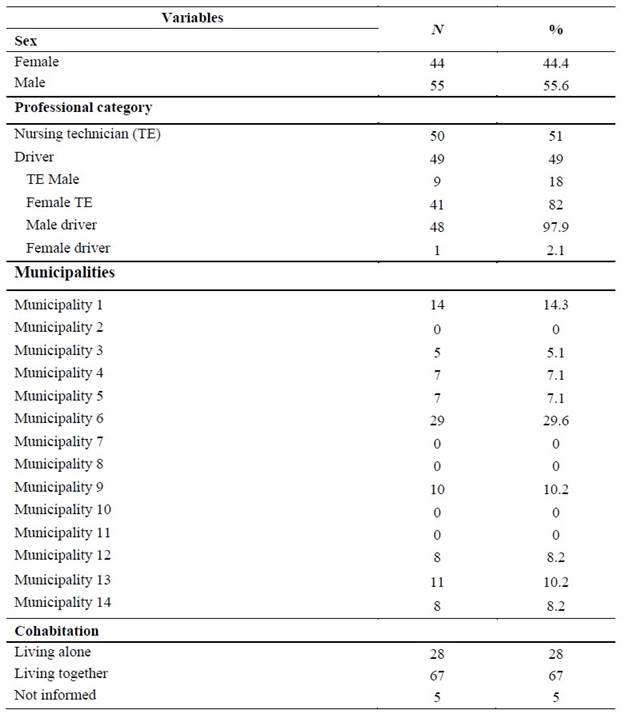
Source: Own elaboration (2023)
Out of the 14 municipalities invited to participate in the training, municipality six had the highest number of professionals (29), while municipalities two, seven, eight, 10, and 11 had no participants. This resulted in the involvement of nine municipalities comprising Pole B of a SAMU Regulatory Complex in the northern region of the state of Paraná.
The composition of the participants revealed a predominance of females among nursing technicians (82%) and males among drivers (97.9%). The average age of the professionals was 44.9 years. The majority of the professionals held statutory employment contracts (87.6%), with a smaller percentage on temporary employment contracts (12.6%). A small percentage of data (4%) was missing.
In terms of educational qualifications, most professionals did not hold a university degree (59.2%), and 54.5% had not attended a trauma care course. Additionally, 53.1% reported that they did not feel adequately qualified to provide trauma care.
Regarding their self-perceived knowledge of trauma care, 52.5% considered themselves poorly trained, 38% believed they were well trained, and 9.1% viewed their training as inadequate.
Figure 1 displays the proportion of correct answers to questions in the knowledge assessment pre-test and post-test. A normality test revealed that the data exhibited a non-parametric distribution. Consequently, the Wilcoxon test was employed to identify paired differences between the two study time points, yielding a p-value of <0.001. This indicates a significant difference between the two study time points.
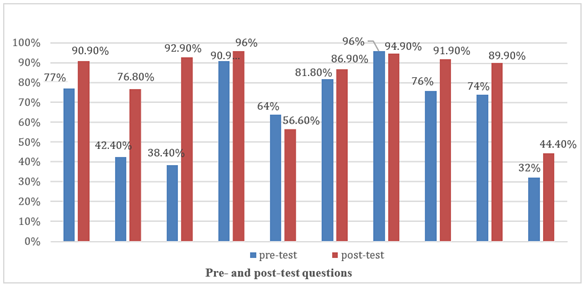
Figure 1: Proportion of correct answers in the pre-test and post-test on the topic of primary trauma care
Regarding the results, the topic of trauma kinematics exhibited improvement when comparing the two assessment moments. In the pre-test, 77% of the answers were correct, which subsequently increased to 90% in the post-test. Notably, there was a significant enhancement in this area.
In terms of the primary assessment stage, the pre-test initially yielded a correct response rate of 42.4%, whereas in the post-test, this percentage surged to 92.9%. This substantial improvement underscores the effectiveness of the training.
Concerning team planning for trauma care, the initial accuracy rate was 90.6%, which further improved to 96% in the post-test. The correct approach to immobilizing trauma victims consistently remained above 90% in both assessment phases.
In the first knowledge assessment, 76% of respondents answered correctly regarding care for victims with suspected chest trauma. In the second assessment, this percentage rose to 91%, indicating increased proficiency in this area. Similarly, in the evaluation of care in the presence of shock, the initial knowledge rate stood at 74%, while the second assessment showed a remarkable improvement, with 89.9% of correct answers on the subject.
In summary, the majority of the ten questions posed achieved the expected scores following the training. While the questions related to the primary assessment of trauma patients and airway control did not reach the same percentage of correct responses, there was noticeable improvement in knowledge acquisition when employing the realistic simulation method among BLS professionals in trauma care.
Discussion
Of the total of 98 professionals taking part, the survey showed a balance between the number of professional categories taking part, 51 % and 49 % of nursing technicians and ambulance drivers, respectively. This balance contributed to the smooth running of the training, given that the simulation activities were carried out in pairs, with one ambulance driver and one nursing technician. The research described by Oliveira et al. 16 on cardiopulmonary arrest, for BLS professionals from the Mobile Emergency Care Service (SAMU), showed a similar percentage of professionals.
Regarding the gender of the professionals, women (80 %) predominated among the nursing professionals, demonstrating the strength of women in nursing work, as seen historically, and corroborating the data presented by the Federal Nursing Council. 17 Oliveira et al.’s research 16 also showed that women were in greater numbers in the same professional category as the SAMU teams studied.
The category of ambulance drivers in this study showed that 97.9 % were men, as the work of this professional requires driving skills, strength in activities that require immobilization, transport and handling of the transport stretcher, especially when the weight and strength are too high. However, 2.1 % of women performed the same job. This activity is expanding for women, because in the National Register of licensed drivers in Brazil, by December 2022, there were 3.21 % of women licensed with a D license (license for transport that accommodates more than eight passengers), which is one of the criteria for driving ambulances. 18 Oliveira et al.’s research 16 showed 100% men in this activity and attributed this to the fact that men are more dynamic, rational and physically strong.
It is important to note that this study showed that 96 % of the professionals planned their trauma care and always checked their materials at the beginning of their shifts, making sure they had the necessary materials for trauma care, as described in the Basic Life Support Protocol, 19 PE3 - practices for patient safety, item four, which deals with practices for safe procedures, and item eight, prevention of falls and accidents.
It is noteworthy that it was possible to observe that, at first, the professionals had difficulties with the stages of the primary assessment. Thus, simulation training based on the National Association of Emergency Medical Technicians (NAEMT) has the mission of training professionals for the Emergency Medical Services (EMS), in order to improve victim care through quality in-service education, improving the skills of professionals.
The PHTLS trauma care protocol describes the primary assessment of trauma, with an emphasis on exsanguinating hemorrhages, which has been an integral part of the training program since 2019. It prioritizes the XABCDE mnemonic, serving as a standardized guideline for prioritizing actions based on the imminent risks to trauma victims' lives.
This research demonstrated enhanced comprehension of topics related to the primary assessment of trauma patients and their respective stages, care for suspected chest trauma, and management of shock. Realistic simulation, incorporating briefing, simulation, and debriefing stages, played a pivotal role in significantly enriching the understanding of trauma care protocol components.
Thus, the letter “X” refers to the detection of injuries with exsanguinating hemorrhages that require immediate intervention by the APH professional. In the context of exsanguinating hemorrhage control, it was evident that professionals lacked sufficient skills in managing hemorrhages due to a lack of familiarity with the updated trauma care protocol. This protocol emphasizes the criticality of addressing severe hemorrhages, particularly arterial hemorrhages, which can lead to rapid deterioration in a victim's condition. Early recognition of bleeding in trauma patients is paramount in preserving blood volume and the body's ability to maintain organ function. (6
Despite addressing identification and control of exsanguinating hemorrhages in the questionnaire, there was limited improvement in participants' understanding of this topic. Similar challenges were identified in a study by Santos et al. 20 where professionals showed difficulty in identifying injuries and delays in treating bleeding during simulations.
Stage A, which entails airway assessment and spinal movement restriction as necessary, did not exhibit significant changes in participants' performance, suggesting prior familiarity with this procedure. However, continuous reassessment of the victim's condition is crucial to ensuring safety throughout the assessment process.
In the pre-hospital setting, spinal movement restriction is necessary for trauma victims with altered levels of consciousness, aligning with the Prehospital Trauma Life Support (PHTLS) 6) guidelines. Participants understood the importance of spinal movement restriction, considering possible spinal injuries based on trauma kinematics and thorough physical examinations.
Before deciding whether or not to restrict spinal movement, the victim should be constantly reassessed to ensure greater safety at all stages of the assessment, and any changes in the signs and symptoms of the victim can be intervened upon at any time. You should always take into account the chance of there being a spinal injury that needs to be treated, and the restriction of spinal movement applied. 6 In their study, Oliveira et al. 16 noted that a significant number of professional first responders also recognized items in the protocol, even before the training, which was considered to be a positive impact of the study.
Airway control assessment, which constitutes stage C, saw a modest improvement from 81.8% to 86.9% in participants' understanding following the realistic simulation. In stage C, peripheral perfusion, capillary refill time, skin color, and humidity are assessed, and immediate intervention is required if any abnormalities are detected. 6
The penultimate stage, stage D, guides professionals in conducting a neurological assessment using the Glasgow Coma Scale (GCS). Although participants demonstrated improved comprehension of this care, it remains a complex topic, necessitating ongoing guidance and supervision, particularly in the pre-hospital context where a patient's condition may change during transport, as described in Prehospital Trauma Life Support 6.
The neurological assessment with the GCS is crucial in stage D of the trauma care protocol. Studies by Oliveira 21 indicate challenges in using the GCS, demonstrating low reliability and accuracy of the assessments carried out, emphasizing the need for training and education in this area.
Lanes et al. 22 showed in their review of studies carried out in Europe, Asia and America that the use of ECG is still a difficulty faced by health professionals. It emphasizes the need for training as a way of improving knowledge, and it is important and necessary to expand educational actions and professional training on the subject. In comparison, this study showed that the participants had difficulties with the subject of ECG and that, even after theoretical and practical training and realistic simulation, there was little improvement in their understanding and application of this content, which went from 33 % to 44.4 % of the participants getting it right.
And stage E, which concludes the primary assessment, is the stage in which the victim should be exposed, with the aim of identifying possible injuries not observed in the other stages of the assessment, and then controlling hypothermia by warming the victim with a blanket or thermal blanket. 6
Professionals working in pre-hospital care must be familiar with the protocol for assessing trauma patients and their critical thinking must guide them in providing care, prioritizing the most critical situation. 6 Considering that the trauma victim with exsanguinating hemorrhage a potentially serious victim, the importance of care by a team with more complex skills and appropriate materials and medications for the emergency situation will contribute to the trauma victim’s better survival.
It is therefore important to point out that within the nursing team, nurses trained in emergency care play a fundamental role in the care of trauma victims, through their scientific knowledge, critical thinking, agility in decision-making, timely intervention in times of stress and their work with the multi-professional team to stabilize and maintain life. Procedures such as controlling major external bleeding, maintaining a patent airway, correctly restricting spinal movement and maintaining transport. 23) The care and treatment of critically ill, life-threatening or life-threatening patients who require highly complex intensive care is covered by Article 11 of the Professional Practice Law No. 7,498/86 of June 1986, which is the exclusive activity of nurses. 24
In APH, the team activity, with the doctor, ambulance driver and nurse, has the mission of caring for the victim, at the scene of the accident and throughout the transportation to the final destination. The care may require invasive procedures, highly complex care for resuscitation and stabilization of the victim. In situations of support for the BLS teams, the APH nurse responsible for directing the care provided, according to the characteristics of the incident, and leading teamwork in advanced life support will provide greater safety for the victim. 25
In order to provide the best assistance to victims, it is important that APH professionals actively participate in professional, technical and pedagogical training courses, with realistic simulations, so that they can improve their technical skills in order to provide systematized, organized and prioritized care in urgent and emergency situations.
This highlights the importance of professional training for those who provide urgent and emergency care and trauma on the roads, using active methodologies. Realistic simulation has stood out in health teaching, as it exposes workers to practical experience and critical reflection, as it enables professionals to provide care in a systematized way, where theory and practice complement each other, and professionals can put their protocol-based protagonism into practice in the face of trauma care in a safe environment.
Xavier et al. 26 adds that active methodologies help to show professionals their ability to absorb knowledge and test their agility in practice. It is important and necessary to maintain the periodicity of these training sessions, so that the practice contributes to the proper development of professional skills, strengthens safety in the assessment and care of victims and results in patient safety.
In a comparative study, Mesquita et al. 27 used realistic simulation as a strategy for professional training, demonstrating its relevant role in health activities, as simulation contributes to the development of cognitive and psychomotor skills, through experience in a simulated environment, close to the real thing, thus adding theoretical knowledge to practical knowledge in a practical, stimulating way, in which professionals can learn, identify, recognize, redo and correct possible errors. Thus, both independent simulation and simulation combined with theory are effective, as they develop professionals’ self-confidence, improve their skills and, directly, patient safety.
Thus, Oliveira et al. 16 consider realistic simulation to be an important tool used in continuing education for health professionals, as this strategy is considerably effective in developing theoretical and practical learning, especially with professionals who work in the APH, as it provides the opportunity to apply skills, identify flaws, correct errors and improve knowledge. Araújo et al. 28 also recommend the use of realistic simulation as a teaching strategy, which can be applied to mid-level professionals, with the aim of improving absorption and increasing the level of knowledge of the professionals taking part in this process. Thus, the study can measure the teams’ previous knowledge and provide them with knowledge of the trauma care protocol and the experience of dealing with a trauma situation in a realistic simulation.
The pre-hospital environment requires professionals to be physically, mentally and cognitively prepared, dedicated, conscientious and ethical, and to bear in mind the characteristics of the environment in which they normally work. An ill-prepared professional can contribute to worsening the survival of a victim, but their good conduct and resourcefulness in care, based on protocol, will provide the patient with positive impacts on morbidity and mortality in relation to trauma. Thus, the use of the trauma care protocol will make a significant contribution to first aid at the scene of Advanced Trauma Life Support,12 if associated with the practice of clinical simulation as an in-service training method.
Limitations of the study
The absence of professionals from five municipalities demonstrates the insufficient communication and dissemination of training by service managers to professionals working in pre-hospital care in the municipalities.
The withdrawal of some registered professionals on the day of the training led to the withdrawal of others who depended on transportation to get to the municipality where the training was being held, as well as other situations where the start of the activities was delayed.
Conclusion
The results of this study showed the importance of periodically training the professionals who work in APH and provide trauma care, given the complexity of the cases and the fact that these professionals often provide care in their region due to the lack of other support services close to the occurrences. Faced with “a group” who thought they were poorly trained to deal with traumas, the realistic simulation training developed respected its execution phases and enabled considerable improvement in most of the stages of the trauma care protocol, as this practice gave professionals the opportunity to train their skills in practice and reflect on them.
The survey also pointed out the difficulties faced by VLB professionals in assessing and carrying out two stages of care considered to be highly complex, with the indication of advanced life support assessment and care, in order to better manage cases in these situations.
Contributions to the field of nursing
A study analyzing before and after an educational intervention demonstrated the relevance of active methodologies, as they have been gaining ground as teaching strategies. The realistic simulation used in this research proved to be a recognized teaching-learning tool in nursing education and training for mid-level professionals and professionals who are in the field, directly dealing with real situations and need to be ready to face them on a daily basis. In this way, this study will contribute to improving the skills of professionals working in basic life support teams, as well as professionals working in pre-hospital care, in primary trauma assessment, through realistic simulation as a strategy for improving the knowledge of these professionals.
The methodology used to carry out this research proved to be highly effective in relation to the first evaluation carried out on the professionals, with positive results in the short term when comparing the stages before and after the realistic simulation.
REFERENCES
1. World Health Organization. Global status report on road safety 2018 (Internet). Geneva: World Health Organization; 2018 (acesso em 2023 abr 23). Disponível em: Disponível em: https://www.who.int/publications/i/item/9789241565684 [ Links ]
2. Hospital Israelita Albert Einstein. Panorama do Trauma no Brasil e no mundo (Internet). São Paulo: Hospital Israelita Albert Einstein; 2017 (acesso em 2023 abr 24). Disponível em: Disponível em: https://www.einstein.br/estrutura/nucleo-trauma/o-que-e-trauma/panorama-trauma-brasil [ Links ]
3. Carvalho, IC, Saraiva, IS. Perfil das vítimas de trauma atendidos pelo serviço de atendimento móvel de urgência. Revista Interdisciplinar. 2015;8(1):137-48. [ Links ]
4. França, JR, Costa, LD, Rodrigues Filho, LF, Pereira, NGBG, Soares, N da S. Simulação realística em enfermagem: a experiência discente enquanto vítima de trauma em desafio. Braz. J. Develop. (Internet). 2023 (acesso em 2023 mai 10);9(3):9070-7. Disponível em: Disponível em: https://ojs.brazilianjournals.com.br/ojs/index.php/BRJD/article/view/57725 [ Links ]
5. Farias, DC, Celino, SDM, Peixoto, JBS, Barbosa, ML, Costa, GMC. Acolhimento e Resolubilidade das Urgências na Estratégia Saúde da Família. Rev Bras Educ Med (Internet). 2015 (acesso em 2023 abr 23);39(1):79-87. doi: doi: 10.1590/1981-52712015v39n1e00472014 [ Links ]
6. National Association of Emergency Medical Technicians. PHTLS - Atendimento pré-hospitalar ao traumatizado. 9ª ed. Burlington: Jones & Bartlett Learning; 2020. [ Links ]
7. Araújo, MS, Medeiros, SM, Costa, EO, Oliveira, JSA, Costa, RRO, Sousa, YG. Analysis of the guiding rules of the nurse technician’s practice in Brazil. Rev Bras Enferm (Internet). 2020 (acesso em 2023 abr 23);73(3):e20180322. doi: doi: 10.1590/0034-7167-2018-0322 [ Links ]
8. Ribeiro, VS, Garbucio, DC, Zamariolli, CM, Eduardo, AH, Carvalho, EC. Simulação clínica e treinamento para as práticas avançadas de enfermagem: revisão interativa. Acta Paul Enferm. 2018;31(6):659-66. doi: 10.1590/1982-0194201800090 [ Links ]
9. Costa, RRO, Medeiros, SM, Coutinho, VRD, Mazzo, A, Araújo, MS. Satisfaction and self-confidence in the learning of nursing students: randomized clinical trial. Esc Anna Nery (Internet). 2020 (acesso em 2023 abr 23);24(1):e20190094. doi: doi: 10.1590/2177-9465-EAN-2019-0094 [ Links ]
10. Schulz, KF, Altman, DG, Moher, D. CONSORT 2010 Statement: updated guidelines for reporting parallel group randomised trials (Internet). 2010 (acesso em 2023 abr 24). Disponível em: https://www.equator-network.org/reporting-guidelines/consort/ [ Links ]
11. Jeffries, PR (Ed.). The NLN Jeffries simulation theory. Wolters Kluwer. New York: National League for Nursing; 2016. [ Links ]
12. American College of Surgions Committee on Trauma. ATLS - Advanced Trauma Life Support. 9ª ed. Chicago: Amercian College of Surgeons; 2019. [ Links ]
13. Almeida, CL. Simulação realística: estratégia de ensino- aprendizagem no atendimento ao trauma (Tese de doutorado). Londrina: Universidade Estadual de Londrina, Centro de Ciências da Saúde, Programa de Pós-Graduação em Enfermagem; 2022. [ Links ]
14. Pasquali, L. Princípios de elaboração de escalas psicológicas. Rev Psiquiatr Clin. 1998 (acesso em 2023 abr 23);25(5):206-13. Disponível em: Disponível em: http://ppget.ifam.edu.br/wp-content/uploads/2017/12/Principios-de-elaboracao-de-escalas-psicologicas.pdf [ Links ]
15. Rudolph, JW, Simon, R, Dufresne, RL, Raemer, DB. There’s no such thing as “nonjudgmental” debriefing: a theory and method for debriefing with good judgment. Simulation Healthcare. 2006 (acesso em 2023 abr 23);18(1):49-55. Available from: Available from: https://simulation.med.ufl.edu/wordpress/files/2020/10/Theres-no-such-thing-as-a-nonjudgemental-debriefing.pdf [ Links ]
16. Oliveira, TMN, Moreira, ACMG, Martins, EAP. A simulação da reanimação cardiopulmonar e o conhecimento de socorristas: Estudo quase-experimental. Rev Min Enferm (Internet). 2022 (acesso em 2023 abr 23);26. doi: doi: 10.35699/2316-9389.2022.39427 [ Links ]
17. Machado, MH (Coord.). Perfil da Enfermagem no Brasil: relatório final (Internet). Rio de Janeiro: NERHUS - DAPS - ENSP/Fiocruz; 2017 (acesso em 2023 abr 24). Disponível em: Disponível em: http://www.cofen.gov.br/perfilenfermagem/pdfs/relatoriofinal.pdf [ Links ]
18. Ministério da Infraestrutura (BR). Registro Nacional de Condutores Habilitados no Brasil (Internet). Brasília: Ministério da Infraestrutura; 2023 (acesso em 2023 abr 24). Disponível em: Disponível em: https://www.gov.br/infraestrutura/pt-br/assuntos/transito/conteudo-Senatran/estatisticas-quantidade-de-habilitados-denatran [ Links ]
19. Ministério da Saúde (BR). Protocolos de Intervenção para o SAMU 192 - Serviço de Atendimento Móvel de Urgência (Internet). Brasília: Ministério da Saúde; 2016 (acesso em 2023 abr 24). Disponível em: Disponível em: https://bvsms.saude.gov.br/bvs/publicacoes/protocolo_suporte_basico_vida.pdf [ Links ]
20. Santos, ISN, Souza, CJ, Silvino, ZR. A simulação realística como ferramenta gerenciadora do cuidado no controle de hemorragias no trauma. Conjucturas (Internet). 2022 (acesso em 2023 abr 23);22(11):792-805. doi: doi: 10.53660/CONJ-1453-2A05 [ Links ]
21. Oliveira, MR, Anaisse, SLST, Silva, MA, Silva, AF, Barboza, EE, Santos Neto, AT, et al. Aplicação da escala de coma de glasgow em urgência e emergência nos cuidados de enfermagem. International Journal of Development Research (Internet). 2021 (acesso em 2023 abr 23);11(9):50208-11. doi: doi: 10.37118/ijdr.22884.09.2021 [ Links ]
22. Lanes, TC, Carneiro, AS, Bernardi, CMS, Villagran, CA. Avaliação neurológica a partir da Escala de Coma de Glasgow em vítimas de traumatismo cranioencefálico. Braz. J. Hea. Rev. (Internet). 2021 (acesso em 2023 mai 10);4(5):23591-602. Disponível em: Disponível em: https://ojs.brazilianjournals.com.br/ojs/index.php/BJHR/article/view/38767 [ Links ]
23. de Carvalho, AK de A, Figueira, MC e S, da Costa, LSL, da Macena, MC, Lima, M de F, dos Santos, JGS, Ribeiro, KAA. O enfermeiro no atendimento pre- hosptalar movel em vítimas de trauma: uma revisão integrativa. Braz. J. Develop. (Internet). 2023 (acesso em 2023 mai 10);9(4):13550-66. Disponível em: Disponível em: https://ojs.brazilianjournals.com.br/ojs/index.php/BRJD/article/view/58889 [ Links ]
24. Dispõe sobre a regulamentação do exercício da Enfermagem e dá outras providências. Lei no 7.498/1986, 25 de junho. Diário Oficial da União (Internet). 1986 (acesso em 2023 abr 24). Disponível em: Disponível em: http://www.planalto.gov.br/ccivil_03/leis/l7498.htm [ Links ]
25. Luna, HM, Silva, JA, Aoyama, EA. O Papel Do Enfermeiro No Atendimento Pré-Hospitalar Móvel. Rev Bras Interdiscip Saúde (Internet). 2022 (acesso em 2023 abr 23);4(4):80-7. Disponível em: Disponível em: https://revistarebis.rebis.com.br/index.php/rebis/article/view/452 [ Links ]
26. Xavier, ACA, Santos, AT, Santos, KA, Luz, RE, Sanches, GJC. Metodologias ativas na disciplina de urgência e emergência: contribuição para formação do enfermeiro a partir de uma análise bibliográfica. Rev Saúde.Com (Internet). 2021 (acesso em 2023 abr 23);17(1). doi: 10.22481/rsc.v17i1.5392 [ Links ]
27. Mesquita, HCT, Santana, BS, Magro, MCS. Efeito da simulação realística combinada à teoria na autoconfiança e satisfação de profissionais de enfermagem. Esc Anna Nery (Internet). 2019 (acesso em 2023 abr 23);23(1):e20180270. doi: doi: 10.1590/2177-9465-EAN-2018-0270 [ Links ]
28. Araújo, MS, Medeiros, SM, Costa, RRO, Coutinho, VRD, Mazzo, A, Sousa, YG. Efeito da simulação clínica na retenção do conhecimento de estudantes de enfermagem. Acta Paul Enferm (Internet). 2021 (acesso em 2023 abr 23);34:eAPE000955. doi: doi: 10.37689/acta-ape/2021AO000955 [ Links ]
How to cite: Rocco KMW de, Pereira MGN, Almeida CL de, Haddad MDC, Martins EADP. Realistic simulation as a training strategy for the health team. Enfermería: Cuidados Humanizados. 2023;12(2):e3329. doi: 10.22235/ech.v12i2.3329
Authors’ participation: a) Conception and design of the work; b) Data acquisition; c) Analysis and interpretation of data; d) Writing of the manuscript; e) Critical review of the manuscript. K. M. W. D. R. has contributed in a, b, c, d; M. G. N. P. in b, d, e; C. L. D. A. in a, e; M. D. C. H. in e; E. A. D. P. M. in a, d, e.
Received: April 26, 2023; Accepted: September 03, 2023
 Este é um artigo publicado em acesso aberto sob uma licença Creative Commons
Este é um artigo publicado em acesso aberto sob uma licença Creative Commons
