










Serviços Personalizados
Journal

Artigo
 texto em
texto em  Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
Links relacionados
Compartilhar

 Permalink
PermalinkEnfermería: Cuidados Humanizados
versão impressa ISSN 1688-8375versão On-line ISSN 2393-6606
Enfermería (Montevideo) vol.11 no.1 Montevideo jun. 2022 Epub 01-Jun-2022
https://doi.org/10.22235/ech.v11i1.2712
Original Articles
Pain Evaluation and Registration in an Emergency Department: A Cross-sectional Study

1 Centro Hospitalar de Setúbal, Portugal
2 Instituto Politécnico de Setúbal, Escola Superior de Saúde, Portugal
3 Centro Hospitalar de Setúbal, Portugal, tania_carmo@hotmail.com
Introduction:
Pain is the main reason for seeking healthcare in an emergency service. Nurses have a crucial role in promoting and intervening in pain control as they are professionals with a privileged relationship with people.
Objective:
Describe how the nursing team assessed and recorded pain in the minor’s area of an Accident and Emergency service.
Methodology:
Quantitative, descriptive, and cross-sectional study. The pain assessment records of 105 people were analyzed. Data analysis was conducted using descriptive statistics.
Results:
Pain was assessed in 53 episodes (50.48 %). The Numerical Rating Scale was the most used instrument (43.81 %). The characteristics of pain were described in 39.05 % of the episodes. In 1.90 % of the attacks, there was a record of pain reassessment after implementing pharmacological measures.
Conclusion:
Pain assessment was underreported in the different dimensions described in the study. Thus, it is essential to define strategies for the education and training of nurses on pain assessment.
Keywords: pain assessment; electronic health records; nursing; hospital emergency service
Introdução:
A dor constitui-se como o principal motivo de procura de cuidados de saúde no serviço de urgência. Os enfermeiros têm um papel essencial na promoção e intervenção no controlo da dor dado serem profissionais com uma relação privilegiada com as pessoas.
Objetivo:
Descrever como foi avaliada e registada a dor na área de ambulatório de um serviço de urgência geral pela equipa de enfermagem.
Metodologia:
Estudo quantitativo, descritivo e transversal. Foram analisados os registos de avaliação da dor de 105 pessoas. Procedeu-se à análise dos dados utilizando estatística descritiva.
Resultados:
A dor foi avaliada em 53 episódios (50,48 %). A Escala de Avaliação Numérica foi o instrumento mais utilizado (43,81 %). As características da dor foram descritas em 39,05 % dos episódios. Em 1,90 % dos episódios houve registo de reavaliação da dor após implementação de medidas farmacológicas.
Conclusão:
A avaliação da dor foi subnotificada nas diferentes dimensões descritas no estudo. Neste sentido, torna-se essencial a definição de estratégias para a formação e treino dos enfermeiros sobre avaliação da dor.
Palavras-chave: medição da dor; registos eletrónicos de saúde; enfermagem; serviço hospitalar de emergência.
Introducción:
El dolor es el principal motivo de búsqueda de atención sanitaria en un servicio de urgencias. Las enfermeras tienen un papel crucial en la promoción e intervención en el control del dolor, ya que son profesionales con una relación privilegiada con las personas.
Objetivo:
Describir cómo el equipo de enfermería valoró y registró el dolor en el área de menores de un servicio de Urgencias.
Metodología:
Estudio cuantitativo, descriptivo y transversal. Se analizaron los registros de valoración del dolor de 105 personas. El análisis de los datos se realizó mediante estadística descriptiva.
Resultados:
El dolor fue evaluado en 53 episodios (50,48 %). La Escala Numérica fue el instrumento más utilizado (43,81 %). Las características del dolor se describieron en el 39,05 % de los episodios. En el 1,90 % de las crisis se registró una reevaluación del dolor tras la aplicación de medidas farmacológicas.
Conclusiones:
La evaluación del dolor fue subestimada en las dimensiones presentadas en el estudio. Por ello, es imprescindible definir estrategias para la educación y formación de las enfermeras en la valoración del dolor.
Palabras clave: evaluación del dolor; historias clínicas electrónicas; enfermería; servicio de urgencias hospitalarias
Introduction
Considering the International Association for the Study of Pain (IASP), the NANDA-I Nursing Diagnoses taxonomy defines pain as an “unpleasant sensory and emotional experience associated with actual or potential tissue damage or described in terms of such damage”. This taxonomy difference acute pain, a sudden or slow onset of pain, variable intensity and expected end, from chronic pain, similar to acute pain in its beginning and intensity, but continuous or recurrent, lasting more than three months and without prevision of your end.1
Pain is a physiological condition with high importance for a person’s physical integrity. In addition to the suffering and reduced quality of life it causes, it causes pathophysiological changes that contribute to the emergence of organic and psychological comorbidities and can perpetuate pain. In addition to the suffering and reduced quality of life, it causes pathophysiological changes that contribute to the appearance of organic and psychological comorbidities and can perpetuate the painful phenomenon. Pain also significantly impacts family members and/or caregivers and represents a loss that is difficult to quantify for society in general. According to the European Federation of IASP Chapters, the pain socio-economic consequences have been equated with those caused by cardiovascular disease or cancer.2
The scientific community has shown a growing interest in this area, which has allowed an evolution in pain prevention and treatment, which inevitably poses challenges to care provision. In this sense, it is essential to define education, training, and teaching strategies for all stakeholders to develop good practices in the various contexts of professional intervention. The responsibility for acquiring and updating pain knowledge must be shared by educational institutions, care providers, and nurses.3
Pain is the main reason for seeking health care in the emergency department, being a reality that nurses constantly have to deal with. In providing care, pain must be systematically evaluated and recorded to allow early and individualized intervention to promote well-being, continuity, and quality of care.4 Effective pain control is not only a duty of health professionals but also a right of people who suffer from it and a crucial step towards the effective humanization of health institutions.5
The Ordem dos Enfermeiros (OE) increase the importance of nurses in promoting and intervening in pain control, as they are professionals with a privileged relationship with people due to their proximity and time of contact with them. Particularly the Nurse Specialists in Nursing in Persons in Critical Situations must carry out the “differentiated management of pain and well-being of the person in a critical situation and/or organ failure, optimizing the answers”.6
The process of regular pain monitoring should start at the time of triage, and it must be continued throughout the length of stay in the emergency department. According to Grupo Português de Triagem, “pain assessment in an emergency context is a process that requires expertise and training, with special restrictions in this environment, which reflect the nature of the urgency of the person’s health situation and the lack of time for assessment”.7
According to the recommendations of the Grupo de Avaliação da Dor da Sociedade Portuguesa de Cuidados Intensivos (SPCI) / Pain Assessment Group of the Portuguese Society of Intensive Care, which meets the definition of the institution’s Clinical Guidance Standard, pain assessment should be carried out in all shifts and whenever necessary; at the beginning of a shift; 5-10 minutes before starting a painful procedure; during a painful practice; 15 minutes after the painful practice; and 30 minutes after the implementation of pharmacological and/or nonpharmacological measures.8
Pain assessment encompasses physical examination; l characteristics (location, quality, intensity, duration, frequency); ways of communicating pain/expressions of pain; relief and aggravating factors; coping strategies; associated symptoms; description of the use and effect of pharmacological and nonpharmacological measures; knowledge/understanding about the disease; implications of pain on life activities; and emotional, socio-economic, and spiritual impact of pain.3
Pain assessment instruments include the Numerical Pain Rating Scale and the Faces Pain Scale. The Numerical Pain Rating Scale consists of a ruler divided into eleven equal parts, numbered from 0 to 10, where 0 corresponds to the classification “No Pain” and 10 to “Maximum Pain”. In the Faces Pain Scale, the person is asked to rate the intensity of their pain based on the mimicry presented in each drawn face, with the expression of happiness corresponding to the classification “No Pain” and the expression of maximum sadness corresponding to the score “Pain maximum”.5
The choice between the different assessment instruments must consider: the type of pain; age; clinical situation; interpretation criteria; psychometric properties, comparable quantification scale, ease of application, and user experience.3
Records should be an integral element of the entire pain assessment process and monitoring and practice of nurses to ensure continuity of care. The relevance of health care records has been the subject of ongoing debate. From Nightingale to the current International Classification for Nursing Practice, records have become indispensable and essential and are based on a legal basis.4
Nurses recognize the importance of documentation for continuity of care. However, in clinical practice, it is observed that this is sometimes neglected since records are scarce and incomplete when performed.4
According to the Professional Nursing Deontology (item d) of article 104 “On the right to care”, the Nurse must “ensure the continuity of care, accurately recording the observations and interventions carried out.”9) The importance of records is increased too in the Nursing Care Quality Standards and in the General Care Nurse Competency Profile Regulation (competence criterion 62), where it is described that the Nurse “consistently communicates relevant, correct and understandable information about the client’s health status, orally, in writing and electronically, respecting their area of competence.”10 In addition to the importance of continuity of care, records are essential to obtain data for quality assessment, epidemiological analysis, and research.3
The present study was guided by the research question: “How is pain evaluated and recorded by the nursing team in the outpatient area of the emergency department?”. As a form of guidance in this process, we defined four sub-questions: “What are the moments of pain assessment?”; “What are the pain assessment scales used?”; “Which pain characteristics are evaluated and recorded?” and “Was there implementation of pharmacological and/or nonpharmacological measures?”.
Objectives
The present article is based on an investigation developed at an emergency department to describe how pain was assessed and recorded in people in the outpatient area by the nursing team. In this sense, we have outlined specific objectives: to identify the moments of pain assessment recorded; identify the pain assessment scales in use; describe the pain characteristics reported in nursing records and verify the implementation of pharmacological and nonpharmacological measures.
Methodology
A study was carried out with a quantitative, transversal, simple descriptive approach. Participants were selected using a non-probabilistic convenience sampling technique. Considering that this study presents the partial results of an investigation that includes the pain evaluation and recording in an outpatient clinic and at the emergency department, people aged 18 years and over who have stayed for some time were considered inclusion criteria. Equal to or greater than 8 hours in hospital between January 15, 2019, and January 31, 2019. All people who stayed less than 8 hours were excluded. The results presented in this article refer to the pain assessment and recording of people during their stay in the outpatient clinic.
This study received a favorable opinion from the Ethics Committee for Health and the Board of Directors of the respective Hospital Center on 4/23/2019 - Minutes No. 16/19. The ethical aspects inherent to a research path were considered.
The co-investigators carried out data collection, and the principal investigator assumed responsibility for their treatment, ensuring data security, fidelity and scientific integrity.
A ten items tool was created, in a table format, for the documentary analysis of the data extracted from the ALERT® computer platform, which included the collection of variables for the characterization of the sample (gender, age, length of stay in the clinic, flowchart and discriminator in triage) and the pain assessment and recording (records of pain intensity and characteristics, pain scale and pharmacological and nonpharmacological measures implemented) during the person’s stay in the outpatient area. The effectiveness and validity of this tool were confirmed with a pre-test application of 10 episodes that met the inclusion criteria. The instrument was calibrated, and it was unnecessary to make any changes.
The statistical treatment of the data related to the 105 episodes of Emergency was carried out after recoding the nominal variables into numerical ones, using descriptive statistics, using the Microsoft Excel® program.
Results
Regarding the characterization of the sample (Table 1), we can say that 56.19 % of the people were female, the average age was 78 years old, with a standard deviation of 12.66 years, and the length of stay in the outpatient area, it averaged 21 hours, with a mode of 16 hours.
The most used flowchart at the time of the Manchester Triage was “dyspnea”, with 39.0 5%. In 7.62 % of the episodes, people were screened by the pain flowchart - chest pain, abdominal pain and headache. The discriminator “pain” was chosen in 16.19 % of the episodes, with “moderate pain” being the most selected with 14.29 %.
Table 1: Sample characterization
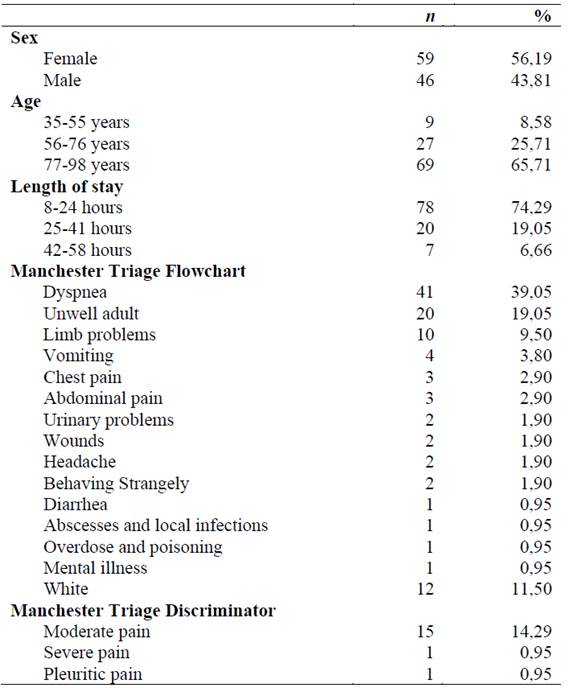
Source: Data taken from the ALERT® IT platform. Own elaboration (2019).
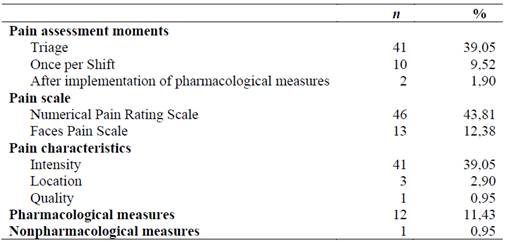
Data related to pain assessment and recording are presented in Table 2.
26.66 % of people reported mild pain, 3.80 % moderate pain, and 0.95 % severe pain at the screening time. The pain was recorded at the time of screening in 39.05 % of episodes, and 31.43 % of the cases, people expressed pain and in 7.62 % of the cases, they denied its existence. Of the remaining 60.95 % of the episodes in which pain was not recorded, 11.43 % referred to people screened by the white flowchart, in which, by definition, it is not possible to record pain assessment in the complaint.
On pain assessment records at least once per shift, recommended by the SPCI, we found that this guideline has complied with 9.52 % of the episodes.
The pain reassessment recorded after implementing pharmacological measures was performed in 1.90 %, and in one of them, the reassessment was performed and recorded two different times.
Pain records in the “vital signs” field were performed in 41.90 % of the episodes, with 39.05 % corresponding to the assessment conducted at triage and 2.86 % during the person’s stay in the outpatient area. The pain assessment records in the “nursing notes” field were performed in 22.86 % of the cases, of which 14.29 % of the people had not expressed pain in the triage. It should be noted that in one of the episodes, the pain was recorded at three different times.
The most used pain assessment scale was the Numerical Pain Rating Scale (43.81 %).
Regarding the adequacy of the scale used, taking into account the clinical situation of each person, we considered that in 37.14 %, the scale used was adequate to the situation and that in 13.33 %, there was no adequacy of the scale.
Pain intensity was the most registered characteristic (39.05 %). The remaining features evaluated referred to the location (chest pain, pain in the left hemithorax) and quality of pain (pricking type). A record (0.95 %) was also identified concerning an aggravating factor (worsening on inspiration).
The record of nonpharmacological measures implementation was performed in 0.95% of the episodes (no reassessment record). In 11.43 %, the performance of the pharmacological actions was recorded, namely in 8.58 % of the people who reported pain at the time of screening and in 2.86 % who mentioned pain during the outpatient stay.
Discussion
Pain is the main reason people use emergency services, and, in general, 25-29 % of the population suffers from pain.11 The number of people with pain who use emergency services has been increasing, making their assessment essential, namely through the use of pain assessment tools and the training of professionals in this area.11 Lima et al.11) and Mota et al.12) confirmed that in Portugal, acute pain was the main reason for hospital admission, reporting that more than 70 % of people had pain as the main symptom.
In the present study, in 7.62 % of the episodes, people were screened by flowcharts related to pain, and in 16.19 %, the discriminator “pain” was selected.
We infer this difference in results from two perspectives: devaluation of pain assessment or underreporting its registration. Several authors mentioned the devaluation of pain by professionals.12,13,14) The underreporting of pain records was evidenced by Gimenes et al.15, who mentioned a disparity between the records made and the pain reports collected from people. In their study, 33.3 % of people who experienced acute pain had no assessment recorded. These findings undermine the quality and safety of care.15 For Gimenes et al.15 and Stalnikowicz et al.16, the lack of records may be related to the insufficient knowledge of nurses regarding pain assessment and management.
For effective pain management, continuous and regular assessment by health professionals is essential.5 The Nursing Interventions Classification (NIC) defines the “pain control” intervention as the relief of pain or its reduction to a comfort level accepted by the person. The NIC also lists a list of activities to be developed within this intervention that, considering the study’s objectives, we would like to highlight, among others: the observation of the person; complete pain assessment; the implementation, evaluation and teaching of pharmacological and nonpharmacological interventions.17 “Pain control” also emerges in the results suggested in the classification of nursing outcomes (NOC).18
Pain assessment should consider emotional and psychosocial issues that may exacerbate the person’s complaints11 to optimize therapy to promote and improve quality of life.5 Mota et al.12 emphasized the importance of mandatory pain assessment and recording to ensure proper management. Some factors influence the assessment of pain by health professionals: lack of empathy, work overload, and difficulty understanding and applying the pain assessment scale.11
In the present investigation, the pain was recorded 50.48 % of the episodes, 39.05 % at triage time, 9.52 % once per shift and 1.90 % after implementing pharmacological measures. In this sense, it becomes possible to perceive a poor record regarding pain assessment, namely regarding the effectiveness of pain control measures implemented, as recommended in the NIC and the NOC results.
Perera et al.19 valued identifying and assessing pain at triage time as fundamental for its treatment. In the present study, the pain was recorded at the time of screening in 39.05 % of the episodes, and in 31.43 % of the episodes, people reported pain, and in 7.62 % of the cases, they did not reveal pain. In this context, making a parallel with the activities described in the NIC, we consider it extremely important to assess the occurrence of non-verbal indicators of discomfort, namely in people unable to communicate their presence orally. It should be noted that the importance of this assessment is not limited to the moment of triage but must be present throughout the person’s stay in the service.
Stalnikowicz et al.16 considered the possibility of nurses administering analgesics at the time of triage using a previously structured protocol. We believe it pertinent to mention that there is an analgesic protocol in the triage in the SUG where this investigation was carried out, making it possible for people to receive analgesia care from the moment they enter the service.
The SPCI Pain Assessment Group8 and the institution’s Clinical Guidelines recommend pain assessment at the beginning of each shift. In the present investigation, pain assessment complied with this recommendation in 9.52 % of episodes.
The application of pain assessment scales, whose objective is to measure, locate and adequately manage the measures to be implemented, is the nurse’s responsibility, and he must be able to apply it.11 The most used assessment scale for recording pain in the emergency department was the Numerical Pain Rating Scale (43.81 %), followed by the Faces Pain Scale (12.38 %). The values found in the study are lower than those reported in the study by Mota et al.12, in which 88.5% of the participants assumed the use of the Numerical Pain Rating Scale and 71.9% the use of the Faces Pain Scale.
According to the OE3 and other authors, the choice of assessment instruments should consider the person’s age, type of pain, clinical situation, psychometric properties, interpretation criteria, ease of application, and experience of use by healthcare professionals.11,12 Considering the person’s clinical situation, we found that the scale used was considered adequate in 37.14 % of the episodes; in 13.33 % of the cases, there was no correct choice of the assessment instrument. Pain assessment scales and their proper use are fundamental tools for nurses to monitor pain and ensure effective treatment.12
The characteristic of pain most recorded in the present study was intensity (39.05 %), an aspect in line with Perera et al.19, who report that nurses value intensity in recording acute pain and, later, location, quality and interventions for pain relief. In the current study, we were able to show a gap in the recording of complete pain assessment, which includes location, characteristics, onset/duration, frequency, quality, intensity and severity, in addition to precipitating factors, as recommended in the NIC activities. Gimenes et al.15 emphasize the lack of knowledge of health professionals is one of the reasons for underreporting and inadequate pain management. Nurses need to assume responsibility for the quality and humanization of care, namely concerning pain relief as a person’s right,15 not underestimating it and intervening in the sense of its early minimization.11
Access to pain management is a fundamental human right referred to by the World Health Organization, Human Rights Watch and the Montreal Declaration.12,19 The Directorate-General for Health2 adds that it is also a health professional’s duty. In this study, the registration of pharmacological measures implemented was performed in 11.43 % of the analyzed emergency episodes. These results agree with the study developed by Stalnikowicz et al.16, who mentions that despite pain being one of the main symptoms in emergency services, about 70% of people with acute pain do not receive any analgesia for pain control. Mota et al.12 also refer to several studies that indicate that 60%-80% of people receive ineffective pain treatment. Inadequate analgesia treatment is mentioned by Perera et al.19 and Mota et al.12. They point out the causes of an approach that undervalues pain assessment in emergency services,12 less adequate guidelines and subtherapeutic dosages.19
According to a study by Perera et al.19, Nonpharmacological measures were used in 4.2 % of the situations and were 100 % effective. In the present investigation, the record of the implementation of these measures was also low (0.95 %). Several nonpharmacological measures are referenced in the literature: massage, comfortable positioning, relaxation techniques, therapeutic touch, guided visualization, care with medical devices, application of heat and cold, application of cryogenic fluids, vibration, biofeedback, transcutaneous electrical nerve stimulation, and hypnosis.12,15,19
In the current study, the records show that pharmacological interventions were favored over nonpharmacological ones. These data are consistent with the study by Gimenes et al.15, who reported that analgesia was privileged in favor of nonpharmacological measures in 36.5 % of the situations.
The research also allowed to identify gaps in the records regarding the implementation of pharmacological and nonpharmacological measures for pain relief to ensure that the person receives proper care, as recommended in the NIC activities and the NOC results. It is also pointed out that, due to the nature of the service, it is difficult to control environmental factors (lighting, noise, temperature) that promote an improvement in the person’s response to pain and the promotion of adequate rest to relieve it.
In the present study, pain reassessment after implementing pharmacological measures was observed in 1.9 % of episodes. Gimenes et al.15 also report that in 23.8 % of the cases, there was no record of pain or nursing interventions to manage the person’s pain.
Aspects that make pain assessment difficult have been identified in the literature and are related to: work overload, the person’s clinical situation, the devaluation of pain by professionals, the lack of knowledge about the scales and their application, and the use of language technique.12,13,14 The literature also highlights the need for education and training of health professionals for pain assessment and the proper use of pain assessment scales.11,12,13,14,15
Conclusion
This article emerged within the scope of an investigation in an emergency department to describe how pain was evaluated and recorded in people in the outpatient area of the emergency department by the nursing team.
We can conclude that the pain assessment record was underreported. The number of records is lower than expected at the time of pain assessment provided for by the SPCI and the institution’s Clinical Guidance Standard.
We identified some limitations in carrying out the study, namely the number of white flowcharts and the selection of the discriminator at the time of screening.
The identification and implementation of strategies within the scope of continuous education and training of nurses on pain assessment and recording, particularly about assessment moments, the use of pain assessment scales, the characteristics of pain and the implementation of pharmacological and nonpharmacological treatments are essential to optimize pain management in the emergency department. It is also important to mention that it is imperative to make nurses aware of the importance of pain assessment records.
The development of this study made it possible to identify gaps in the assessment and recording of pain that require intervention, thus substantiating the importance of developing a project to continuously improve the quality of nursing care within the scope of pain assessment and control, also contributing to monitoring of the institution’s Clinical Guidance Standard - “Assessment and Monitoring of Pain in Adults”.
REFERENCES
1. Herdman TH, Kamitsuru S. Diagnósticos de Enfermagem da NANDA. Definições e Classificação 2015-2017 (Internet). Artmed; 2015 (cited 2022 Feb 27). Available from: Available from: https://www.biosanas.com.br/uploads/outros/artigos_cientificos/10/df71d2977c3c9eab8c6c511a8692c2ad.pdf [ Links ]
2. Direção-Geral de Saúde. Portal da Direção-Geral da Saúde (Internet). Circular Normativa Nº 11/DSCS/DPCD. Programa Nacional de Controlo da Dor. Lisboa: DGS; 2008 (cited 2020 Mar 10). Available from: Available from: https://www.dgs.pt/ficheiros-de-upload-2/programa-nacional-de-controlo-da-dor-circular-pdf.aspx [ Links ]
3. Ordem dos Enfermeiros. Portal da Ordem dos Enfermeiros (Internet). DOR: Guia Orientador de Boa Prática. Lisboa: OE; 2008 (cited 2020 Mar 10). Available from: Available from: https://www.ordemenfermeiros.pt/arquivo/publicacoes/Documents/cadernosoe-dor.pdf [ Links ]
4. Silva M, Gonçalves RF. Avaliação e registo da dor no serviço de urgência: que realidade? (Dissertação de Mestrado). Coimbra: Escola Superior de Enfermagem de Coimbra; 2017 (cited 2021 Mar 23). Available from: Available from: https://repositorio.esenfc.pt/private/index.php?process=download&id=52974&code=296 [ Links ]
5. Direção-Geral da Saúde. Portal da Direção-Geral da Saúde (Internet). Circular Normativa Nº 09/DGCG. A Dor como 5º sinal vital. Registo sistemático da intensidade da Dor. Lisboa: DGS; 2003 (cited 2020 Mar 10). Available from: Available from: https://www.dgs.pt/directrizes-da-dgs/normas-e-circulares-normativas/circular-normativa-n-9dgcg-de-14062003-pdf.aspx [ Links ]
6. Ordem dos Enfermeiros. Portal da Ordem dos Enfermeiros (Internet). Regulamento das Competências do Enfermeiro Especialista em Pessoa em Situação Crítica. Lisboa: OE; 2010 (cited 2020 Mar 10). Available from: Available from: https://www.ordemenfermeiros.pt/arquivo/legislacao/Documents/LegislacaoOE/RegulamentoCompetenciasPessoaSituacaoCritica_aprovadoAG20Nov2010.pdf . [ Links ]
7. Oliveira F, Macedo AP, Vilaça SP. Barreiras na Monitorização da Dor identificadas pelos Enfermeiros de um Serviço de Urgência (Dissertação de Mestrado). Braga: Escola Superior de Enfermagem da Universidade do Minho; 2019 (cited 2021 Mar 23). Available from: Available from: http://repositorium.sdum.uminho.pt/bitstream/1822/64206/1/Filipe_Andre_Soares_Oliveira.pdf [ Links ]
8. Sociedade Portuguesa de Cuidados Intensivos. Portal da Sociedade Portuguesa de Cuidados Intensivos (Internet). Plano Nacional de Avaliação da Dor: Resultados. Lisboa: SPCI; (s. d.). (cited 2020 Feb 06). Available from: Available from: https://www.spci.pt/media/documentos/15827260875e567bc79f633.pdf [ Links ]
9. Ordem dos Enfermeiros. Portal da Ordem dos Enfermeiros (Internet). Deontologia Profissional de Enfermagem. Lisboa: OE; 2015 (cited 2020 Mar 10). Available from: Available from: https://www.ordemenfermeiros.pt/media/8887/livrocj_deontologia_2015_web.pdf [ Links ]
10. Ordem dos Enfermeiros. Portal da Ordem dos Enfermeiros (Internet). Regulamento do Perfil de Competências do Enfermeiro de Cuidados Gerais; 2012 (cited 2020 Mar 10). Available from: Available from: https://www.ordemenfermeiros.pt/media/8910/divulgar-regulamento-do-perfil_vf.pdf [ Links ]
11. Lima V, Lohmann P, Costa A, Marchse C. O uso da escala da dor pelos profissionais de enfermagem no contexto da urgência e emergência: uma revisão integrativa. Research, Society and Development. 2020 (cited 2021 Mar 05);9(11). DOI: 10.33448/rsd-v9i11.9403. [ Links ]
12. Mota M, Cunha M, Santos MR, Duarte J, Rocha AR, Rodrigues A et al. Gestão da dor na prática de enfermagem no serviço de urgência. Millenium. 2020 (cited 2021 Mar 06);2(5):269-279. DOI: 10.29352/mill0205e.29.00257 [ Links ]
13. Pinheiro A, Marques R. Behavioral Pain Scale e Critical-Care Pain Observation Tool para avaliação da dor em pacientes graves intubados orotraquealmente. Revisão sistemática da literatura. Rev Bras Ter Intensiva. 2019 (cited 2021 Mar 13);31(4):571-581. DOI: 10.5935/0103-507X.20190070. [ Links ]
14. Valério AF, Fernandes KS, Miranda G, Terra FS. Difficulties faced by nurses to use pain as the fifth vital sign and the mechanisms/actions adopted: an integrative review. BrJP. São Paulo. 2019 jan-mar (cited 2021 Mar 13);2(1):67-71. DOI 10.5935/2595-0118.20190013 [ Links ]
15. Gimenes A, Lopes C, Rodrigues-Neto A, Salvetti M. O registro da dor aguda em pacientes hospitalizados. BrJP. São Paulo. 2020 jul-set (cited 2021 Mar 09);3(3):245-8. DOI: 10.5935/2595-0118.20200178. [ Links ]
16. Stalnikowicz R, Mahamid R, Kaspi S, Brezis M. Undertreatment of acute pain in the emergency department: a challenge. Int J Qual Health Care (Internet). 2005 (cited 2021 Mar 10);17(2):173-6. DOI: 10.1093/intqhc/mzi022. [ Links ]
17. Bulechek GM, Butcher HK, Dochterman JM. 5ª ed. NIC Classificação das intervenções de Enfermagem. Rio de Janeiro: Elsevier Editora Ltda; 2010. [ Links ]
18. Garbin LM, Rodrigues CC, Rossi LA, Carvalho EC. Classificação de resultados de Enfermagem (NOC): identificação da produção científica relacionada. Rev Gaúcha Enfer., Porto Alegre (Internet). 2009 (cited 2022 Mar 01);30(3):508-15. [ Links ]
19. Perera J, López F, Candelas R, Chacón R, Morizot G. Prevalence and Therapeutic Approach of Acute Pain in Emergency Provided by Triage Nursing. Aquichan. 2019 (cited 2021 Mar 12);19(4). DOI: 10.5294/aqui.2019.19.4.4. [ Links ]
How to cite: Figueira AIR, Amaral GMMDS, Carmo TIGD. Pain Evaluation and Registration in an Emergency Department: A Cross-sectional Study. Enfermería: Cuidados Humanizados. 2022;11(1), e2712. DOI: 10.22235/ech.v11i1.2712
Contribution of the authors: a) Study conception and design, b) Data acquisition, c) Data analysis and interpretation, d) Writing of the manuscript, e) Critical review of the manuscript. A. I. R. F. has contributed in a, b, c, d, e; G. M. M. D. S. in a, b, c, d, e; T. I. G. D. C. in a, b, c, d, e.
Received: October 16, 2021; Accepted: May 10, 2022
 Este é um artigo publicado em acesso aberto sob uma licença Creative Commons
Este é um artigo publicado em acesso aberto sob uma licença Creative Commons
