










Servicios Personalizados
Revista

Articulo
 texto en
texto en  Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Curriculum ScienTI
Curriculum ScienTILinks relacionados
Compartir

 Permalink
PermalinkEnfermería: Cuidados Humanizados
versión impresa ISSN 1688-8375versión On-line ISSN 2393-6606
Enfermería (Montevideo) vol.10 no.2 Montevideo 2021 Epub 01-Dic-2021
https://doi.org/10.22235/ech.v10i2.2346
Original Articles
User Difficulties for the Problem-Solving Ability of Ophthalmological Care in the Health Care Network

1 Universidade Estadual Paulista “Júlio de Mesquita Filho”, Brasil, s.meneguin@unesp.br
2 Universidade Estadual Paulista “Júlio de Mesquita Filho”, Brasil
3 Universidade Estadual Paulista “Júlio de Mesquita Filho”, Brasil
Contextual framework:
The problem-solving ability of healthcare is a concept associated with the final resolution of the problems the users bring to the health service.
Objective:
Know the motives that hamper the problem-solving ability of ophthalmological care in secondary healthcare from the user’s perspective and to identify suggestions to improve it.
Methods:
A qualitative-quantitative research was undertaken in a non-probabilistic sample of 208 patients, who were referred for ophthalmological care at a secondary health service in a city in the interior of São Paulo, Brazil. The interviews were recorded with the participants’ consent, transcribed, and analyzed, using the methodological strategy of the Collective Subject Discourse.
Results:
Countless motives delay the problem-solving ability of care, which are linked to bureaucracy, lack of human and material resources and the non-existence of referral and counter-referral in the organization of the healthcare network.
Conclusion:
The difficulties the users feel reflect this service’s lack of organization, which not only does not grant priority to care for the diabetic patients but does not commit either to proper forwarding or monitoring.
Keywords: unified health system; secondary health care; eye health services; nursing.
Marco contextual:
A resolubilidade da assistência à saúde é um conceito associado à resolução final dos problemas trazidos pelos usuários ao serviço de saúde.
Objetivo:
Conhecer os motivos que dificultam a resolubilidade do cuidado oftalmológico na atenção secundária de atenção à saúde, sob a perspectiva do usuário e identificar sugestões de melhoria para a mesma.
Métodos:
Trata-se de uma pesquisa quali-quantitativa, realizada com uma amostra não probabilística de 208 pacientes, que receberam indicação de cuidado oftalmológico em unidade de atenção secundária de saúde, de município do interior de São Paulo. As entrevistas foram gravadas, após consentimento dos participantes, transcritas e analisadas utilizando-se a estratégia metodológica do Discurso do Sujeito Coletivo.
Resultados:
Os motivos que atrasam a resolubilidade do cuidado são inúmeros e estão atrelados à burocracia, falta de recursos humanos e materiais, bem como inexistência da referência e contrarreferência na organização da rede de atenção à saúde.
Conclusão:
As dificuldades sentidas pelos usuários refletem a falta de organização desse serviço, que além de não priorizar o atendimento aos pacientes diabéticos. também não se compromete com o devido encaminhamento e acompanhamento.
Palavras-chave: sistema único de saúde; atenção secundária à saúde; serviços de saúde ocular; enfermagem.
Marco contextual:
La capacidad de la atención de salud para resolver problemas es un concepto asociado a la resolución final de los problemas que los usuarios presentan al servicio de salud.
Objetivo:
Conocer los motivos que dificultan la capacidad del cuidado oftalmológico para resolver problemas en la atención secundaria de salud bajo la perspectiva del usuario, e identificar sugestiones para mejorarla.
Métodos:
Se trata de una investigación cualitativa-cuantitativa, desarrollada con una muestra no probabilística de 208 pacientes, a quienes fue indicado cuidado oftalmológico en una unidad de atención secundaria del interior de São Paulo. Las entrevistas fueron grabadas, tras el consentimiento de los participantes, transcritas y analizadas mediante la estrategia metodológica del Discurso del Sujeto Colectivo.
Resultados:
Los motivos que atrasan la capacidad de resolución de problemas del cuidado son innúmeros y están vinculados a la burocracia, falta de recursos humanos y materiales, además de la inexistencia de referencia y contra referencia en la organización de la red de atención.
Conclusión:
Las dificultades sentidas por los usuarios reflejan la falta de organización de ese servicio, que no solo no prioriza la atención a los pacientes diabéticos, pero tampoco se compromete con el encaminamiento y seguimiento necesario.
Palabras clave: sistema único de salud; atención secundaria de salud; servicios de salud ocular; enfermería.
Introduction
The problem-solving ability of health care is a fundamental concept, being associated with the final resolution of the problems users bring to the service and their satisfaction. 1) Thus, the problem-solving ability is considered a satisfactory response that the service provides to the user when seeking care for some health need. It is not limited exclusively to the cure of diseases, but also covers the relief of suffering, health promotion and maintenance. 1
In this scenario, in which chronic non-communicable diseases (NCDs) are the main cause of mortality in Brazil and an important public health problem, 2) nursing is responsible for meeting the health needs of the population. 3
Among these, it is estimated that, in 2017, Diabetes Mellitus (DM) affected approximately 12.5 million Brazilians 4 and ranked the country fourth among the ten countries with the highest number of cases of the disease, 5 and whose late complications can lead to sight loss. 3
According to the World Health Organization (WHO), globally, at least 2.2 billion people in the world live with visual impairment or blindness, and one billion have a visual impairment that could have been prevented or resolved. 6 In Brazil, in 2018, the estimate was 28 thousand blind Brazilians aged between 0 and 15 years; 169 thousand between 15 and 49 years and 66.3 thousand over 50 years of age. There are countless causes of visual impairment, linked to region, socioeconomic group, gender, age, diabetes, among others. 7
A wide variety of health promotion, disease prevention and treatment strategies have been offered to meet the needs associated with eye diseases throughout life. 6 In this context, health care at the different levels aims to provide individual and/or collective care with emphasis on comprehensiveness and the problem-solving ability of care. 8
In the past ten years, the National Eye Care Policy, which was set up by the Brazilian Federal Health Department, has established not only the actions and strategies for the prevention and promotion of visual health at the three levels of health care, but it has also shown the need to promote comprehensive eye care to the users of the Unified Health System (SUS), including the design of a care area that crosses all levels of care, in order to ensure the integrality of health care. 9,10
Nevertheless, the existence of ordinances and covenants in health policies does not necessarily guarantee the existence of universal and integral access to individuals with ophthalmological demands, especially those with DM, being more susceptible to eye diseases, such as diabetic retinopathy and macular edema. 11
Thus, in view of the magnitude of the ophthalmological care performed at a Secondary Health Care Service, it is considered that one of the most important tasks of nursing is its participation in the organization of health care, planned so that health services are able to respond to the demands of the population. 9 In this context, nursing plays a comprehensive role, with an active participation in care, service management and the autonomous practice of the profession. (13, 14)
Despite the relevance of the topic, in the literature, there is a lack of studies that evaluate the problem-solving ability of ophthalmic care in secondary health care services. Recent research has focused on eye health actions in schools. 15
In view of the above, the proposal of the study was to answer the following guiding questions: Is the care ophthalmologists propose in secondary health care service able to solve the users' problems? What are the difficulties users face to put this care in practice? How can this care be improved?
By considering the complexity of this topic, we intend, from the users' viewpoint, to grant visibility to poorly addressed or veiled issues, and thus contribute to the reorganization of this service.
In view of the above, this study aimed to know the reasons that hinder the problem-solving ability of ophthalmic care in secondary health care from the users' perspective, as well as to identify suggestions to improve it.
Methods
This qualitative-quantitative study was performed with patients attended at the Integrated Health Center in an inland city in the State of São Paulo, Brazil, between April and December 2016.
All patients to whom ophthalmological treatment was indicated in the period from November 2013 to November 2015 were selected from a database and service records. We excluded patients who could not be contacted by telephone to formally extend the invitation due to a change of address or telephone, patients who had died, who were repeated in the database due to repeated consults, as well as patients who did not show up for the procedure.
Of the 241 patients to whom ophthalmological treatment was indicated in the period selected for the study, four missed the scheduled procedure, seven died and 22 could not be contacted by telephone, totaling 208 participants from a non-probabilistic sample. Initially, the participants were contacted by telephone, inviting them to participate in the research and, after their agreement, and interview was scheduled at the Integrated Health Center. A semi-structured script was used for the interviews, consisting of two parts, the first to collect the participants' sociodemographic characteristics and the second composed of two questions namely: "in your opinion, did you face difficulties to get the proposed ophthalmological care? If so, which?"; "In your perception, what do you suggest to improve the practice of the proposed ophthalmological care?”
The interviews were conducted at a single moment, individually, to guarantee the participant's privacy, in a private room at this service. The audio was fully recorded on the researcher's audio recorder, who took care not to influence the interviewee's response in any way. Recordings were destroyed at the end of the study. The average length of the interviews was twenty minutes.
One of the researchers conducted all the interviews, who was a post-graduation student on the occasion. The participants had no personal information about her. The interviewees' testimonies were identified using the letter "P" (interviewee), followed by the number they received in the transcription of the interviews.
The problem-solving ability to put in practice the ophthalmological care proposed by the ophthalmologist of the Integrated Health Center was also considered.
After the interviews, the statements were transcribed and the discourse analysis began, using the methodological strategy of the collective subject discourse (CSD), based on social representations theory. 16
The CSD seeks to respond and know the thoughts, representations, beliefs and values of a group on a given topic, using scientific methods.17
The methodological steps followed from the interviews until the CSD synthesis included: (a) reading of the set of testimonies collected in the interviews; and (b) reading of the answer to each particular question, highlighting the selected key-expressions, and (c) identification of the central ideas of each response; (d) analysis of all key expressions and central ideas, grouping the similarities into homogeneous sets; (e) identification and naming of the central idea, which is a synthesis of the central ideas of each discourse; and (f) construction of the collective subject discourse after the identification of the central ideas and key expressions the collective subject discourses named. 17
To ensure the quality and transparency of the study, the use of the COREQ qualitative research report was adopted. 18
The research started with the approval of the Research Ethics Committee at the Botucatu School of Medicine, under Opinion number 1.227.288-CAAE 48082015.9.0000.5411, and was carried out after getting the participants' Informed Consent Term in writing.
Results
Regarding the characteristics of the 208 participants, ages ranged from 18 to 88 years, with an average of 63 years. The majority were women (126,60.0 %), white (191,92.0 %), who had a partner (157, 75.4 %) and had finished high school (133, 64.0 %). Among the participants, only 63 (30 %) were diabetic.
Based on the analysis of the interview transcripts, the central ideas and key expressions were identified, and the discourses of the three themes emerged from the guiding questions. The following topics are presented with their respective central ideas and patients' CSD.
Based on the analysis of the interview transcripts, the central ideas and key expressions were identified, and the discourses of the three themes emerged from the guiding questions were organized. Next, the themes are presented with the respective central ideas and the collective subject discourse. Table 1
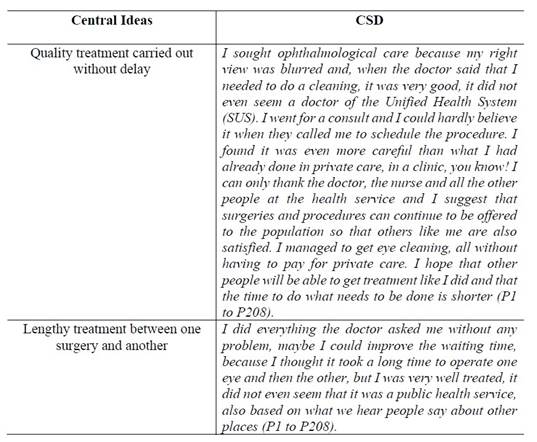
Table 1: Synthesis of central ideas and collective subject discourse related to the theme problem-solving ability of ophthalmological care from the participants' perspective
Table 2 presents the second theme "Obstacles to the accomplishment of the proposed care in the health care network", with the respective central ideas and collective subject discourse.

Table 2: Synthesis of central ideals and collective subject discourse related to the theme obstacles to the accomplishment of the care proposed in the health care network
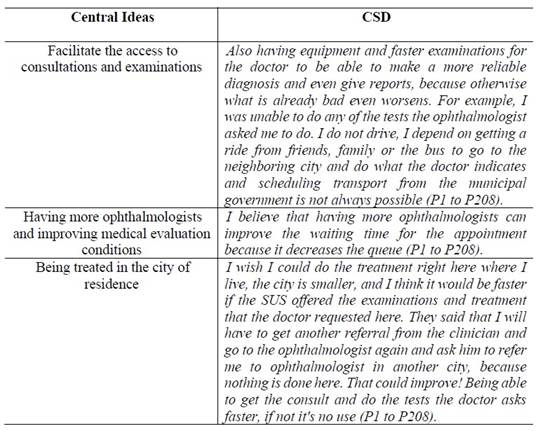
Table 3 presents the second theme "Contributions to the improvement of ophthalmic care” with the respective central ideas and collective subject discourse.
Discussion
The study results point out that, despite the waiting time, for many study participants, the problem-solving ability of ophthalmological care was achieved.
On the other hand, the lack of a service that prioritizes the users' emerging needs also comes to the fore. That situation hinders the achievement of some of the health system's basic objectives, such as, for example, the continuity of care, the resolution of problems at the appropriate level with equity and efficiency, as Brazilian public eye health policies guarantee.
The participants' discourse also reveals the lack of criteria that prioritize care for diabetics in screening for chronic complications. This supports the premise that health services are responding to a spontaneous demand, in a disjointed and discontinued manner.19
This is a fact that affects Diabetes Mellitus (DM) patients, whose eyes should be examined periodically for the prevention of blindness. It certainly denotes a setback in ophthalmological care through the SUS, which is multifaceted for the patients. On the one hand, there is the long-sought problem-solving ability and, on the other, the numerous obstacles that have to be overcome, reinforcing the reflection that the SUS is still disease- instead of health-centered.
The study also showed that only 30 % of the participants to whom eye care was indicated were diabetic, although this is one of the most prevalent diseases in the country. This fact shows us the extent to which people still neglect this care, despite all its not only eye-related complications.
Regarding the obstacles for the practice of eye care, the findings show the patients' difficulty to communicate with the service, with telephone as the only means. It is known that informing someone from a purely technical point of view does not mean clarifying. In this sense, it is suggested that the information be simple, attractive, understandable, and loyal, that is, arranged within the participants' standards of understanding.
The participants' discourse also revealed that, often, the information published in communication means and/or disseminated by the service is incorrect and inaccurate. It is assumed that this problem occurs because it is done by people without proper technical training.
Therefore, one of the proposals for improvement, as evidenced in the discourse, was to facilitate the access to consultations and exams, a situation that depends on the effective means of communication the services provide, which should be accessible to the population.
A study carried out in a Scottish city showed that a simple communication tool to ensure the safe transfer of information can speed up the information shared among the teams of secondary care services and help reduce major delays. 20
In this study, participants also mentioned the need to improve the conditions for medical evaluation. The lack of materials and equipment revealed in the discourse shows that ophthalmology, unlike what occurs in other medical specialties, requires managers' great investment in the acquisition of equipment. On the other hand, what is witnessed is a service with little infrastructure, increasingly challenging the health professionals in terms of care for the vulnerable population that demands ophthalmological care. 21
Therefore, the reality that emerges in the perception of the users interviewed in this study causes concern in the face of the current precarious situation of ophthalmological care in the SUS, with broken and even a lack of equipment to perform more complex examinations. Ophthalmological care in the SUS represents a challenge faced individually by each of the individuals who depend on the only resource they have to produce their conditions of existence: health.
This finding reinforces the need to build a model of health care that ensures the structuring of services, considering the dignity of patients as citizen.22
In this perspective, there is no consensus in the literature on the hiring of more doctors, as the study participants suggested. The understanding is that there is no lack of professionals, but that the SUS users lack appropriate access. 23
The data collected in the study also showed that being treated in one's own city could contribute to improve the problem-solving ability of ophthalmological care. This shows that patients are incorporated into the services they were referred to, but that this is not regulated at the points of origin, or that, when this is the case, this return is not formalized.(24, 25) This fact arouses reflections on the non-existence and/or non-effectiveness, as well as on the SUS users' lack of knowledge on a counter-referral system.
Thus, the ophthalmological care available in SUS faces a double challenge: to ensure comprehensive care to users and, at the same time, to implement health care networks that can address the needs, in view of persisting access difficulties and inequalities. The international literature on the prevention of blindness shows that, in Latin America, 60 % of the population does not have access to eye care, due to the lack of proper policy and the development of projects that create better eye health conditions. 26
Therefore, eye health programmes should be based on three fundamental pillars: development of human resources, infrastructure, as well as the integration of basic eye care into primary health care.
The central issue is how individual and collective, integral, and differentiated attention could be given to users who present such distinct problems. And also how health service managers should promote integral eye health through the SUS, as the system presents itself today, with difficulties of access, equity, bonding and continuous and problem-solving integral care for the users who turn to the services. 27
In this context, nurses have the mission to establish more democratic relationships with users and develop therapeutic proposals committed to the guidelines of the SUS and the Brazilian ophthalmological care policy, which excel in humanized care, focusing on the individuals and their biopsychosocial aspects. 14
In short, it grants health professionals the difficult task of implementing people-centered eye care integrated into health systems, and making eye care an integral part of universal health coverage.
Finally, it is acknowledged that one of the limitations of this research is related to the fact that it was conducted at a single center and with regional characteristics. Another factor to be considered is the memory bias, alluding to the time elapsed between care at the Integrated Health Center and the interviews by the researcher. In addition, the lack of studies on the topic in the health care network made it difficult to compare the results, which reinforces the need for further research in this area.
Conclusions
The difficulties the users revealed for the problem-solving ability ophthalmic care in secondary care reflect the lack of organization of this service, which in addition to not prioritizing care also does not commit to appropriate referral and follow-up.
In the discourse analysis, it was also evidenced that the lack of risk classification to prioritize care contributes not only to care delays, but also to the aggravation of potential complications deriving from diabetes.
In addition, the results also show that the city where the research was conducted does not control for the outcomes of ophthalmological evaluation requests.
Finally, it is expected that the study results, driven by nursing, can contribute to the reorganization of the service through a collective action and approach of health managers and services in combatting the worsening of eye health conditions, which directly affect the health and life of the population.
REFERENCES
1. Turrini RNT, Lebrão ML, Cesar CLG. Resolutividade dos serviços de saúde por inquérito domiciliar: percepção do usuário. Cad Saúde Pública. março de 2008;24(3):663-74. [ Links ]
2. Figueiredo AEB, Ceccon RF, Figueiredo JHC. Doenças crônicas não transmissíveis e suas implicações na vida de idosos dependentes. Ciênc saúde coletiva. janeiro de 2021;26(1):77-88. [ Links ]
3. Brasil. Ministério da Saúde. Secretaria de Atenção à Saúde. Política Nacional de Humanização. Formação e intervenção. Textos Básicos de Saúde. Cadernos HumanizaSUS (Internet). 2010. Disponível em: http://bvsms.saude.gov.br/bvs/publicacoes/cadernos_humanizaSUS.pdf [ Links ]
4. Cho NH, Shaw JE, Karuranga S, Huang Y, da Rocha Fernandes JD, Ohlrogge AW, et al. IDF Diabetes Atlas: Global estimates of diabetes prevalence for 2017 and projections for 2045. Diabetes Research and Clinical Practice. abril de 2018;138:271-81. [ Links ]
5. Brasil. Ministério da Saúde. Ministério da Saúde. DATASUS. Informações em Saúde - Mortalidade (Internet). 2015 (citado 21 de maio de 2021). Disponível em: Disponível em: http://www2.datasus.gov.br/DATASUS/index.php?area=0205&id=6937 [ Links ]
6. World Health Organization. World report on vision (Internet). 2019 (citado 21 de maio de 2021). Disponível em: Disponível em: https://www.who.int/publications/i/item/9789241516570 [ Links ]
7. de Carvalho KM, Zin A. Prevenção da cegueira e deficiência visual na infância. Rio de Janeiro: Cultura Médica; 2016. [ Links ]
8. Moll MF, Goulart MB, Caprio AP, Ventura CAA, Ogoshi AACM. O conhecimento dos enfermeiros sobre as redes de atenção à saúde. Rev enferm UFPE on line. 2017;11(1):86-93. [ Links ]
9. Brasil. Ministério da Saúde. Institui a política nacional de atenção em oftalmologia. Portaria 957/GM de 16 de maio de 2008. [ Links ]
10. Brasil. Ministério da Saúde. Implantação das Redes de Atenção à Saúde e Outras Estratégias da SAS. 2014. [ Links ]
11. Hirakawa TH, Costa W do C, Nakahima F, Ferreira AIC, Ribeiro LB, Ticianeli JG, et al. Knowledge of diabetic patients users of the Health Unic System about diabetic retinopathy. Revista Brasileira de Oftalmologia (Internet). 2019 (citado 1o de dezembro de 2020);78(2). Disponível em: Disponível em: http://www.gnresearch.org/doi/10.5935/0034-7280.20180106 [ Links ]
12. Pereira JM, Salomão SR, Cinoto RW, Mendieta L, Sacai PY, Berezovsky A, et al. Avaliação dos serviços de assistência ocular em população urbana de baixa renda da cidade de São Paulo - Brasil. Arq Bras Oftalmol. junho de 2009;72(3):332-40. [ Links ]
13. Alves Maftum M, Gonçalves da Silva Â, De Oliveira Borba L, Brusamarello T, Czarnobay J. Mudanças ocorridas na prática profissional na área da saúde mental frente à reforma psiquiátrica brasileira na visão da equipe de enfermagem Changes in professional practice in the mental health area against brazilian psychiatric reform in the vision of the nursing team. R pesq cuid fundam online. 11 de abril de 2017;9(2):309-14. [ Links ]
14. Santos EO dos, Eslabão AD, Kantorski LP, Pinho LB de. Nursing practices in a psychological care center. Rev Bras Enferm. 2020;73(1):e20180175. [ Links ]
15. Fernandes LA, Köptcke LS. Análise da ação de saúde ocular do Programa Saúde na Escola no Brasil de 2014 a 2019: um estudo transversal. Epidemiol Serv Saúde. 2021;30(2):e2020339. [ Links ]
16. Lefevre F, Lefevre AMC. O sujeito coletivo que fala. Interface (Botucatu). dezembro de 2006;10(20):517-24. [ Links ]
17. Lefevre F, Lefevre AMC, Marques MC da C. Discurso do sujeito coletivo, complexidade e auto-organização. Ciênc saúde coletiva. agosto de 2009;14(4):1193-204. [ Links ]
18. Tong A, Sainsbury P, Craig J. Consolidated criteria for reporting qualitative research (COREQ): a 32-item checklist for interviews and focus groups. International Journal for Quality in Health Care. 16 de setembro de 2007;19(6):349-57. [ Links ]
19. Machado LM, Colomé JS, Beck CLC. Estratégia de Saúde da Família e o sistema de referência e de contra-referência: um desafio a ser enfrentado. Rev Enferm UFSM. 21 de janeiro de 2011;1(1):31. [ Links ]
20. Testrow S, McGovern R, Tully V. Secondary care interface: optimising communication between teams within secondary care to improve the rehabilitation journey for older people. BMJ Open Qual. fevereiro de 2021;10(1). [ Links ]
21. Pereira JM, Salomão SR, Cinoto RW, Mendieta L, Sacai PY, Berezovsky A, et al. Avaliação dos serviços de assistência ocular em população urbana de baixa renda da cidade de São Paulo - Brasil. Arq Bras Oftalmol. junho de 2009;72(3):332-40. [ Links ]
22. Brasil. Ministério da Saúde. Secretaria de Atenção à Saúde. Departamento de Atenção Básica. Avaliação para melhoria da qualidade da estratégia saúde da família. (Internet). 2005. Disponível em: http://189.28.128.100/dab/docs/publicacoes/geral/doc_tec_amq_portugues.pdf [ Links ]
23. Gentil RM, Leal SMR, Scarpi MJ. Avaliação da resolutividade e da satisfação da clientela de um serviço de referência secundária em oftalmologia da Universidade Federal de São Paulo - UNIFESP. Arq Bras Oftalmol. 2003;66(2):159-65. [ Links ]
24. Silva CR, Carvalho BG, Cordoni Júnior L, Nunes E de FP de A. Dificuldade de acesso a serviços de média complexidade em municípios de pequeno porte: um estudo de caso. Ciênc saúde coletiva. abril de 2017;22(4):1109-20. [ Links ]
25. Machado MC, Kara-José N, Arieta CEL, Lourenço JLG, Carvalho R de S. A study of pent-up demand in ophthalmology: Divinolândia Hospital/Unicamp. Rev bras.oftalmol. dezembro de 2012;71(6):390-3. [ Links ]
26. Lansingh VC, Eckert KA. Vision 2020: the right to sight in 7 years? MEHDI Ophthalmol. 2013;2(2):26-9. [ Links ]
27. Martins AME de BL, Muniz AB, Silveira MF, Carreiro DL, Souza JGS, Ferreira EF e. Avaliação da assistência oftalmológica na perspectiva dos usuários. Rev bras epidemiol. junho de 2016;19(2):390-402. [ Links ]
How to cite: Meneguin, S., Fernandes Pollo, C., y Mainini Oliveira, I. R. User Difficulties for the Problem-Solving Ability of Ophthalmological Care in the Health Care Network. Enfermería: Cuidados Humanizados. 2021;10(2):29-41. DOI: https://doi.org/10.22235/ech.v10i2.2346
Contribution of the authors: a) Study conception and design, b) Data acquisition, c) Data analysis and interpretation, d) Writing of the manuscript, e) Critical review of the manuscript. S. M. contributed in a, c, d, e; C. F. P. in e; I. R. M. in a, b, c, d, e.
Received: November 23, 2020; Accepted: June 25, 2021
 Este é um artigo publicado em acesso aberto sob uma licença Creative Commons
Este é um artigo publicado em acesso aberto sob uma licença Creative Commons
