










Services on Demand
Journal

Article
 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Related links
Share

 Permalink
PermalinkEnfermería: Cuidados Humanizados
Print version ISSN 1688-8375On-line version ISSN 2393-6606
Enfermería (Montevideo) vol.10 no.1 Montevideo June 2021 Epub June 01, 2021
https://doi.org/10.22235/ech.v10i1.2481
Original Articles
Perception of hospitalized patients in medical surgical units on humanized nursing care

1 Universidad de Concepción, Chile pjara@udec.cl
2 Universidad Autónoma de Nuevo León, México
Keywords: humanization of assistance; holistic nursing; quality of health care; nursing care.
Palabras clave: humanización de la atención; enfermería holística; calidad de la atención de salud; atención de enfermería.
Palavras-chave: humanização da assistência; enfermagem holística; qualidade da assistência à saúde, cuidados de enfermagem.
Introduction
Advances in knowledge and technology have modified the care provided in the health sector, which is becoming increasingly sophisticated and specialized, being a permanent concern for health professionals, mainly nursing (1).
Although this process has helped the early investigation and control of certain diseases, it has also generated a more fragmented care of the human being, a fact that is evident in the users of the health system, who feel vulnerable to professionals who are more focused on clinical techniques and procedures than on the person himself/herself (1-3). This phenomenon also affects nursing, due the structural and organizational characteristics of health system generates a gap that deviates from its essence, which is the holistic and comprehensive care of people, an aspect that is closely related to the humanization of care (4), a quality demanded by nursing practice today (5-6). That is why in recent years the term humanized care has emerged with greater force, along with the need to analyze and eliminate the barriers that arise in the current exercise of care (7), in response to facts totally against it, and in fact, they are related to distancing and depersonalization of health professionals (6). In addition, the actions generated from an impersonal and undifferentiated care can affect more deeply people who are going through a state of vulnerability, such as sick people, since they often face a process characterized by anxiety, fear, and pain (8).
In relation to these evidences, nursing plays a fundamental role, because it is globally recognized that it is the discipline of care, and its central axis is based on providing comprehensive care to the person, family and community (9). Thus, many nursing theorists consider care as a practical basis of the profession (10-12), care that refers to the interaction and adaptation between the nurse and the person when the action of assisting is exercised, an act that is inserted in the conception of totality and integrality (13-14). From this perspective, the theoretical framework that supports this study corresponds to the theory of transpersonal care by Jean Watson (10). This theory was born from his concern to give a new meaning and dignity to the world of nursing and the care of people and establishes that:
In view of the risk of dehumanization in patient care, due to the great administrative restructuring of most health care systems in the world, it is necessary to rescue the human, spiritual and transpersonal aspect, in clinical, administrative, educational and research practice by nurses (15).
The PCHE instrument was derived from Watson's theory (10), which contains 3 implicit components in its 10 caritas factors, which are: quality, provision of care and communication (16-17). This instrument is based on the humanistic vision of the world, where the act of caring is not a mere procedure, but an interconnected, intersubjective process of shared sensations between the patient and the nurse. From this perspective, it is the nurse who should help the patient to increase their harmony within the mind, body and soul (10). The quality dimension of nursing work is integrated into the 10 caritas factors of Jean Watson's theory, since the actions considered in these points to the delivery of comprehensive care that considers the human being as a whole. So, when we understand care from that perspective, it becomes a care of excellence (18). At the same time, the dimension of care provision is also integrated into these care factors and can be appreciated through the reagents of the instrument which presents actions to be evaluated such as: allowing the expression of feelings of the sick person, worrying about her state of mind, giving a warm and welcoming care within others, this items are present in factor 5 and 8 of the caritas process “promotion and acceptance of feelings” and in “provision of a supportive, protective and corrective environment mental, physical, sociocultural and spiritual” (10, 18). The effective communication dimension of the instrument is directly related to factor 8 of the caritas process, where you have 8 questions aimed to evaluate both the external and internal environment, an important aspects to the person who is in a condition of illness and disease, such as: safety, comfort, shelter and specifically the communication itself, as well as the opportunity to satisfy a requirement that has been presented, such as: If they answered questions clearly, if they identified themselves with their name and position before performing any procedure, if they took time to clarify their concerns, if they gave explanations when the patient requested them, if they looked into his eyes when they spoke to him/her and if they provided him/her with enough information to make decisions for himself/herself (16, 18).
Scientific studies support the characteristics or factors that comprise a humanized care, where they were mainly identified as relevant: listening, dialogue, true presence, welcoming, bonding and incorporation of the family. Likewise, they relate the perception of humanized nursing care according to variables such as age, sex, origin, educational level, monthly income per person and partner status (21, 23-24).
Faced with this reality, it was considered of utmost importance to inquire about this phenomenon in the field of closed care in public health institutions in Chile, specifically collecting information from the perspective of hospitalized people where the disease, interventions, examinations, procedures, among others, keep them away from their families and give rise to feelings such as frustration and uncertainty, which can also cause anxiety and rejection (4).
Therefore, the objective of this study was to analyze the perception of patients hospitalized in medical-surgical services on the humanized care of nursing professionals, and secondarily to identify the most relevant dimension in terms of humanized care and relate the perception of this with bio sociodemographic variables.
Method
Descriptive, correlational, cross-sectional study, which was carried out for 8 months, in 3 public hospitals of the Eighth Region of Chile, during 2017. The study population corresponded to people (men and women), adult (over 18 years of age), hospitalized in medical-surgical units of those health establishments. The sample was probabilistic, simple random. The universe was known, and it corresponded to the total number of hospitalized patients in medicine and surgery in the healthcare centers participating in this research, which corresponded to 250 people. With this data applied to the statistical formula for sample calculation where an alpha of 5 % and a confidence level of 95 %, a sample size of 152 was obtained, which was finally made up of 150 people, since two did not agree to participate in the study, distributed proportionally in the 3 establishments. The sample consisted of sick people who met the following inclusion criteria: with more than 3 days of hospitalization, over 18 years of age, and intellectually and physically enabled to respond to the instrument, which was compared with the application of 3 questions that had to be correctly answered by the users before starting with the application of the survey, these were: What day is it today? What is your name? and Where are you? And at the same time, they did not present pain and their participation was voluntary in relation to the informed and signed consent. For the selection of the sample, the Random Number software was used, which allows obtaining numbers randomly, with which it was possible to select the people participating in the study and the days on which the survey would be applied.
The instrument used was: Perception of Humanized Care Behaviors in Nursing with prior authorization from its authors (16-17), which is based on Jean Watson's theory of transpersonal care (10). Before its application, a cultural and linguistic adaptation (25) was carried out for subsequent validation of the construct by convergence (26), with the aim of avoiding biases derived from language (27), and to make easier the clarity and understanding of the instrument by Chilean users. So, finally was composed by 32 items which were the same three dimensions of the original instrument (17-18): quality of nursing work, which includes 7 items; provision for care, with 17 items; and effective communication, with 8 items (25). For the interpretation of the results of the instrument, the responses were classified into four measurement categories: always, almost always, sometimes, almost never. This categories were for the general (global) perception and for each of its dimensions (Table 1).
Table 1: Measurement categories according to score for the three dimensions of the PCHE instrument
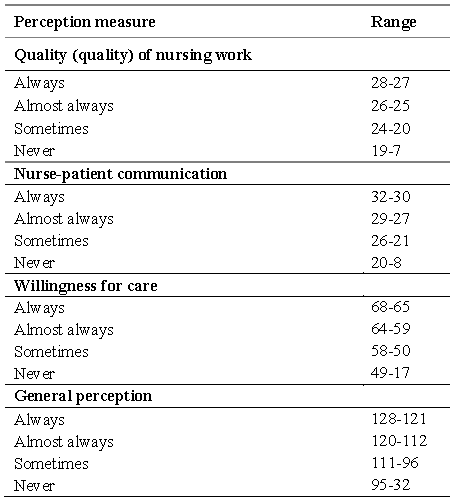
Source: Perception of hospitalized patients in medical surgical units on humanized nursing care.
In the data collection, we went to each of the healthcare centers where the inclusion criteria were verified and they were invited to participate voluntarily, explaining the informed consent to each participant before requesting the information required for the study. In the process, a group of last-year nursing students participated, previously inducted in the research protocol, who applied the survey in a personalized way, this process lasted 6 months. To profile the participants, a previously prepared data card was used, which stipulated the sociodemographic variables that were going to be required for this study. The quality control of the data was protected by measuring the reliability of the instrument, the Cronbach's alpha coefficient was 0.96, considered excellent, which showed that the elements of the scale were homogeneous and the averages correlations between the items were consistent, giving the scale reliability. For all its dimensions, it presented values above acceptable according to the criteria of George and Mallery (28; Table 2).
Table 2: Cronbach's alpha of the global PCHE instrument and by dimensions
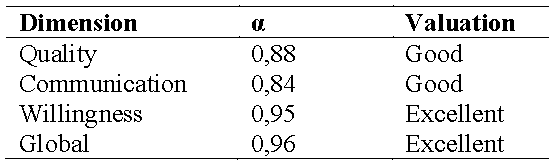
Source: PCHE validation for Chile.
A cross-cultural linguistic adaptation of the PCHE instrument version 2014 Colombia (17) was carried out previously, so that the items contemplated in it were clear and easy to understand for the Chilean population, avoiding biases derived from language (25).
In addition, the construct validity was evaluated by convergence when applied in conjunction with another instrument (Instrument for the assessment of humanized care provided by nursing professionals to hospitalized people; 29) that measured the same study phenomenon, this stage of the research was carried out through the pilot test. With the validation by construct, the results showed that the new questionnaire (29) was very clear and understandable for Chilean people, presenting a positive correlation with the other instrument evaluated with 0.73, evidencing a positive convergence, determining an adequate validity of the construct or content of the PCHE instrument version adapted to the Chilean population (25).
For the demographic characterization and for the analysis of the perception of humanized care behaviors granted by nurses, descriptive, inferential parametric statistics were used, using means, standard deviation, minimum and maximum value and use of percentages. To check the significant differences between the studies groups (sociodemographic variables), the dimensions of the instrument were used Anova and to identify the groups in which there were greater differences the Tukey posttest was used. To perform the correlation of the data should be established normality in the first place using the Shapiro - Wilk test, resulting in the data not being distributed in a normal way, having to resort to nonparametric statistics, so for the correlations were worked with the Spearman Rho. This data analysis was performed through of the SPSS version 24.0 social science statistical package.
The ethical aspects were protected with the presentation and approval of the project by the Ethics Committee of the Universidad de Concepción, Chile, resolution 014-16 and by the Scientific Ethics Committee of the Talcahuano Health Service, Chile; Act n ° 49 2016, entity of which depend on the three public establishments participating on the study. Subsequently, data collection is carried out, prior to the signing of informed consent, containing the ethical requirements of Ezekiel Emanuel. Standards and guidelines of the World Medical Association were complied, as well as the Declaration of Helsinki, to protect rights and respect for human dignity in scientists’ studies.
Results
In relation to the sociodemographic information, which characterizes the study population, the sample was made up of a balanced proportion of women and men, where the percentage corresponded to 52 and 48 %, respectively. The average age was 55 years, 78 % had basic and secondary studies that did not exceed technical or university education. In relation to income level, more than half of this group of people received a monthly salary of less than 300 thousand Chileans pesos (approximately US$ 380) and most of them were in a relationship, corresponding to 54 % of the sample. According to the distribution of patients by type of unit, this was presented in a fairly balanced way, with 54 % of patients in medical units and 45 % in surgical units, most of them were hospitalized with a stay of one week, with a minimum of 3 days and a maximum of 3 months.
The global results of the application of the instrument were the following: The average score of the humanized care behavior of the nurses was 117.6, which corresponds to the concept almost always. When appreciating the result of the categorization of the perception of behaviors of humanized nursing care, it is evident that the concept that predominated was that of always, for which the perception of the patients was favorable in favor of the practice of humanized care.
In relation to the perception of humanized care behaviors by clinical services, it was found that this was similar for both units, with an average score for Medicine of 117.5 and for Surgery of 117.8 values that are within the categorization of usually (Table 3).
Table 3: Perception of caring behaviors humanized nursing by hospital and total
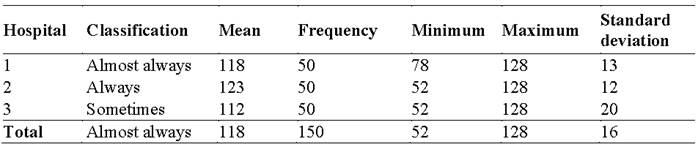
Source: Perception of hospitalized patients in medical surgical units on humanized nursing care.
According to the dimensions of the PCHE instrument, they correspond to: Quality of nursing work, willingness to care and openness to nurse-patient communication, the results found were the following:
Although these three dimensions were mostly evaluated with a positive perception of humanized care behaviors, the category always prevailing with 69.3 % for the quality of nursing work, 66.7 % for willingness to care and a 56.7 % for openness to communication. It’s important saying that the latter obtained the lowest percentage of positive perception, in turn it was the one that presented a higher proportion of responses with negative connotations in relation to the other dimensions (16 % in the category sometimes versus 14 % for care provision and 7.3 % for quality of nursing work; Table 4).
Table 4: Categorized dimensions of the PCHE instrument
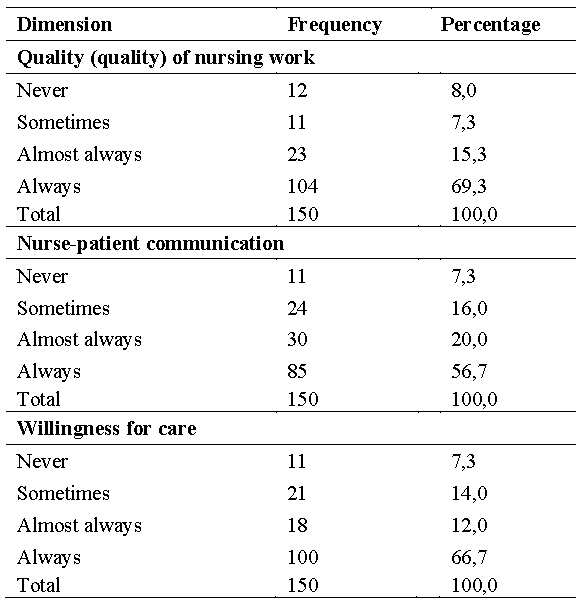
Source: Perception of hospitalized patients in medical surgical units on humanized nursing care.
Regarding the relationships between PCHE and sociodemographic variables: no significant relationship was found between age and the perception of humanized nursing care behaviors. It was only evidenced that it was direct, but not statistically significant (Spearman's Rho correlation coefficient 0.099; p = 0.227).
In relation to the perception of humanized nursing care behaviors and the gender variable, men and women presented averages of 116 and 119.1 points, respectively. Values that are within the categorization: almost always, variables in which no significant relationship was found (p = 0.229). When analyzing the information based on the dimensions of the PCHE instrument and the sex variable, it could be seen that the average scores of all of them in relation to men and women were within a positive perception. After applying Anova, no significant differences were found (Quality p = 0.3189; Communication p = 0.343; Availability = 0.191).
When analyzing the clinical service variable, it was identified that there were no relevant differences for the global perception of humanized nursing care behaviors (p = 0.912) and its dimensions (Quality p = 0.719; Communication p = 0.864; Disposition p = 0.805).
Regarding the days of hospitalization, no significant associations were found between this variable and the global perception of humanized care behaviors (Spearman's Rho correlation coefficient -0.093, p = 0.256) or its dimensions.
For educational level, no significant associations were found between this variable and the global PCHE (Spearman's Rho correlation coefficient -0.132, p = 0.108). However, when analyzing the dimensions of the instrument based on the educational level, a subtle difference was investigated between the different groups, where it was possible to appreciate that for effective communication the lowest perception is presented in the group with the highest educational level. It is important to highlight that even obtaining statistical significance, the number of participants with a university education was very small in relation to that of the others.
For monthly income, no relationships were found between this variable and the PCHE (Spearman's Rho correlation coefficient 0.106, p = 0.199), nor for its dimensions. No significant differences were found for partner status, both for global PCHE and for its dimensions.
Discussion
The study allowed characterizing the sample of people hospitalized in medical-surgical units of three public hospitals in the Eighth Region of Chile. Of the sample, about half corresponded to women and the other to men, making up a proportionally balanced group with respect to sex, which was relevant in the study to avoid perceptions bias influenced by the predominant sex of the participants. Similar results were found in other investigations where the groups distributed by sex presented a fairly homogeneous division (21-24). Regarding age, the average was located at 55 years, coinciding with the analysis of another research that investigated the perception of humanized care provided by nursing (21). The predominance of age in the present study can be attributed to the fact that it was carried out with patients who presented medical-surgical pathologies, within the latter many surgeries were elective, and therefore they mainly involved younger people (30).
Regarding the possible incidence of sociodemographic variables in the perception of humanized nursing care behaviors, no significant associations were found, for which the variables: days of hospitalization, sex, age, income level and educational level would not be influencing the perception of humanized care by the patients involved in this study, similar findings were found in other investigations (24, 31-32). These conditions mentioned are not variables that allow differentiation of perception, since all had a high perception of humanized care and it is possible that the condition of being sick, hospitalized and feeling vulnerable does not allow making a difference and can make any help be perceived as humanized (19), perhaps following up with these patients when they are already discharged and at home could provide a variation in this perception, which is suggested for future research.
Although the bio sociodemographic variables did not present statistical significance in relation to the perception of humanized nursing care behaviors, all the information emanating from the sociodemographic characterization of this population emerges as an aspect of great interest to nursing. Mainly due to its contribution to nursing assessment stage, since there must be tools that allow us to understand the social reality from which the person being cared for comes from and the implications that these characteristics have on the care plan that must be offered to them and their families.
In this way, the study revealed that the socioeconomic level of this population was medium-low (33) evidenced by an income level where more than half of this group received a monthly salary of less than 300 thousand Chilean pesos (380 dollars approximately). This finding matches with results reported by other investigations where the majority belonged to stratum 1, that is, lower class (20-21). Another study with results similar with this research, shows the predominance of the social class belonging to the low-low stratum and the low stratum (34). Related to this this aspect is the educational level, where it should be noted that 79 % of the sample indicated studies that did not exceed technical or university education, this shows a low level of instruction. However, they were all literate, an important aspect to consider, having consider the difficulties and vulnerability of this group of people in relation to their disease process and the care required. Similar investigations in other studies indicate that most of the participants in research on the perception of humanized care provided by nursing did not finish primary school or had not completed secondary school (20-21).
This is how the information emanated based on the income and educational level of the participants is considered of great relevance for nursing knowledge, since this condition is associated with the vulnerability presented by users of public health system, a finding which is consistent with that reported by CEPAL (35), where it is established that social determinants, such as not having access to education, precarious work related to low income, are linked to social vulnerability (35). In addition, this condition can generate that the needs of this group of people are greater than those presented by those of higher social strata, for which, the nurse must have knowledge of the social reality of these people and a special sensitivity to be able to identify in a timely and effective manner the real needs of this population.
In relation to the perception of humanized care behaviors in nursing, it was found that this was high by hospitalized people, which evidenced a good provision of humanized nursing care, considering that this variable was measured in four classification criteria (very good, good, average, and bad). Similar results are found in investigations where the general perception of humanized care behaviors by nursing was perceived as excellent (20-21, 24, 36). This fact could be given because in a vulnerable condition, all help received can be considered as humanized care, which is transversal to every person or family that goes through the hospitalization process (19), since being hospitalized in an adult unit there is no less sensitivity to value this direct relationship of humanized care (19). The foregoing, in relation to one of the studies carried out in a pediatric unit (36), where it is concluded that there is great sensitivity on aspects that are directly related to the humanization of care.
The findings by dimension of humanized care showed that the quality of care and provision of care were the dimensions best evaluated by the participants and effective communication obtained a lower appreciation. This result may be influenced by the current trend that exists at a national and international level regarding the preponderance of accreditation processes, giving relevance to technical-administrative quality (37), which could be having a favorable impact on the quality of care provided and on the provision for care. However these same processes that imply a high demand for the nurse can have a direct impact on professional practice, which could be influencing the less time the nurse has to be able to establish effective communication with the people in their care (36, 38-40).
At the same time, quality of care work and disposition for care that obtained a high positive perception on the part of hospitalized people, in light of the theory, the items evaluated point to the treatment received, to feel like a person when treated, to feel that is well cared for and calm (25), which are elements that in Watson's theory are integrated into the factors of the caritas process (10), which suggests that nurses in their daily work carry out actions that contribute to the maintenance of an interpersonal relationship of quality with the person in their care. However, it should not be overlooked that, in this study, although it was in a lower percentage, there were people who presented a low perception of these dimensions, which could be due to the work overload of nurses (6), therefore which is important to ensure labor well-being so that this aspect does not negatively affect the delivery of humanized care. In the same way, this fact could be negatively influencing the perception of the effective communication dimension, since this, without its appreciation being low, turned out to be the dimension with the highest negative perception on the part of hospitalized people, which is an aspect that must be analysed in depth, since communication, in the light of Watson's theory (10), is the fundamental and central aspect of the nurse-patient relationship (10-18).
In the breakdown by dimensions, it was possible to investigate that there was an orientation between age and perception of the quality of care provided by nursing and even though this turned out to have slight statistical significance, the direct relationship was not strong (r = 0.175 p = 0.033) , this fact prevents its generalization, therefore, this finding coincides with the results of another study where it was not possible to establish a relationship between sociodemographic variables and the perception of quality of care. This phenomenon would be given because the user, regardless of their age, has needs and expectations that influence the perception of the quality of care they receive (41).
Finally, due to the results obtained, it is considered of utmost importance to strengthen more human aspects, such as the communication in nursing work. Since this dimension has been the least approved, reveals a weakness that must be addressed. As Watson (10) suggests, communication is the fundamental pillar to strengthen the nurse-patient relationship, especially its affective and communicative aspects (10-18). Aspect highlighted by users, who attach great importance to the cordial relationship established between them and the nurses in charge of their care (42-43). So, this dimension of care emerges as relevant, which is why it is essential to strengthen it in the work environment. In this way the delivery of humanized care by the nurse is favored.
At the same time, the importance that hospitalized people give to the delivery of humanized care by nurses is highlighted and although in this study the perception of this area was well evaluated, there are still aspects that are visualized as areas of opportunity for nursing, such as seeking strategies that improve communication processes with patients and strengthen care environments, as mentioned by Watson (10), from both a physical and spiritual perspective (10, 43).
Through this study, it was possible to appreciate that the need to be treated with dignity and receive humanized care by nursing staff predominates in the human being, which highlights the need to deliver humane, ethical and dignified care to all patients without distinction. This poses a challenge to nursing in the face of social inequalities that exist today in health (41).
Conclusions
The study showed a good perception about the humanized care by nurses of people hospitalized in medical-surgical units of three hospitals in the Eighth Region in Chile.
In addition, it was investigated that of the three dimensions that the instrument presents in relation to humanized care, the one that obtained the highest average score was the quality of nursing work, which could be influenced by the current accreditation processes that Chilean hospitals have undergone, which has required the delivery of high-quality care, which may also be positively affecting the provision to care dimension.
The dimension which results in a lower average of positive perception was communication, it is striking that these basic characteristics of communication being the axis of the training curricula for nurses, part of the nursing principle of maintaining the individuality of the patient human being and axis of the caritas process of Watson’s theory reached only 56.7 % of being always present. Although the interpretation of the scale is global, this dimension when adding the category always and almost always reached close to 80 % of the presence of humanized care, but 20 % of the patients declare their perception of this careful only sometimes or never. This shows that this is an area that must be strengthened by nurses, since it is essential in the delivery of comprehensive and individualized care, since it allows an adequate assessment and planning of effective care.
Also in today's societies, every time more individualized, communication becomes a necessary social skill to interact with the other, which is essential in nursing work, thus opening an opportunity for improvement in relation to this area.
This research has allowed to delve into the subject of humanized care, allowing to have a greater understanding of the phenomenon under study and at the same time provides information that can be deepened in future investigations.
As a limitation of the study, it is possible to mention the time that was used in presenting the research project to the different ethics committees, and the time used in presenting this project to the directives of the healthcare centers where the study was carried out.
REFERENCES
1. Arredondo-González C, Siles-González J. Tecnología y Humanización de los Cuidados: Una mirada desde la Teoría de las Relaciones Interpersonales. Index de Enfermería (Internet). 2009 (citado 9 agosto 2020); 18(1):32-36. Disponible en: https://doi.org/10.4321/S1132-12962009000100007 [ Links ]
2. Poblete M, Valenzuela S. Cuidado humanizado: un desafío para las enfermeras en los servicios hospitalarios. Acta Paulista de Enfermagem (Internet ). 2007 (citado 9 agosto 2020); 20(4):499-503. Disponible en: https://doi.org/10.1590/S0103-21002007000400019 [ Links ]
3. Gálvez M, Gómez J, Martín M, Ferrero M. Humanización de la Sanidad y Salud Laboral: Implicaciones, estado de la cuestión y propuesta del Proyecto HU-CI. Medicina y Seguridad del Trabajo (Internet ). 2017 (citado 9 agosto 2020); 63(247):103-119. Disponible en: http://scielo.isciii.es/scielo.php?script=sci_arttext&pid=S0465-546X2017000200103&lng=es [ Links ]
4. Salazar O. Humanized Care: A Challenge for Nursing. International Archives of Nursing and Health Care (Internet ). 2018 (citado 9 agosto 2020); 4(2). Disponible en: doi.org/10.23937/2469-5823/1510092 [ Links ]
5. De Souza Corbani N, Passarela Brêtas A, Cassuli Matheus M. Humanização do cuidado de enfermagem: o que é isso? Revista Brasileira de Enfermagem (Internet ). 2009 (Citado 9 agosto 2020); 62(3):349-54. Disponible en: https://doi.org/10.1590/S0034-71672009000300003 [ Links ]
6. Beltrán-Salazar O. Cuando las enfermeras están ausentes. Index de Enfermería (Internet ). 2010 (Citado 9 agosto 2020); 19(4):240-244. Disponible en: http://scielo.isciii.es/scielo.php?script=sci_arttext&pid=S1132-12962010000300002&lng=es [ Links ]
7. Beltrán-Salazar O. The meaning of humanized nursing care for those participating in it: Importance of efforts of nurses and healthcare institutions. Investigación y Educación en Enfermería (Internet ). 2016 (citado 9 agosto 2020); 34(1):18-28. Disponible en: https://doi.org/10.17533/udea.iee.v34n1a03 [ Links ]
8. Pezoa M. ¿Qué elementos de la atención en salud son, desde la perspectiva del usuario los que más contribuyen a que se sienta satisfecho? Santiago: Superintendencia de Salud (Internet ). 2012 (citado 9 agosto 2020). Disponible en: http://www.supersalud.gob.cl/normativa/571/articles-7392_recurso_1.pdf [ Links ]
9. Moreno-Fergusson M. Humanización del cuidado: una meta enraizada en la esencia de enfermería. Aquichan (Internet ). 2013 (citado 10 agosto 2020); 13(2):146-147. Disponible en: https://aquichan.unisabana.edu.co/index.php/aquichan/article/view/3515 [ Links ]
10. Watson J. The philosofhy and science of caring. 1a ed. Colorado: University Press of Colorado; 2008. [ Links ]
11. Raile M, Marriner A. Modelos y teorías en enfermería. 9a ed. Barcelona: Elsevier; 2018. [ Links ]
12. Eriksson K. The Theory of Caritative Caring: A Vision. Nursing Science Quarterly. 2007; 20(3): 201-2. [ Links ]
13. Duran M, Gutierrez E, Pino N, Sanchez B, Vasquez E, Villagra L. Dimensiones del cuidado. 1a ed. Colombia: Facultad de Enfermería, Universidad Nacional de Colombia; 1998; p. 103-108. [ Links ]
14. Busch I, Moretti F, Travaini G, Wu A, Rimondini M. Humanization of Care: Key Elements Identified by Patients, Caregivers, and Healthcare Providers. A Systematic Review. The Patient (Internet ). 2019 (citado 10 agosto 2020); 14(1):461-474. Disponible en: https://doi.org/10.1007/s40271-019-00370-1 [ Links ]
15. Beltran-Salazar O. Cuidado humanizado: una relación de familiaridad y afectividad. Investigación y Educación en Enfermería (Internet ). 2015 (citado 10 agosto 2020); 33(1):17-27. Disponible en: http://www.scielo.org.co/scielo.php?pid=S0120-53072015000100003&script=sci_arttext&tlng=es [ Links ]
16. Rivera L, Triana A. Percepción de comportamientos de cuidado humanizado de enfermería en la Clínica del Country. Avances en Enfermería (Internet ). 2007 (citado 10 agosto 2020); 25(1):56-68. Disponible en: https://revistas.unal.edu.co/index.php/avenferm/article/view/35901 [ Links ]
17. González-Hernández O, Validez y confiabilidad del instrumento Percepción de comportamientos de cuidado humanizado de enfermería PCHE 3ª versión. Aquichan (Internet ). 2015 (citado 10 agosto 2020); 15(3):381-392. Disponible en: https://doi.org/10.5294/aqui.2015.15.3.6 [ Links ]
18. Urra M, Jana A, García M. Algunos aspectos esenciales del pensamiento de Jean Watson y su teoría de cuidados transpersonales. Ciencia y Enfermería (Internet ). 2011 (citado 9 agosto 2020); 17(3):11-22. Disponible en: http://dx.doi.org/10.4067/S0717-95532011000300002 [ Links ]
19. Waldow V. Cuidado humano: la vulnerabilidad del ser enfermo y su dimensión de trascendencia. Index de Enfermería (Internet ). 2014 (citado 10 agosto 2020); 23(4):234-238. Disponible en: http://dx.doi.org/10.4321/S1132-12962014000300009 [ Links ]
20. Bautista-Rodríguez L, Parra-Carrillo E, Arias-Torres K, Parada-Ortiz K, Ascanio-Meza K, Villamarin-Capacho M. Percepción de los comportamientos de cuidado humanizado en los usuarios hospitalizados en una institución de salud de 3° y 4° nivel de atención. Revista Ciencia y Cuidado (Internet ). 2015 (citado 9 agosto 2020); 12(1):105-118. Disponible en: https://doi.org/10.22463/17949831.331 [ Links ]
21. Romero E, Contreras I, Moncada A. Relación entre cuidado humanizado por enfermería con la hospitalización de pacientes. Hacia la Promoción de la Salud (Internet ). 2016 (citado 9 agosto 2020); 21(1):26-36. Disponible en: http://dx.doi.org/10.17151/hpsal.2016.21.1.3 [ Links ]
22. González D. Percepción de Comportamientos de Cuidado Humanizado en Estudiantes de Enfermería. Actualizaciones en Enfermería (Internet ). 2014 (citado 9 agosto 2020); 17(2):14-21. Disponible en: https://encolombia.com/medicina/revistas-medicas/enfermeria/ve-172/percepcion-comportamientos-humanizado/ [ Links ]
23. Castelo-Rivas W, García-Vela S, Viñan-Morocho J. Cuidado humanizado de enfermería a pacientes con pie diabético del Hospital General Santo Domingo- Ecuador. Archivo Médico Camagüey (Internet ). 2020 (citado 8 diciembre 2020); 24(6):801-813. Disponible en: http://revistaamc.sld.cu/index.php/amc/article/view/7169 [ Links ]
24. Monje P, Miranda P, Oyarzün J, Seguel F, Flores E. Percepción de cuidado humanizado de enfermería desde la perspectiva de usuarios hospitalizados. Ciencia y Enfermería (Internet ). 2018 (citado 8 agosto 2020); 24(5). Disponible en: http://dx.doi.org/10.4067/s0717-95532018000100205 [ Links ]
25. Melita-Rodríguez A, Jara-Concha P, Pereira DI, Luengo Machuca L. Adaptación transcultural y validación de un cuestionario de cuidado humanizado en enfermería para una muestra de población chilena. Revista Cuidarte (Internet ). 2018 (citado 8 enero 2021); 9(2):2245-56. Disponible en:://doi.org/https 10.15649/cuidarte.v9i2.531 [ Links ]
26. Cardona-Arias J, Ospina-Franco L, Eljadue-Alzamora A. Validez discriminante, convergente/divergente, fiabilidad y consistencia interna, del whoqol-bref y el mossf-36 en adultos sanos de un municipio colombiano. Revista Facultad Nacional de Salud Pública (Internet ). 2015 (citado 14 agosto 2020); 33(1):50-57. Disponible en: Disponible en: https://revistas.udea.edu.co/index.php/fnsp/article/view/15865 [ Links ]
27. Ramada-Rodilla J, Serra-Pujadas C, Delclós-Clanchet G. Adaptación cultural y validación de cuestionarios de salud: revisión y recomendaciones metodológicas. Salud Pública de México (Internet ). 2013 (citado 10 agosto 2020); 55(1):57-66. Disponible en: https://doi.org/10.1590/S0036-36342013000100009 [ Links ]
28. Frías-Navarro D. Análisis de fiabilidad de las puntuaciones de un instrumento de medida. Alfá de Cronbách: un coeficiente de fiabilidad. (Internet ) España: Universidad de Valencia; 2014 (citado 14 agosto 2020). Disponible en: https://docplayer.es/22648856-Apuntes-de-spss-dolores-frias-navarro-universidad-de-valencia-2014.html [ Links ]
29. Hermosilla A, Mendoza R, Contreras S. Instrumento para valoración del cuidado humanizado brindado por profesionales de enfermería a personas hospitalizadas. Index Enferm (Internet ). 2016 Dic (citado 2021 Mayo 16) ; 25( 4 ): 273-277. Disponible en: http://scielo.isciii.es/scielo.php?script=sci_arttext&pid=S1132-12962016000300011&lng=es. [ Links ]
30. Nazar C, Zamora M, González A. Cirugía ambulatoria: selección de pacientes y procedimientos quirúrgicos. Revista Chilena de Cirugía (Internet ). 2015 (citado 8 agosto 2020); 67(2):207-213. Disponible en: http://dx.doi.org/10.4067/S0718-40262015000200017 [ Links ]
31. Reis C, Sena E, Fernandes M. Humanization care in intensive care units: integrative review. Revista de Pesquisa: Cuidado é Fundamental Online (Internet ). 2016 (citado 8 agosto 2020); 8(2):4212-4222. Disponible en: https://doi.org/10.9789/2175-5361.2016.v8i2.4212-4222 [ Links ]
32. Silva-Fhona J, Ramón-Cordova S, Vergaray-Villanueva S, Palacios-Fhon V, Partezani-Rodrigues R. Percepción del paciente hospitalizado respecto a la atención de enfermería en un hospital público. Enfermería Universitaria (Internet ). 2015 (citado 8 agosto 2020); 12(2):80-87. Disponible en: https://doi.org/10.1016/j.reu.2015.04.001 [ Links ]
33. Departamento de estudios sociales. Estratificación Socioeconómica en Encuestas de Hogares (Internet ). Chile: Instituto Nacional de Estadísticas; 2011 (citado 14 marzo 2020). Disponible en: historico.ine.cl/canales/menu/publicaciones/estudios_y_documentos/documentostrabajo/estratificacion_socioeconomica_encuestas_hogares.pdf [ Links ]
34. Jiménez M, Fuentes-González N. Percepción de la calidad del cuidado de enfermería en pacientes diabéticos hospitalizados. Revista Investigación en Salud Universidad De Boyacá (Internet ). 2018 (citado 14 marzo 2020); 5(2): 219-245. Disponible en:://doi.org/https 10.24267/issn.2389-7325 [ Links ]
35. Mesa Directiva de la Conferencia Regional sobre Desarrollo Social de América Latina y el Caribe. La matriz de la desigualdad social en América Latina (Internet ) Santo Domingo: CEPAL; 2016 (citado 14 marzo 2020). Disponible en: https://repositorio.cepal.org/bitstream/handle/11362/40668/4/S1600946_es.pdf [ Links ]
36. González-Ruiz G, Oviedo-Córdoba H, Bedoya-Idrobo L, Benavides-Peñaloza G, Dalmero-Arvilla N, Vergara-Ascanio C. Cuidado humanizado de enfermería percibido por familiares de pacientes pediátricos, usuarios del Hospital Fernando Troconis en Santa Marta. Memorias. 2013; 11(20):31-39. [ Links ]
37. Kafruni N, Castro Del Toro M. Sistema integrado de gestión para las IPS de alta complejidad de la ciudad de Barranquilla basado en los estándares de acreditación en salud, el modelo European foundation for quality management y el Balanced Scorecard. Prospectiva (Internet ). 2018 (citado 14 marzo 2020); 16(1):91-99. Disponible en: https://doi.org/10.15665/rp.v16i1.1468 [ Links ]
38. Hernández R, Moreno M, Cheverría S, Landeros M, Interial M. Cuidado de enfermería perdido en pacientes hospitalizados en una institución pública y una privada. Index de Enfermería (Internet ). 2017 (citado 9 agosto 2020); 26(3):142-146. Disponible en: http://scielo.isciii.es/scielo.php?script=sci_arttext&pid=S1132-12962017000200005 [ Links ]
39. Hernández-Valles J, Moreno-Monsiváis M, Interial-Guzmán M, Vázquez-Arreola L. Cuidado de enfermería perdido en pacientes con riesgo o con úlceras por presión. Revista Latino-Americana de Enfermagem (Internet ). 2016 (citado 9 agosto 2020); 24(2817). Disponible en:://doi.org/https 10.1590/1518-8345.1462.2817 [ Links ]
40. Germán Bes C, Orkaizagirre Gómara A, Huércanos Esparza I, Hueso Navarro F. ¿Provocan las enfermeras su propia invisibilidad? a propósito del caso de María. Index de Enfermería (Internet ). 2015 (citado 14 marzo 2020); 24(3):139-143. Disponible en:://dx.doi.org/http 10.4321/S1132-12962015000200005 [ Links ]
41. Lenis-Victoria C, Manrique-Abril F. Calidad del cuidado de enfermería percibida por pacientes hospitalizados. Aquichán (Internet ). 2015 (citado 9 agosto 2020); 15(3): 413-425. Disponible en: http://dx.doi.org/10.5294/aqui.2015.15.3.9 [ Links ]
42. Sanz M, Garrido L, Caro C. Factores que influyen en la satisfacción del paciente de diálisis con enfermería. Enfermería Nefrológica (Internet ). 2017 (citado 9 agosto 2020); 20(1): 66-75. Disponible en: http://scielo.isciii.es/scielo.php?script=sci_arttext&pid=S2254-28842017000100009&lng=es [ Links ]
43. Bautista L, Arias M, Carreño Z. Percepción de los familiares de pacientes críticos hospitalizados respecto a la comunicación y apoyo emocional. Revista Cuidarte (Internet ). 2016 (citado 9 agosto 2020); 7(2):1297-1309. Disponible: http://dx.doi.org/ 10.15649/cuidarte.v7i2.330 [ Links ]
How to cite: Melita-Rodríguez A, Jara-Concha P, Moreno-Monsiváis MG. Perception of hospitalized patients in medical surgical units on humanized nursing care. Enfermería: Cuidados Humanizados. 2021; 10(1): 89-105. Doi: https://doi.org/10.22235/ech.v10i1.2481
Contribution of the authors: a) Study conception and design, b) Data acquisition, c) Data analysis and interpretation, d) Writing of the manuscript, e) Critical review of the manuscript. AMP contributed in a, b, c, d; PJC contributed in a, e.; MGMM contributed in e.
Received: March 02, 2021; Accepted: May 20, 2021
 Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
