










Serviços Personalizados
Journal

Artigo
 texto em
texto em  Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
Links relacionados
Compartilhar

 Permalink
PermalinkEnfermería: Cuidados Humanizados
versão impressa ISSN 1688-8375versão On-line ISSN 2393-6606
Enfermería (Montevideo) vol.10 no.1 Montevideo jun. 2021 Epub 01-Jun-2021
https://doi.org/10.22235/ech.v10i1.2359
Original Articles
Clinical gait analysis in patient with poliomyelitis sequelae and total knee arthroplasty
1
 http://orcid.org/0000-0001-9748-6964
http://orcid.org/0000-0001-9748-6964
1
http://orcid.org/0000-0002-3654-7636
1
http://orcid.org/0000-0002-1858-2948
1
http://orcid.org/0000-0001-7399-9597
1 Universidad Católica del Uruguay ernesto.benitez@ucu.edu.uy
Keywords: post-poliomyelitis syndrome; arthroplasty replacement knee; gait analysis; biomechanical phenomena.
Palabras clave: síndrome pospoliomielitis; artroplastia de reemplazo de rodilla; análisis de marcha; fenómenos biomecánicos.
Palavras-chave: síndrome pós-poliomielite; artroplastia do joelho; análise de marcha; fenômenos biomecânicos.
Introduction
Poliomyelitis is a highly infectious disease caused by the poliovirus that predominantly affects children under age 5 and causes lasting effects in adulthood (1). It is characterized by a loss of motor neurons, which can cause flaccid paralysis, muscle loss and hyporeflexia (1-2). Although it mainly affects one or both lower extremities (LE) with varying severity and extent, it can also affect any motor unit with a predominance of the shoulder girdle and lower back (3). Poliovirus-affected cases dropped significantly globally, from 350,000 cases in 1988 to just 35 cases recorded in 2018 (4).
Since patients with flaccid paralysis of the lower extremity develop generalized hypotonia, abnormal alignments and laxity, in addition to the high frequency of affectation of the quadriceps muscle (indispensable during certain stages of gait), these patients are predisposed to knee joint pathologies at early ages (2). Despite the existence of therapeutic strategies to try to safeguard the joint early on, which improves alignment and increases stability, once painful osteoarthritis has been established in addition to ligamentous laxity (which occasionally triggers painful hyperextension of the knee joint), patients should be indicated a total knee arthroplasty (TKA; 1-2).
TKA in these patients is a technical challenge due to the aberrant anatomical characteristics of all the tissues that make up this joint (2). These alterations include joint and metaphyseal deformities, increased external tibial rotation, excessive valgus alignments, bone loss, narrowing of the femoral and tibial canal, genu-recurvatum, and ligamentous laxity (2). Additionally, these patients’ rotational profiles of the lower extremities in many cases predispose them to chronically subluxated or dislocated patellae (1-2). Despite the above, the findings support the use of TKA in patients with knees affected by polio sequelae (5). Post operatory functional results are like other types of TKA patients; however, implant revision rates are higher in post-polio patients (1-2, 5-7).
Quadriceps muscle strength seems to be an important prognostic factor for functional results and, when it is lower than antigravity, the use of constrained implants is recommended (8). In addition, the use of hinged implants is indicated in more severely affected patients with poor muscle strength that does not provide intrinsic stability, increasing the risk of recurrence of knee hyperextension and ligamentous laxity (9). The poor long-term results of conventional TKA use also support the use of constrained implants (7, 10-11). Tigani et al. do not justify previous criticism regarding the use of constrained implants, since modern rotary hinged designs more closely replicate the joint physiological kinematics, further reducing stress at the implant-bone interface (7).
In normal gait kinematics, the period where the foot is in contact with the ground is called support, represents 60 % of the gait cycle and is divided into 5 phases: initial contact, load response, medium support, terminal support, and pre-balancing. Each phase has a different duration and responds to a particular functional demand (3).
The first two phases (initial contact and load response) make up the task called weight acceptance, a challenging activity during gait that involves absorbing shock, initial stability when unloading weight and preservation of progression. During load response, a rapid bending of the knee joint of about 20 degrees occurs, which is the main mechanism of shock absorption. The quadriceps is activated eccentrically to control this movement, generating an extensor force moment, and slowing the rate of knee flexion (3).
The acceptance of weight is followed by the monopodal support, another challenging task involving the member under study being responsible for withstanding all body weight while the progression of the gait continues. This task is divided into the medium and terminal support phases, differentiated mainly by their progression mechanisms. At the beginning of the middle support, the knee joint begins to extend due largely to the plantar flexor-knee extensor coupling, a mechanism that corresponds to the eccentric action of the plantar flexors (mainly the soleus) during the first part of the middle support, which controls the progression of the ground reaction vector on the supporting foot. This resists the external flexor moment generated by the vector that passes behind the knee joint, creating an acceleration in the opposite direction, which assists in its correct extension.
Given the importance of walking in humans and due to alterations in gait patterns that occur in patients with polio sequelae, the study authors consider it appropriate to perform a characterization of the kinematics of gait in a patient with these characteristics. Through the analysis of the information provided by these studies, it is possible to generate strategies in the field of rehabilitation of these patients and improve the recovery of maximum functionality in daily life activities (12-13).
Case of study
76-year-old female patient with polio sequelae with a LE predominance, who developed the pathology at 5 months of life. In 2017, a right TKA was performed since her quality of life was affected by pain and deterioration in activities of daily life. In 2018, an evaluation was carried out in the University Movement and Gait Analysis Laboratory. The laboratory has a system of 8 2.2 Megapixel motion capture cameras (Vicon Motion System, Oxford, UK).
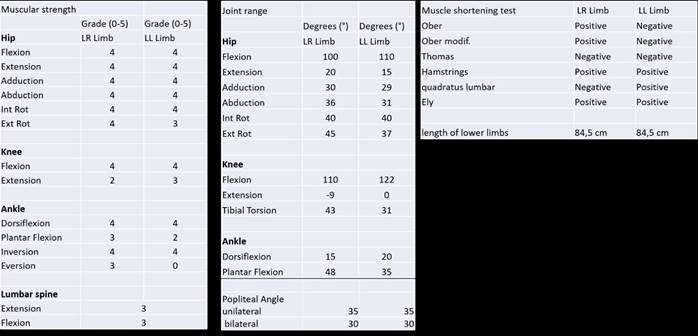
A physical examination was performed where the muscle strength and the joint range of LE were assessed using manual strength tests (14) and goniometry, respectively (15; Table 1).
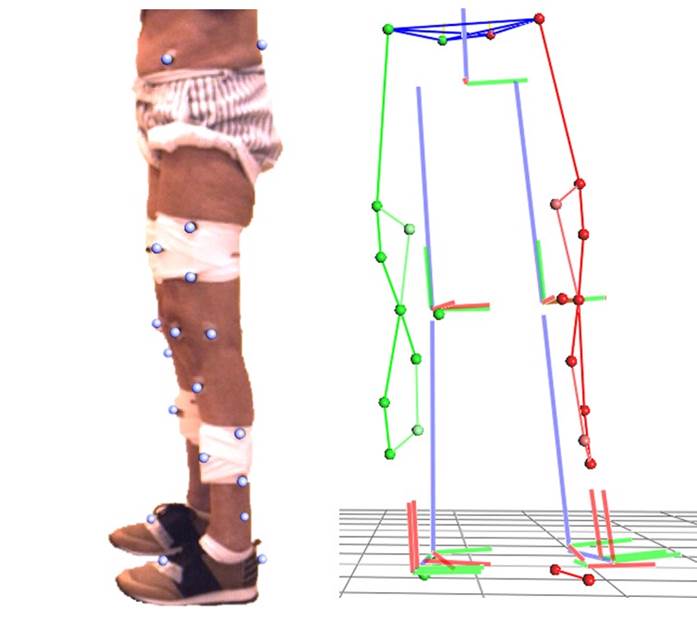
Reflective markers were placed on the pelvis, thighs, legs, and feet (Figure 1a), so that they were captured by the motion capture cameras and an instrumented study of the gait could be carried out. At the pelvic level, markers are placed in the anterior superior and posterior superior iliac spines. A marker is placed on the thigh on the external femoral condyle and 3 auxiliary non-anatomical markers (cluster) approximately in the distal third. A marker is placed on the leg in the anterior tuberosity of the tibia and, as on the thigh, 3 auxiliary non-anatomical markers are placed approximately in the distal third. A marker is placed on the head of the second metatarsal and on the calcaneus on the feet. Auxiliary markers are also placed on the kneecaps, and virtual markers are determined for internal femoral condyle, external and internal malleoli. This set of markers allows the calculation of two biomechanical models simultaneously. The most used is the Conventional Gait Model, which groups several similar models together, but with small variations (16-18). Despite being the best known, this model has some limitations that could compromise the quality of the data (19). Other biomechanical models use a greater number of markers to compensate for the limitations of the conventional model (20-21). These models allow to identify and follow different segments of the body independently (Figure 1b) and thus make a better estimate of the joint centers and axes dynamically through functional calibration (22-25).
Results
The results of the gait kinematics analysis show a consistent pattern, with an increase in the time of bilateral support. In relation to the spatiotemporal parameters (Table 2), a decrease can be seen in the length of the gait cycle, stride length, cadence and speed, the latter being approximately half of normal. Regarding the length of the stride, the patient presents an asymmetry, the right being 20 % shorter than the left (Table 2).
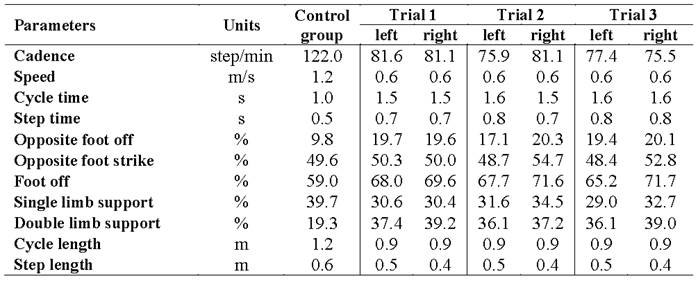
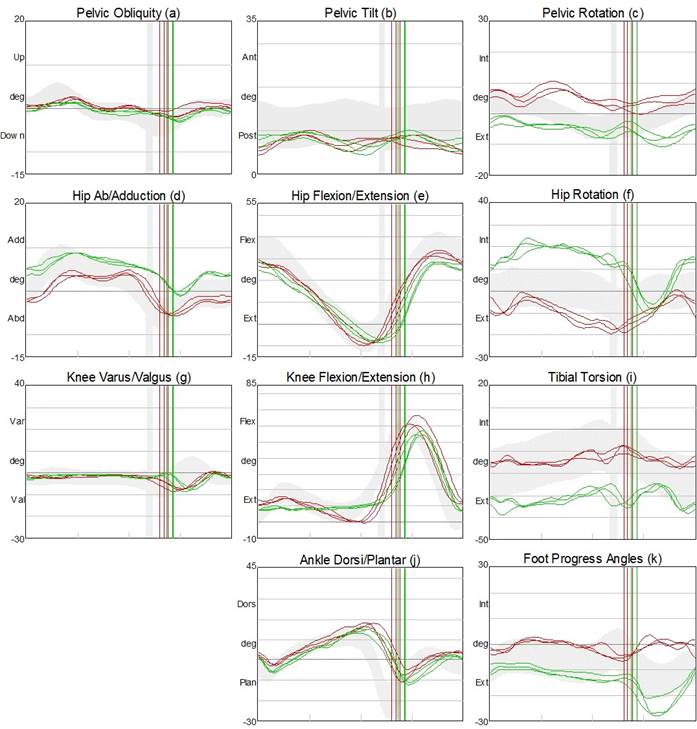
Table 3 shows the graphs of the kinematic analysis where the movement of each joint is dissociated in each anatomical plane. The rows show the angular kinematics of each joint (pelvis, hip, knee, and ankle, starting from the top) and the columns the planes of motion (frontal, sagittal and transverse plane, starting from the left).
The pelvis in the frontal plane (Table 3a) shows a restricted but symmetrical range of motion, while in the sagittal plane (Table 3b) a slight tendency towards retroversion can be seen with an inverted double bump pattern. The transverse plane presents a rotated pelvis (Table 3c), with the right hemipelvis delayed throughout the entire gait cycle.
The hip joints present an asymmetry in the frontal plane with the right more adduced than the left (Table 3d), while the flexion-extension range is preserved, but with a slight decrease in flexion at initial contact (Table 3e). In the transverse plane, an asymmetric pattern is recorded with the right hip internally rotated during support with a marked peak of external rotation during swing, while the left hip is slightly externally rotated throughout the gait cycle (Table 3f).
The left knee joint presents an adequate pattern and range of motion in the sagittal plane with a slight increase in flexion at initial contact (Table 3h). The right knee joint exhibits a sustained flexion of approximately 9 ° during most of the support, maintaining this flexion angle throughout initial contact, load response, medium support, and terminal support. On the transverse plane, an increased right-sided tibial torsion can be observed (Table 3i).
Finally, in relation to the angles of the ankle and foot joint, an adequate pattern of motion can be observed in the sagittal plane, but a slight decrease in the range of bilateral plantar flexion (Table 3j). On the transverse plane there is a slight asymmetry of the angles of progression of the feet (left inward), with a significant peak of external rotation of the right foot in the balancing phase (Table 3k).
Discussion
Given the scarcity of publications on gait analysis in this type of patients and with the surgical treatment performed, although orthotic treatment was found (26-27), some conjectures could be made about the possible causes of the different adaptations that were observed, so that the patient achieved a functional gait.
The reduced cycle length and speed during gait (Table 2) could be due to the expected lack of overall stability, which relates to weakness (Table 1) of the muscle groups necessary for a stable gait.
The found fact that the steps with the lower right limb are shorter (Table 2) could be due to the differences in the assessment of the muscle strength of the plantar flexor muscles of the left ankle (2/5) with respect to the right (3/5; Table 1). The patient reacts to the weakness of the plantar flexor muscles by reducing its demand, using the limitation of progression by taking shorter steps with the contralateral limb as a strategy (3).
Pelvic retroversion could be due to the weakness of the extensor muscles of the lumbar spine (verified during physical evaluation 3/5) due to the sequelae of poliomyelitis (3). This pelvic retroversion favors the activation of the iliac muscle during the oscillation phase and the contribution of flexor moment by the passive periarticular structures of the hip in the form of ligament resistance to the extension of said joint (28). In addition, pelvic retroversion positions the Tensor Fasciae Latae (TFL) Muscle in a length-to-stress ratio so that it is within the maximum active tension range and in a good passive tension position, maximally favoring this muscle´s function on the lower limb in the demands of abduction, internal rotation, and flexion. The function of this muscle is extremely important during the final oscillation phase for the gait strategy observed in this case (14). When retroversion occurs during the second half of the balancing phase, it may be due to a shortening of the hamstring musculature, a theory that was rejected since this shortening was not observed in the evaluation of the unilateral or bilateral popliteal angle (3; Table 1).
In addition to the above, a greater relative tension of the Gluteus Maximus (GM) with respect to the hip flexors could be contributing to the increased pelvic retroversion. This could be due to the double task that this muscle performs to generate indirect extension of the knee joint by pulling the femur posteriorly through its proximal insertion in said bone, and direct extension of the it through its insertion into the iliotibial band (3). These GM actions are necessary from the final oscillation phase to the middle of the middle support.
Patients who contracted polio during early childhood may suffer from a drop of the pelvis (Pelvic Drop) and therefore present a restriction of pelvic movement in the frontal plane (3). This may be because they can have one limb shorter than the other, generating a pelvic pre-positioning, and since the patient does not present such dysmetria (Table 1), the possibility that she has developed a retraction of the right iliotibial band as an adaptation to provide passive stability to the pelvis and the entire lower limb (3) gains strength.
The marked internal rotation (IR) of the right hip joint during the observed mid and final oscillation could be due to different factors. On the one hand, it could serve to promote the activation of the TFL so that its action as a hip abductor is transformed into hip flexion thanks to the rotation of the flexion-extension axis and in turn stabilizing the knee joint to the maximum extension available to the patient (9 ° flexion; Table 1). The TFL muscle, through its insertion into the tibia through the iliotibial band, acts as a knee extensor between 0-30° of flexion and as a knee flexor from 30 ° of flexion onwards (29). Remembering that during the phases mentioned above, under normal circumstances, the quadriceps should oversee providing this double function of hip flexor (collaborator in hip flexion) through the rectus anterior and that the vastus should be activated during the oscillation phase and to ensure extension of the knee joint, as well as to prepare the knee for the high functional demands associated with the abrupt drop in body weight during weight acceptance/load response (3). The patient presents a lower right quadriceps strength value than the antigravity one (Table 1) and is forced to develop alternative strategies for functional gait.
On the other hand, the internal rotation of the hip joint predisposes the femoral condyles during the initial contact in such a way that it manages to rotate the natural flexion-extension axis of the knee joint, preventing the high energy produced in the subsequent phase of the response to the load from faltering in knee flexion (30). Thus, absorbing it in the form of a forced yawn/varus of the lateral compartment of the prosthesis, given the weakness of the quadriceps muscle that makes it incapable of eccentrically slowing down the rapid knee flexion that occurs as one of the several mechanisms of absorption of impact when contact the lower limb with the ground abruptly.
Finally, internal rotation of the hip joint during the entire stance could try to compensate for the notable external tibial torsion that the patient exhibits (Table 1) to favor the activity of the weakened triceps suralis (3/5) to retain the advancement of the tibia relative to the advancement of the femur.
From the final swing to the middle of the midstance, it is the GM activity that provides the extension force of the hip joint and the extension stability of the knee joint through the insertion of the knee joint. iliotibial band over the anterolateral border of the tibia, as mentioned above.
During the initial balancing, a significant external rotation movement of the right hip joint occurs. This rotation could be due to the sudden release of the lower limb, which was in marked internal rotation during middle and terminal support, and which produces a release of elastic energy at the end of the ground contact restriction. Another hypothesis for the aforementioned external rotation is that the flexion of the hip joint and the knee joint necessary in the initial swing, are produced mainly by the Sartorius muscle, which in addition to being a flexor of the hip joint and of the knee joint, is the hip external rotator.
The activity of the Psoas as a flexor of the hip joint in the initial oscillation phase could generate an external rotation of the hip since this is its secondary function. The activity of this muscle could be favored by the distance from its origin in the lumbar region dictated by the previously mentioned pelvic retroversion position (14).
The difference in the abduction and adduction of both hip joints could be due to the rotation of the pelvis in the transverse plane that transforms part of the flexion and extension of the hip into abduction and adduction of the hip.
The quasi-invariant flexion position of the knee joint of 9 ° during the initial contact, load response, the middle and terminal support, corresponds to the articular evaluation of the passive range of motion of the knee, the limit of which is - 9 °. It can also be observed that the sagittal view of the postsurgical x-ray (Figure 2) shows a prosthesis in full extension while the position of the joint does not correspond to it but does correspond to a 9 ° knee flexion. This could be due to the technical challenge posed by TKA in patients with polio sequelae in whom, as previously mentioned, joint and metaphyseal deformities, increased external tibial rotation, excessive valgus, poor bone quality, genu-recurvatum and ligament laxity, characteristics that can alter the intrinsic processes of the surgery, such as the making of the canals for the tibial and femoral stems (1-2). In addition, the proper placement of these stems and the setting of the cement, which, being osteopenic bones, can easily generate unwanted alterations in the alignment of the prosthetic element (8).

Among the limitations of this study is the fact that it only analyzes the results of gait kinematics, since there is no other equipment such as force platforms or electromyography, which are occasionally presented in this type of study. The analysis of the kinetics (moments of force and strength of the joints), or the record of muscular electrical activity, could yield other information for an even deeper and more exhaustive analysis (31-32). Pre-TKA gait characterizations are lacking, so it cannot be confirmed whether the variations with respect to normal gait observed in this study and the gait strategy described above were used by the patient prior to the surgery, or if it was acquired in the rehabilitation and readaptation stage. Weakness and delayed activation of the quadriceps muscle has been identified as the major cause of functional limitations after TKA (33-34).
It is concluded that since quadriceps muscle weakness (2/5) is a sequela of poliomyelitis (1), the patient used an extensor thrust strategy (3), in which the GM generates an indirect extension of the knee joint through its insertion in the femur and in turn blocks it in full extension or hyperextension (common in patients with polio sequelae) through the distal insertion of the iliotibial band in the tibia which prevents the claudication of this joint in the load response phase.
The authors of this study share the idea that the extensor thrust occurs but add and highlight the possible importance of the TFL muscle in the phases of the gait in which an extension or maintenance of the knee is required in the 9 ° flex. As the hip joint is in flexion and the GM is not capable of producing its triple function as an extensor of the hip, an indirect extensor of the knee joint and keeping the latter locked in extension, the TFL is in charge of preparing the limb during the mid- and final oscillation so that the initial contact occurs to the maximum extent available to the right knee joint. This is where the GM can undertake its task.
With the information gathered in both the physical assessment and the characterization of gait kinematics, it is proposed that in the face of the quadriceps strength deficit of the right lower limb (irreversible due to the sequelae of post-polio syndrome), one could think about the strengthening of the muscles used to supplement the abolished functions, such as the flexors and rotators of the hip joint, the TFL and the sartorius, and extensors of the same joint as well as the lumbopelvic stabilizing muscles, the GM and medius. In turn, the TFL and the GM collaborate at the distal level with the maintenance of the extension of the knee joint during load response, so it is considered important to focus therapeutic planning towards the mentioned muscle groups.
REFERENCES
1. Patterson BM, Insall JN. Surgical management of gonarthrosis patients with poliomyelitis. J Arthroplasty. 1992; 7(Suppl.): 419-426. [ Links ]
2. Giori NJ, Lewallen DG. Total knee arthroplasty in limbs affected by poliomyelitis. J Bone Joint Surg. 2002; 84(7): 1157-1161. [ Links ]
3. Perry J, Burnfield JM. Gait Analysis: Normal and Pathological Function. 2ª ed. New Jersey: Slack Incorporated; 2010. [ Links ]
4. Organización Mundial de la Salud. Notificados a la OMS el 1 de marzo de 2019. Poliomielitis (Internet). Ginebra: OMS; 2020 (consultado 24 oct 2020). Disponible en: https://www.who.int/es/news-room/fact-sheets/detail/poliomielitis. [ Links ]
5. Rahman J, Hanna SA, Kayani B, Miles J, Pollock RC, Skinner JA, et al. Custom rotating hinge total knee arthroplasty in patients with poliomyelitis affected limbs. Int Orthop. 2015; 39(5): 833-838. [ Links ]
6. Jordan L, Kligman M, Sculco TP. Total knee arthroplasty in patients with poliomyelitis. J Arthroplasty 2007; 22(4): 543-548. [ Links ]
7. Tigani D, Fosco M, Amendola L, Boriani L. Total knee arthroplasty in patients with poliomyelitis. Knee. 2009; 16(6): 501-506. [ Links ]
8. Prasad A, Donovan R, Ramachandran M, Dawson-Bowling S, Milington S, Bhumbra Rej, et al. Outcome of total knee arthroplasty in patients with poliomyelitis: A systematic review. EFORT Open Rev. 2018; 3(6): 358-362. [ Links ]
9. Dauwe J, Vandenneucker H. Indications for primary rotating-hinge total knee arthroplasty. Is there consensus? Acta Orthop Belg. 2018; 84(3): 245-250. [ Links ]
10. Partezani C, Nogueira P, Maftoum C, Gomes R, Kawamura M, Luis G. Knee arthroplasty with rotating -hinge implant: an option for complex primary cases and revisions. Rev Bras Ortop. 2018: 53(2); 151-157. [ Links ]
11. Yang JH, Yoon JR, Oh CH, Kim TS. Primary total knee arthroplasty using rotating-hinge prosthesis in severely affected knees. Knee Surg Sports Traumatol Arthrosc. 2012: 20(3); 517-523. [ Links ]
12. Kirschberg J, Goralski S, Layher F, Sander K, Matziolis G. Normalized gait analysis parameters are closely related to patient-reported outcome measures after total knee arthroplasty. Arch Orthop Trauma Surg. 2018; 138(5): 711-717. [ Links ]
13. Dominguez F, Igual C, Silvestre A, Roig S, Blasco JM. Effects of balance and proprioceptive training on total hip and Knee replacement rehabilitation: A systematic review and meta-analysis. Gait Posture. 2018; 62: 68-74. [ Links ]
14. Kendall FP, McCreary EK. Kendall’s músculos: Pruebas funcionales, postura y dolor. 5a. ed. Madrid: Marbán; 2007. [ Links ]
15. Taboadela C. Goniometría: una herramienta para la evaluación de las discapacidades laborales. 1a ed. Buenos Aires: Asociart ART; 2007. [ Links ]
16. Davis RB, Ounpuu S, Tyburski D GJ. A gait analysis data collection and reduction technique. Hum Mov Sci. 1991; 10: 575-587. [ Links ]
17. Kadaba MP, Ramakrishnan HK . Measurement of Lower Extremity Kinematics During Level Walking. J Orthop Res. 1990; 8: 383-892. [ Links ]
18. McGinley JL, Baker R, Wolfe R, Morris ME. The reliability of three-dimensional kinematic gait measurements: A systematic review. Gait Posture. 2009; 29(3): 360-369. [ Links ]
19. Baker R. Gait analysis methods in rehabilitation. J Neuroeng Rehabil. 2006; 3: 1-10. [ Links ]
20. Cappozzo A, Catani F, Della Croce AL. Position and orientation in space of bones during movement: anatomical frame definition and determination. Clin Biomech. 1995; 10(4): 171-178. [ Links ]
21. Collins TD, Ghoussayni SN, Ewins DJ, Kent JA. A six degrees-of-freedom marker set for gait analysis: Repeatability and comparison with a modified Helen Hayes set. Gait Posture. 2009; 30(2): 173-180. [ Links ]
22. Schwartz MH, Rozumalski A. A new method for estimating joint parameters from motion data. J Biomech. 2005 Jan; 38(1): 107-116. [ Links ]
23. Ehrig RM, Taylor WR, Duda GN, Heller MO. A survey of formal methods for determining the centre of rotation of ball joints. J Biomech (Internet). 2006; 39(15): 2798-2809. Disponible en: http://www.ncbi.nlm.nih.gov/pubmed/16293257 [ Links ]
24. Camomilla V, Cereatti A, Vannozzi G, Cappozzo A. An optimized protocol for hip joint centre determination using the functional method. J Biomech. 2006; 39(6): 1096-1106. [ Links ]
25. Ehrig RM, Taylor WR, Duda GN, Heller MO. A survey of formal methods for determining functional joint axes. J Biomech (Internet). 2007; 40(10): 2150-2157. Disponible en: http://www.ncbi.nlm.nih.gov/pubmed/17169365 [ Links ]
26. Portnoy S, Schwartz I. Gait characteristics of post-poliomyelitis patients: Standardization of quantitative data reporting. Ann Phys Rehabil Med. 2013; 56(7-8): 527-541. [ Links ]
27. Brogardh C, Flansbjer VB, Lexell J. Determinants of falls and fear of falling in ambulatory persons with late effects of polio. PM R. 2017; 9(5): 455-463. [ Links ]
28. Simonsen E, Cappelen K, Skorini R, Larsen P, Alkjær T, Dyhre-Poulsen P. Explanations pertaining to the hip joint flexor moment during the stance phase of human walking. J Appl Biomech. 2012; 28(5): 542-550. [ Links ]
29. Trammell AP, Nahian A, Pilson H. Anatomy, Bony Pelvis and Lower Limb, Tensor Fasciae Latae Muscle (citado May 7 2020). En: StatPearls (Internet). Disponible en: Disponible en: https://www.ncbi.nlm.nih.gov/books/NBK499870/ [ Links ]
30. Kapandji A. Fisiología articular: Miembro inferior. Tomo 2. 1ª ed. Madrid: Panamericana; 2012. [ Links ]
31. Elkarif V, Kandel L, Rand D, Schwartz I, Greenberg A, Portnoy S. Muscle activity while ambulating on stairs and slopes: A comparison between individuals scheduled and not scheduled for knee arthroplasty and healthy controls. Musculoskeletal Science and Practice. 2021; 52: 102346. [ Links ]
32. Bianchi N, Facchini A, Mondanelli N, Sacchetti F, Ghezzi R, Gesi M, Capanna R, Giannotti S. Medial pivot vs posterior stabilized total knee arthroplasty designs: a gait analysis study. Med Glas (Zenica). 2021 Feb 1; 18(1): 252-259. [ Links ]
33. Yoshida Y, Mizner RL, Snyder-Mackler L. Association between long-term quadriceps weakness and early walking muscle co-contraction after total knee arthroplasty. Knee. 2013; 20(6): 426-431. [ Links ]
34. Marmon AR, Snyder- Mackler L. Activation deficits do not limit quadriceps strength training gains in patients after total knee arthroplasty. Int J Sports Phys Ther. 2014; 9(3): 329-337. [ Links ]
How to cite: López D, Peña N, Benítez E, Samudio S, Vecino P, Benvenutto E. Clinical gait analysis in patient with poliomyelitis sequelae and total knee arthroplasty. Enfermería: Cuidados Humanizados. 2021; 10(1): 75-88. Doi: https://doi.org/10.22235/ech.v10i1.2359
Contribution of the authors: a) Study conception and design, b) Data acquisition, c) Data analysis and interpretation, d) Writing of the manuscript, e) Critical review of the manuscript. DL contributed in a, b, c, d, e; NP contributed in a, b, c, d, e.; EB contributed in a, d, e; SS contributed in a, b, c; PV contributed in a, b, c; EB contributed in a, b, c.
Received: December 23, 2020; Accepted: May 21, 2021
 Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
