










Serviços Personalizados
Journal

Artigo
 texto em
texto em  Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
Links relacionados
Compartilhar

 Permalink
PermalinkEnfermería: Cuidados Humanizados
versão impressa ISSN 1688-8375versão On-line ISSN 2393-6606
Enfermería (Montevideo) vol.9 no.2 Montevideo dez. 2020 Epub 01-Dez-2020
https://doi.org/10.22235/ech.v9i2.2208
Original articles
Interrelations in the care with medicinal plants - “it comes from the cradle”
1
 http://orcid.org/0000-0002-3666-0874
http://orcid.org/0000-0002-3666-0874
1
http://orcid.org/0000-0002-5592-365X
1
http://orcid.org/0000-0003-3649-6557
1 Facultade de Enfermagem da Universidade Federal de Pelotas. Brasil
2 Embrapa Clima Temperado. Brasil
This study aims at describing the interrelations of people who carry out the health care with medicinal plants. It is a qualitative, exploratory, descriptive and ethnobotany research which used the Systemic Theory as theoretical reference. Six people were interviewed as reference in the health care with medicinal plants in the first semester of 2018. The data were organized through the WebQDA qualitative data analysis program and it was carried out the Bardin content analysis. Results related to the origin of knowledge about care with medicinal plants are presented and also about the social interrelation as a form of transmission of knowledge. Knowledge is acquired in the family, through courses or, it is understood as a gift. The informers transmit their knowledge in different social contexts according to the disposition of their interrelations. It is concluded that different individual, social and environmental interrelations originate different forms of health care with medicinal plants and their knowledge associated.
Key words: Medicinal Plants; Community Networks; Medicine Traditional
O trabalho teve como objetivo descrever as inter-relações de pessoas que realizam o cuidado em saúde com plantas medicinais. Trata-se de uma pesquisa qualitativa, exploratória, descritiva e etnobotânica que utilizou a Teoria Sistêmica como referencial teórico. Foram entrevistadas seis pessoas referência no cuidado em saúde com plantas medicinais no primeiro semestre de 2018. Os dados foram organizados pelo programa WebQDA qualitative data analysis e foi realizada a análise de conteúdo de Bardin. São apresentados resultados relacionados a origem do saber sobre o cuidado com plantas medicinais e também acerca da inter-relação social como forma de transmissão de conhecimento. O saber é adquirido na família, por cursos ou, é entendido como um dom. Os informantes transmitem seus saberes em diferentes contextos sociais conforme a disposição de suas inter-relações. Conclui-se que diferentes inter-relações individual, social e ambiental originam diferentes formas de cuidado em saúde com plantas medicinais e seus saberes associados.
Palavras chave: Plantas Medicinais; Redes Comunitárias; Medicina Tradicional
Este trabajo tuvo como objetivo describir las interrelaciones de personas que realizan el cuidado en salud con plantas medicinales. Se trata de una investigación cualitativa, exploratoria, descriptiva y etnobotánica que utilizó la Teoría Sistémica como referencial teórico. Fueron entrevistadas seis personas referencia en el cuidado en salud con plantas medicinales en el primer semestre de 2018. Las informaciones fueron organizadas por el programa WebQDA qualitative data analysis y fue realizado el análisis de contenido de Bardin. Son presentados resultados relacionados al origen del conocimiento sobre el cuidado con plantas medicinales y también acerca de la interrelación social como forma de transmisión de conocimiento. El conocimiento es adquirido en la familia, por cursos o es entendido como un don. Los informantes transmiten sus conocimientos en diferentes contextos sociales conforme la disposición de sus interrelaciones. Se concluye que diferentes interrelaciones individual, social y ambiental originan diferentes formas de cuidado en salud con plantas medicinales y sus conocimientos asociados.
Palabras clave: Plantas Medicinales; Redes Comunitarias; Medicina Tradicional
Introduction
Medicinal plants may represent an expanded form of producing health since this structure brings together symbolic, religious, and cultural aspects. In addition to that, they demonstrably contribute to the prevention and cure of certain diseases. Thus, medicinal plants' use is based on popular knowledge - constituted by experiencing reality and commonly spread in a community or group - and on scientific knowledge, characterized by rational and analytical thought, which is habitually more esteemed than popular knowledge 1. The rapprochement between scientific and popular knowledge is necessary so that medicinal plants use no longer stay on the margins of the scientificity consolidated in the biomedical model. Both kinds of knowledge are complemented when the aim is comprehensive care in health promotion 2.
In health care with medicinal plants, some individuals stand out using this therapy. Although it is not an officially recognized profession, erveiros and ervateiros (herbalists, in Brazil) commercialize medicinal plants and establish interrelationships during this activity, playing a primary social role in maintaining health care based on popular knowledge 3. Besides the erveiros, some practice health care with medicinal plants for themselves and to prescribe this therapy.
In the systemic view, the human organism is considered a universe constituted by diverse interrelations between cells, tissues, organs, and systems. Its existence derives from the relationship of these parts, that is, from individual (biological) interrelationships. Similarly, each person is part of one (or more than one) group that can only function through their social interrelations. The ecological interrelation is attributed to the scope of nature or the environment 1.
However, there is a concern with the rational and safe use of medicinal plants in health care 4. There is also apprehension regarding the possibility of this knowledge disappear since it is not widely documented 5. Thus, strategies for rescuing and preserving it regarding the interrelations with the environment are beneficial initiatives for the maintenance and conservation of nature, as well as the knowledge associated with it 4. The use of medicinal plants in health care still faces obstacles regarding the interaction between the scientific and popular methods, challenging comprehensive care that considers the person as a whole, including their interrelations 6.
The approximation between popular and scientific knowledge can contribute to accomplishing the desired comprehensive care, considering that dialogue and approximation are necessary to consider the context of the other. In contemporary times, reason prevails over intuitive wisdom and science over religion. This thought reflects politically and socially the predominance of reason and science, with this knowledge being the only one considered as truth. Nevertheless, a systemic view of life corresponds to the possibility of expanding the perspective on health, diseases, and cure - a holistic approach 1.
In this research, according to the adopted theoretical framework, health is understood by the balance of three levels: individual, social and ecological 1, which may constitute a subjectivity in the interpretation of a person's care demands according to the interrelations established in each level. Thus, this paper aims to describe the interrelations of people who perform health care with medicinal plants.
Methodology
This is a qualitative, exploratory, descriptive, and ethnobotanical study based on the Systemic Theory by Fritjof Capra 1. The research was conducted between January and April 2018, with six people who stand out in health care with medicinal plants.
Two erveiros (a man and a woman), a holistic therapist, a herbal therapist, a benzedeira (a healer who treats people with prayers in Brazil), and a pharmacist were informants in the research Espinheira-santa (Maytenus ilicifolia): o saber de erveiros e feirantes em Pelotas 7. The exclusion criteria were having difficulties in verbal communication and being under 18 years old.
Convenience sampling came from respondents in the research database. Participants whose herb stalls had been active for two generations were the 'starting point' and were invited to participate in the study. Each interviewee was asked to indicate other people who performed health care with medicinal plants. This methodological technique is called network of relationships 8 or 'snowball sampling' (bola de neve, in Portuguese) 9-10. The number of participants 6 was defined when the interviewees suggested people who were already part of the group, and there were no other people to indicate.
To be part of the research, individuals should meet three selection criteria: being indicated by other informants who worked with medicinal plants, as mentioned before, in addition to allowing both the use of a voice recorder and the presentation and dissemination of results in academic and scientific circles.
To gather the required data, an individualized semi-structured interview was recorded with an average duration of 50 minutes. The simple observation did not follow a preset script. The reports were registered in a 34-page field log typed in the Windows' software Word. The participants agreed to participate in the research through the Free and Clarified Consent Term, and the interview happened in a place indicated by themselves. The majority chose the place where they worked, except for one informant who chose the researcher's workplace.
During the interview, informants were required to speak about health care with medicinal plants. They were specifically asked about: when do they use and prescript medicinal plants, why did they choose to work with it, with whom did they learn, if they teach others to work with those plants, and what are the advantages and disadvantages of working with medicinal plants. Finally, they were requested to talk about the origin of the medicinal plants they use and whether they were harvested from nature or cultivated.
The statements were transcribed using Windows' software Word, resulting in 111 pages. The content analysis method was used in the research, chronologically described in three main stages: pre-analysis, material exploration, and data treatment 11.
The pre-analysis consisted of skimming the material and transcribing the interviews, making it possible to get familiar with the data.
The material exploration began with the interview's structural deciphering, which sought understanding within the interviewees' statements. The online software called WebQDA qualitative data analysis was used to organize the information in each transcript, with the following steps being taken: a) The interviews thematic analysis: excerpts, phrases, words that referred to a possible topic were highlighted, centered on the informants' statements; b) Definition of the central theme associated characteristics: for each theme identified, a description of the author's interpretation was made based on the adopted framework, composing a code; c) Sequential analysis: the interview was organized in sequences associated with the codes; d) Oppositions analysis: for contradictions, whether in the same interview or among informants, the same code was established in order to contribute to the analysis of the text; e) Enunciation analysis: it was the time to deepen in the informants' statements in which the testimonies were revisited for an in-depth analysis toward the search for meanings and expressions.
Following the data's organization and codification, its treatment was carried out (the last step of the content analysis method), which, although described separately, co-occurred with the previous steps. However, the elements were classified at this stage, revealing the interpretations related to the adopted framework.
The interviews were conducted after obtaining the concurring opinion of the Research Ethics Committee of the College of Medicine from the Federal University of Pelotas (RS, Brazil). This research was guided by Resolution No. 466/12 12.
Results
This research informants have their knowledge, as well as their practices of healing methods in health with medicinal plants, based on popular knowledge, which, in turn, is developed from experimentation and observation of nature. Their social interrelations allow them to continue handing on their knowledge. The three levels of interrelations (individual, social, and environmental) form a network of people who perform popular health care with plants (Figure 1).
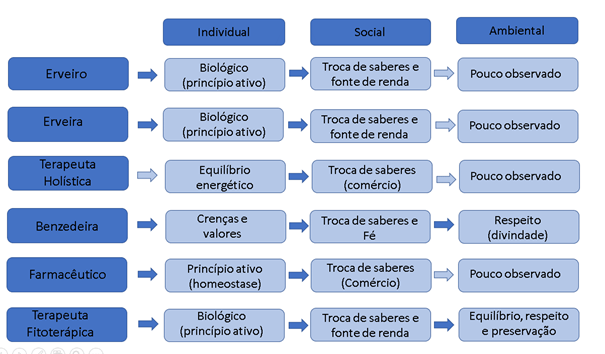
Figure 1: Informants' network of relations in the research Interrelations of people who perform popular health care with medicinal plants, 2018.
For both the erveiro and erveira (the male and female herbalists, respectively), the interrelations were observed mainly at the individual and social levels. The interrelations in the individual (or biological) level occur by consuming the medicinal plant to use the effect of the plant's active ingredient. In turn, the social level was observed when there was knowledge exchange during medicinal plants' commercial activity and in places where they share their knowledge.
The holistic therapist establishes the individual level of interrelation to develop an energetic balance through energy exchange with the plants. However, the social level interrelation occurs more intensely when her medicinal plant knowledge leads to a trade that is her income source.
The individual level of interrelation between the plants and the benzedeira (the healer) occurs when she uses them to communicate with the spiritual world. The social level relates to the bonds formed during the beliefs sharing between the benzedeira and the people who seek her. Another aspect that characterizes the social level is her authority for standing out in health care using plants during her blessings. For this interlocutor, the environment is a deity respectfully treated by her, demonstrating the environmental interrelation.
The pharmacist's individual interrelation with the plants is observed in its consumption as an alternative to achieve chemical balance in the organism's homeostasis. His social interrelation occurs through knowledge transmission as an income source and the bonds established in his patients' care.
The three levels of interrelation with medicinal plants could be observed in the phytotherapist. The individual interrelation occurs when she uses the plant to obtain the benefits of its active ingredient. This informant stands out in her community due to her knowledge of medicinal plants. For this reason, several people come to her seeking treatment for their illnesses, strengthening the social level. The environmental interrelation is observed from her outlook on nature preservation. For example, she allows the spontaneously born plants from her backyard to develop because she understands that they are part of the whole and are necessary to the ecological balance.
The erveiros, the holistic therapist, and the pharmacist did not have their backyards visited, and it is not possible to know their environmental interrelations. Nevertheless, it does not mean that this interrelation level does not exist. It was just impossible to observe in this study.
Regarding the interrelations that led them to learn health care with medicinal plants, two interlocutors reported that they were born with something special or divine permission to perform this kind of cure. Both informants reported that this 'gift' was followed by personal confusion and, regarding the holistic therapist, conflicts in the social relationship with her family.
I carry this with me since I was born. That had been improving (...) It flourished (...) I am sure this is from other lives (Benzedeira).
I started to practice it very early, practically in my adolescence. (...) I was involved with energetical issues from an early age, although my family did not understand me as a child. My family was Catholic; my first path was to find another religion that would help me understand and stabilize that. Over time, I distanced myself from religion and started looking for other kinds of knowledge; I took some courses here and there. (Holistic therapist).
The phytotherapist declared her intuition as her knowledge source. The informant described that, at a specific moment, she intuitively practiced health care with medicinal plants. It was not related to any training received from someone or any material source.
I went after that because I already had an intuition, I liked it (...) I went to study this erysipelas, and how it arouses (...). I searched plants that fit that pathology. I checked 62 plants from all over Brazil. But I wanted a plant that could be found here. Two plants fit: the active ingredient of one is for fever while the other one for infection. One of those plants I had at home, so I thought: I will use this one first, and, if it is necessary, I will use the other. Then I discovered the elderberry (The phytotherapist).
The informants also referred to the family core as the origin of health care knowledge with medicinal plants. Furthermore, even today, the informants request the help of the elders. The erveiro (the male herbalist) affirmed that he learned about health care with medicinal plants from his father in the herb stand. On the other hand, the erveira (the female herbalist) referred to her mother as her knowledge source.
I started learning at the age of six. And I started working (at the herb stall with the father) when I was about ten, receiving clients there, talking (...) It comes from my childhood (The erveiro).
I started learning about plants in my childhood. As I use to say: since my mother's womb. Because she already worked with teas. Then, as a child, my father began to take me into the woods, to harvest macela (Achyrocline satureioides), to harvest the carqueja (Baccharis trimera), these common teas. So, as I grew up, I enjoyed the same thing as them because my mother loves working with teas (The erveira).
On the other hand, the origin of the pharmacist's knowledge of health care with the medicinal plants did not come from the family core. The informant approached the topic when he started working after graduation.
I got a job as an over-the-counter attendant at a compounding pharmacy specialized in complementary and alternative medicine such as phytotherapy. As soon as I started there, I took the book and kept consuming that knowledge. (...) And there I came across with phytotherapy. Until then, I did not even know what a mint (Mentha) was for. I did not know the use of anything, but I began to get a taste for the thing (the pharmacist).
Phytotherapist's motivation was the need to place herself in the job market. Due to unemployment, the informant dedicated herself to obtain knowledge regarding the use of medicinal plants.
I was unemployed at that time, that is why I took the course (...) I have not stopped until today, I became autonomous, I started to open up to things, took courses, and started to evolve and learn. I was always involved in every lecture, everything there was about plants, and then I started to read a lot. (The phytotherapist).
Regarding their knowledge improvement, the informants reported conducting research in books and on the Internet. They also mentioned they participated in congresses, training courses, and postgraduate courses.
I got the knowledge (...) from customers, books, and the Internet. But it is good to always look for a good reference. If what I see does not indicate the reference, I do not trust it. So, I prefer to look it up in several sources (The erveiro).
I started to study at home, I bought books (...) I researched about it on the Internet (...) I took this Chinese herbal medicine course (...) I went to Mato Grosso for a conference on homeopathy (.. .) One person saying one thing, the other person saying another, you learn a lot in those conversation circles. I am not saying that you do not learn at a congress, but a lot is learned in those conversation circles on the street (The phytotherapist).
I had just graduated, and I thought I should take a postgraduate course (...). I took courses in Chinese medicine, Chinese herbal medicine, took short courses with other professionals, and had a postgraduate degree in western herbal medicine. And it also came from personal study (The pharmacist).
The informants in this research commented on how the knowledge is shared at home (with the family). As reported, it may be transmitted from mother to daughter, from the oldest to the youngest, as well as from the youngest to the oldest, as occurs with the pharmacist.
For my daughter to understand, I have to teach, show the way for her to learn. We talk a lot. I explain to her a lot of things (The benzedeira).
It is important to share this knowledge, for sure. Now, I will have to transmit this knowledge to my children (The erveira).
I teach little by little. My mother loves it, and she uses it a lot, my grandmother, too. I recently made her a recipe because she fell and broke her femur, and she loved the medicine, those grandmother things (...). My brothers are more resistant to it (...), my father is a little resistant, too (The pharmacist).
Although oral transmission is usual in the family, the interviewees reported some difficulties in passing on this knowledge. According to them, it would be related to the youngsters' lack of interest or the absence of a person close to the informant.
My son is not open up to this area. So, in fact, I transmit my knowledge to my students (Holistic therapist).
I still do not have anyone to share this knowledge (...) Sometimes, patients come here and say: 'my father, my grandfather, were homeopaths.' Then I ask: where is this knowledge? Did you not get it? No. But then you notice that that person has everything it needs to be a disciple. And she did not listen because she does not have the patience to listen to the oldest people, which is happening now. People who listen are rare. Why did you not learn the benzedura (healing through prayer) with your grandmother? People are not interested, young people much less. This knowledge is being lost. I have a patient whose mother reads people's eyes. She sees the person through the eyes and does not know how to read or write. She is a person from the colony. Another patient, whose father was a homeopath, brought me his book with several notes. But she did not get any of that knowledge, nothing. Her children brought up seeing this, but they did not learn it either. It is getting lost. It is rare to see someone talking to me about it here (The phytotherapist).
There is no one today (...) I have this project of mine to create a page (on the Internet) to put more and more content for people who research and believe because publishing on the Internet is even easy (The erveiro).
This study's informants reported that the dissemination of knowledge related to medicinal plants' use occurs when transmitting it to students, clients, teachers, or colleagues.
Sometimes people ask me, even teachers and colleagues: 'what would be a good tea for this? And what about a good tea for that?' It is good to help. When I see that someone is having problems, I give some tips. I have already passed on much knowledge that way (The erveiro).
I share my knowledge with my customers (The erveira).
Today, I try to pass on to people all my knowledge (The benzedeira).
I had experience with quilombos (communities of descendants of slaves that scaped from their masters). I was invited to speak about my knowledge at school. They brought theirs, and we aggregated it. I even got a very beautiful book from them (The phytotherapist).
For the pharmacist, much knowledge has been lost regarding the use of medicinal plants. The interlocutor states that this gap is due to oral tradition.
This kind of knowledge has lost much strength in Brazil. First, because the herbal medicine tradition was an oral tradition. The indigenous and black people did not write any of this. It got lost over time, and it became impossible to create a framework, an encyclopedia with this knowledge. What remains is an oral tradition in which few people possess the knowledge. This has always been the case since 500 years ago. Much of our culture, our knowledge of Brazilian plants, is gone. We will have to rediscover all of this. The books started to be made in the 1800s. There is a 300-year gap on the subject. This knowledge has been lost. We have this problem of limited knowledge (The pharmacist).
Also, to disseminate knowledge about health care with medicinal plants, the pharmacist has already offered a phytotherapy course, the benzedeira has already taught a healer training course using plants, and the holistic therapist has already organized courses and taught classes on the subject.
I teach complementary practices in several places in the country, but mainly in São Paulo, where I live. But basically, the courses I teach are about phytotherapy (The pharmacist).
One day I sat down and said: I am not going to take this to the grave, I do not want to. I have to pass it on. Then my sister said: 'let's organize a course, I will help you, and you will teach it.' I made a coursebook (...). Besides, I teach the prayers; I make a person pray for the other (...). In addition to learning, the students will have the coursebook's prayers to recheck it every time they need to. (The benzedeira).
I teach my students (...). My students are doctors, psychologists, nurses (...). I taught many courses. For example, there was a job where I taught these courses on rituals using herbs (...). I love it. I have the gift of teaching (The holistic therapist).
Discussion
The impossibility of visiting the participants' backyards may be related to the interlocutors' way of protecting the environment. A similar attitude was observed in the study 13: the informants did not reveal certain knowledge of traditional medicine, as it would cause the plant to lose its healing properties. According to the Systemic Theory, this protective behavior may be interpreted as a weak social interrelation, which hinders knowledge transmission. On the other hand, it might be understood as a powerful environmental interrelation of protection and maintenance.
For the informants, what grants them authority, or at least authorize them to carry out the healing process, is something special that they brought from another life or another (spiritual) world. This 'gift' was taking shape, being perfected by the social interrelations experienced by each interlocutor.
In this sense, health care was historically practiced by healers guided by popular wisdom and spirituality. They considered the diseases to be disorders in the person as a whole, involving his body, mind, self-image, and interrelation with the physical and social environment. The healers adopted different therapeutic techniques. In common, they were never restricted to physical phenomena. However, the popular medicine knowledge, or curandeirismo (healers practices), is based on tradition, using empirical knowledge that does not come from a degree but the oral transmission. At times, it comes from family or, sometimes, accessed through the spiritual world 1.
The informant reported an intuitive knowledge, motivated by experimentation based on nature observation and study. Such ability allows her to replicate the experience of overcoming illnesses in other circumstances. Therefore, she stands out due to her knowledge of health care with medicinal plants.
Although not recognized in the literature, intuition and subjective knowledge are used in health care. A holistic approach recognizes intuitive wisdom as an ally to rational knowledge. However, in the light of Systemic Theory, intuitive knowledge is a characteristic of traditional cultures organized around a sophisticated environmental awareness. In biomedical medicine, it is commonly neglected, which can be related to the evolution of biological aspects and the separation between these aspects and culture in human nature 1.
According to the informants' reports, the way they acquired such knowledge extrapolated oral learning. They oftentimes learned by observing their parents' performance. Thus, according to the theoretical framework adopted, in addition to the social interrelation, the environmental interrelation was also fundamental to the knowledge that some of the interlocutors hold about health care with medicinal plants.
As the knowledge origin is related to more experienced family members, the elderly, in addition to disseminating this knowledge about medicinal plants, stand out for their wisdom 14-15. The acquisition of knowledge about medicinal plants for health care by family members has been reported in other studies 3-16. This knowledge is transmitted orally between generations 16, which is associated with social interrelations, according to the Systemic Theory.
Although it is considered a popular knowledge, health care with medicinal plants is a widespread resource that requires plant providers and their associated knowledge. The pharmacist went after this knowledge because of his customers, who motivated him by ordering plants for their illnesses.
Health professionals' limited knowledge of medicinal plants might be related to their initial lack of interest in the topic. However, the absence of specific college subjects and academic discussions might explain this situation as well. However, personal experience, as well as the dialogue between scientific and popular knowledge, may change professional practices 17.
The phytotherapist realized she could work in this field due to an existing gap: an opportunity to work in this area handling such knowledge. For both the pharmacist and the phytotherapist, it was the social interrelation, discussed by Capra, that impelled them to learn about the care with medicinal plants. In this sense, although traditional knowledge is inherited from ancestors, its transmission also occurs through collective socialization 18.
Today's facilitated access to information, arising from the advent of the Internet, is unquestionable. However, there is concern about the quality and reliability of the information provided. The erveiro revealed to be careful with his research, probably because he is still an undergraduate and has already been warned about the sources.
Modernization and new communication methods are alternatives for obtaining knowledge. Therefore, people interested in learning end up distancing themselves from oral transmission, which reduces this form of knowledge dissemination 19. On the other hand, the adopted theoretical framework's concept of social interrelation, in contemporary times, can be perceived as something beyond face-to-face relations and can constitute a relationship network that disseminates the knowledge of health care with medicinal plants.
Regarding learning possibilities at conferences, these events' social interrelations stand out, enabling knowledge exchange and transmission.
Current medicine has its origin in popular knowledge regarding health 1. However, the popular medicine tradition, which has been historically transmitted orally between generations, nowadays seems to move a 'popular knowledge market' that grants a degree. This finding comes from observing that the informants, except for the erveiros, frequently deal with improvement or training courses in the area, whether teaching or refining their knowledge.
The knowledge transmission between generations is a form of propagation among this research's informants. This kind of knowledge exchange was perceived from the oldest to the youngest and in the opposite direction. This finding highlights the social interrelation between those who belong to the same family group, as observed in other studies 3-20.
According to Capra 1, societies developed popular medicine mainly in the heart of a family (or community). Moreover, those beliefs and activities are transmitted orally.
As it is not always possible to have an apprentice at home, the informants end up spreading their knowledge in other social environments with people they relate to, as with the holistic therapist. However, knowledge about health care with medicinal plants is acquired through observation and experience, accumulatively, without a systematic process. For this reason, the transmission needs to occur within the family core to reduce the chance of this knowledge extinction 13.
From the informants' reports, it is possible to verify that they are concerned about perpetuating such knowledge and continue health care with medicinal plants. Other studies (21; 22; 23) have presented this concern with the possibility of this knowledge disappearing.
Besides, the oral transmission of health care with medicinal plants does not specify a specific period or place for learning, as it is in everyday life that beliefs and practices are shared 15. However, the transmission of this traditional knowledge to future generations has decreased as the youngsters tend to use industrialized medicine and have no interest in such knowledge 24. Another study has already observed that using the Internet to consult treatments with plants prevails among the youngest informants 3.
This study's informants transmit their knowledge about medicinal plants in health care in the different places where they establish their social interrelations. This knowledge becomes available to people who interact with the interlocutors, enabling them to play an essential role in maintaining such knowledge 15.
Although it is typical for informants, the pharmacist believes that the oral transmission of medicinal plants' knowledge hinders its perpetuation.
When reflecting on the oral tradition of the medicinal plants' knowledge dissemination, the pharmacist criticizes its loss. If it is not documented, it does not become accessible to those who are not present at that exact moment or in the context of tradition. Therefore, the limited documentation of this traditional knowledge contributes to its dissolution 5.
The informants also transmit their knowledge by teaching in courses on the topic, outside familiar dynamics. This more formal and organized dissemination allows them to spread their knowledge in different places beyond the family core.
The courses on medicinal plants offer a hybrid learning that combines common and reified sense, based on experimentation and association of popular practices as well as scientific evidence 14. Capra recognizes orality as the primary tool for disseminating knowledge related to popular medicine. However, considering the courses as hybrids allows us to presume that there is a diffusion of beliefs and related activities in addition to the transmission of knowledge about plants.
Conclusion
Individual, social, and environmental interrelations influence the practice of health care with medicinal plants. In this sense, caring has a subjective meaning related to the culture, history, and the environment in which a person is, being a way to find integrality and holism.
Ethnobotany and Systemic Theory made it possible to describe the interrelations of people who perform health care with medicinal plants. However, it brought a concern regarding the perpetuation of this knowledge since oral transmission has not been significant due to the lack of people interested in learning.
Caring with medicinal plants is not always a person's choice, and it can be interpreted as a 'gift' or something spiritual. The family can also be the source of this care and, in a more formal way, training courses on the topic.
This study contributes to an expanded view of health care, describing the person in their different interrelation forms. It allows a holistic view that recognizes popular knowledge validity and its complementarity with current medicine's scientificity. Also, recovering the traditional knowledge associated with medicinal plants' use contributes to the maintenance and dissemination of this knowledge. Further studies are recommended to contribute to the visibility and recovery of traditional knowledge related to health.
REFERENCES
1. Capra, F. O ponto de mutação. 30a ed. São Paulo: Cultrix, 2012. [ Links ]
2. Badke MR, Heisler, EV, Ceolin S, Andrade A de, Budó MLD, Heck RM. O conhecimento de discentes de enfermagem sobre uso de plantas medicinais como terapia complementar. Revista Fundamental Care (Internet), v. 9, n. 2, p. 459-65, abr./jun. 2017. (acesso em 2019 jan 13). Disponível em: https://www.researchgate.net/publication/316202874_O_conhecimento_de_discentes_de_enfermagem_sobre_uso_de_plantas_medicinais_como_terapia_complementar_Nursing_students_knowledge_on_use_of_medicinal_plants_as_supplementary_therapy [ Links ]
3. Almeida C, Barbieri RL, Ribeiro MV, Lopes CV, Heck RM. Espinheira-santa (Maytenus ilicifolia Mart. ex Reiss.): saber de erveiros e feirantes em Pelotas (RS). Revista Brasileira de Plantas Medicinais (Internet), v. 17, n. 4, supl. I, p. 722-9, 2015 (acesso em 2018 jun 28). Disponível em: http://www.scielo.br/pdf/rbpm/v17n4s1/1516-0572-rbpm-17-4-s1-0722.pdf [ Links ]
4. Brasil. Decreto nº 5.813. Política Nacional de Plantas Medicinais e Fitoterápicos. Brasília: Ministério da Saúde (Internet), 2006 (acesso em 2012 dez 10). Disponível em: http://dtr2004.saude.gov.br/dab/docs/legislacao/decreto5813_22_06_06.pdf [ Links ]
5. Leonard CM, Viljoen AM. Warburgia: a comprehensive review of the botany, traditional uses and phytochemistry. Journal Ethnopharmacology; 2015. 13(165): 260-85. [ Links ]
6. Silva RS, Matos LSL, Araújo EC, Paixão GPN, Costa LEL, Pereira A. Práticas populares em saúde: autocuidado com feridas de usuários de plantas medicinais. Revista enfermagem UERJ (Internet), v. 22, n. 3, p. 389-95, mai./jun. 2014 (acesso em 2018 dez 01). Disponível em: http://www.facenf.uerj.br/v22n3/v22n3a16.pdf [ Links ]
7. Almeida, C. Espinheira-santa (Maytenus ilicifolia): saberes e práticas de erveiros e feirantes que comercializam a planta no centro de Pelotas. 2013. 72f. Dissertação (Mestrado em Enfermagem) - Faculdade de Enfermagem, Universidade Federal de Pelotas, Pelotas, 2013. [ Links ]
8. Víctora CG, Knauth DR, Hassen MN. A. Pesquisa qualitativa em saúde: uma introdução ao tema. Porto Alegre: Tomo Editorial, 2000. [ Links ]
9. Albuquerque UP, Lucena RFP. (Orgs.). Métodos e técnicas na pesquisa etnobotânica. Recife: Ed. Livro Rápido/NUPEEA, 2004. [ Links ]
10. Goodman LA. Snowball sampling. The Annals of Mathematical Statistics; 1961. 32(3): 619-70. [ Links ]
11. Bardin, L. Análise de Conteúdo. 1a ed. São Paulo: Edições 70, 2016. [ Links ]
12. Brasil. Resolução nº 466/12 que dispõe sore pesquisa envolvendo seres humanos. Brasília: Ministério da Saúde (Internet), 2012 (acesso em 2012 dez 30). Disponível em: https://bvsms.saude.gov.br/bvs/saudelegis/cns/2013/res0466_12_12_2012.html [ Links ]
13. Singh AG, Kumar A, Tewari DD. An ethnobotanical survey of medicinal plants used in Terai forest of western Nepal. Journal Ethnobiology Ethnomedicine; 2012. 8: 19. [ Links ]
14. Martins S da R, Pereira FW, Acosta DF, Amorim CB. Representações sociais de profissionais da saúde acerca das plantas medicinais. Revista cubana de Enfermería (Internet), v. 33, n. 2, 2017 (acesso em 2018 jul 24). Disponível em: http://revenfermeria.sld.cu/index.php/enf/article/view/1065/258 [ Links ]
15. Silveira DDS, Albuquerque MBB. Práticas de cura, magia, educação e saberes sobre plantas poderosas na Amazônia. Revista Cocar (Internet), v. 9, n. 18, p. 255-84, jul./dez. 2015 (acesso em 2018 jul 24). Disponível em: https://paginas.uepa.br/seer/index.php/cocar/article/viewFile/713/535 [ Links ]
16. Miranda TG, Oliveira Júnior JF, Martins Júnior AS, Martins ACCT. O uso de plantas em quintais urbanos no bairro da Francilândia no município de Abaetetuba, Pará, Brasil. Scientia Plena (Internet), v. 12, n. 6, p. 2-18, 2016 (acesso em 2018 set 06) Disponível em: https://www.scientiaplena.org.br/sp/article/view/3058 [ Links ]
17. Goés ACC, Silva LSL, Castro NJC. Uso de plantas medicinais e fitoterápicos: saberes e atos na Atenção Primária à Saúde. Rev. Aten. Saúde, São Caetano do Sul; 2019. 17(59): 53-61. doi: 10.13037/ras.vol17n59.5785 ISSN 2359-4330 [ Links ]
18. Silva TLS, Rosal LF, Montão DP, Oliveira MFS, Batista RF. Conhecimentos sobre plantas medicinais de comunidades tradicionais em Viseu/Pará: valorização e conservação. Revista brasileira de agroecologia; 2019. 14(3): 72-83. doi: 10.33240/rba.v14i3.22522 [ Links ]
19. Silva PH, Oliveira YR, Abreu MC. Entre símbolos, mistérios e a cura: plantas místicas dos quintais de uma comunidade rural piauiense. Gaia Scientia; 2018. 12(1): 1-16. [ Links ]
20. Souza AMB. De, Barbosa Júnior LB, Lira M dos S, Costa LF, Simonetti ER de S. Estudo de caso de plantas medicinais no povoado Dezesseis, zona rural do município de Augustinópolis-TO (Internet). XVI ERA Encontro Regional de Agroecologia do Nordeste, Rio Largo, Alagoas, v. 1, n. 1, 2017 (acesso em 2018 jul 30). Disponível em: http://www.seer.ufal.br/index.php/era/article/view/3720/2913 [ Links ]
21. Belayneh A, Asfaw Z, Demissew S, Bussa NF. Medicinal plants potential and use by pastoral and agro-pastoral communities in Erer Valley of Babile Wereda, Eastern Ethiopia. Journal Ethnobiology Ethnomedicine; 2012. 22(8): 42. [ Links ]
22. Bibi S, Sultana J, Sultana H, Malik RN. Ethnobotanical uses of medicinal plants in the highlands of Soan Valley, Salt Range, Pakistan. Journal Ethnopharmacology; 2014. 155(1): 352-61. [ Links ]
23. Dutt H C, Bhagat N, Pandita S. Oral traditional knowledge on medicinal plants in jeopardy among Gaddi shepherds in hills of northwestern Himalaya, Jamp; K, India. Journal Ethnopharmacology; 2015. 168: 337-48. [ Links ]
24. Mata ND, Sousa RS, Perazzo FF, Carvalho JC. The participation of Wajãpi women from the State of Amapá (Brazil) in the traditional use of medicinal plants--a case study. Journal Ethnobiology Ethnomedicine; 2012. 19(8): 48. [ Links ]
How to cite: Almeida C, Ribeiro MV, Kaster Portelinha M, Oliveira SG, Barbieri, RL. Interrelations in the care with medicinal plants - “it comes from the cradle”. Enfermería: Cuidados Humanizados. 2020;(9): 229-242. Doi: https://doi.org/10.22235/ech.v9i2.2208
Authors' participation: a) Conception and design of the work; b) Data acquisition; c) Analysis and interpretation of data; d) Writing of the manuscript; e) Critical review of the manuscript.
Correspondence: Camila Almeida; e-mail: almeidakk@yahoo.com.br. Márcia Vaz Ribeiro; e-mail: marciavribeiro@hotmail.com. Márcia Kaster Portelinha; e-mail: portelinhamarcia@gmail.com. Stefanie Griebeler Oliveira; e-mail: stefaniegriebeleroliveira@gmail.com. Rosa Lía Barbieri; e-mail: lia.barbieri@gmail.com
Received: February 10, 2020; Accepted: October 07, 2020
 Este é um artigo publicado em acesso aberto sob uma licença Creative Commons
Este é um artigo publicado em acesso aberto sob uma licença Creative Commons
