











 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Curriculum ScienTI
Curriculum ScienTI
 Permalink
Permalink
Introduction
Gestation is a physiological phenomenon in a woman’s life, which usually evolves without intercurrence. Gestation is a physiological phenomenon in the life of a woman that usually evolves without intercurrence. However, there is a small portion of pregnant women, called high risk, who, because they have a disease or suffer some health problem, are more likely to have an unfavorable evolution 1 .
Pregnant women with cardiopathy are included in this group, as their obstetric and fetal risks are potentialized during the pregnancy-puerperal cycle. Heart disease is considered the largest non-obstetric cause of maternal morbidity and mortality in the world 2.
The occurrence of cardiovascular diseases in pregnancy ranges from 0.2% to 4% in Western countries and its complications are related to thromboembolic events, heart failure, and arrhythmias, among others 3.
In Brazil, the incidence of heart disease during pregnancy exceeds international statistics, with a rate of 4.2% 4). This percentage is attributed to the high incidence of rheumatic disease that affects childbearing-age women, representing 80% of cardiopathies during gestation 5.
Rheumatic disease, in turn, is considered an important etiology of valvular heart disease, since the scars from the inflammatory process that affects all heart follow-ups during the outbreaks of this disease cause heart valve deformation 6.
In pregnancy and in the postpartum period, cardiovascular changes associated with pregnancy may contribute to clinical deterioration in these patients and often to the initial diagnosis of valvular heart disease 7. In this period, circulating blood volume increases by approximately 30% to 50%. Concurrently, systemic vascular resistance substantially reduces, and blood pressure decreases. These changes begin in the first trimester and peak at 24 weeks’ gestation, with an additional increase in the immediate postpartum period 2.
Although gestation is a biological and social event that marks some of the most important moments in a woman’s life, it becomes complex when associated with the problems, limitations, and risks inherent in heart disease 8
In addition, considering that pregnancy is a choice for women who desire this experience is necessary; their decisions may be based on several conscious and unconscious reasons such as deepening a man-woman relationship, concretizing the desire for continuity and hope of immortality, maintaining a broken bond, competing with family members, and filling an internal void, among others ( 8). These factors help many women to desire pregnancy despite the high risk.
However, little is known about the experience of high-risk gestation in women with heart disease. In general, the literature has focused on the cardiovascular repercussions and clinical outcomes of gestation 9.
Faced with the lack of studies, this investigation aims to answer the following questions: What meanings do women with heart disease attribute to their high-risk pregnancy? What is your perception of the risk for the mother-child binomial?
Thus, this study aimed to comprehend the meanings women with heart disease attribute to their high-risk pregnancy and to identify their perception of the risks to the mother-child binomial
Methodology
This is a qualitative-quantitative study, which used the Discourse of Collective Subject, based on the Social Representation Theory 10.
In an empirical study, the thought, materialized in the form of discourse, is a qualitative variable. However, as it is a collective thought, it is also characterized as a quantitative variable when considering it expresses the individuals’ opinions (10).
This study was conducted in a gynecology and obstetrics outpatient clinic at a public hospital in the interior of São Paulo, Brazil. Data collection was performed from November 2011 to May 2015. The data collection period was extended because the study was conducted at a general hospital that serves few pregnant women with cardiopathies.
The inclusion criteria were: to be pregnant with heart disease as of the second trimester of pregnancy, to be receiving prenatal care in the institution, and to consent to participate. The choice of this period was due to the increase in blood volume, which peaks at 24 weeks’ gestation and is 40% larger than the pregravid volume (1). The exclusion criteria were: unavailability to participate in the interview and self-reported verbal inability to speak.
A sample was composed of thirty-nine pregnant women who met the previously established inclusion criteria. This sample consisted of the total of patients cared for in the data collection period. All participants consented to participate in the interview, which was not interrupted. Data were collected using semi-structured interviews and an instrument with sociodemographic (age, education level, marital status, number of children) and clinical data (previous abortions, family planning, gestational age, participation or not in a family planning group, etiology of the heart disease), as well as two leading question: "In your opinion, what does being a mother with heart disease mean to you? Were you aware of the risks posed by this gestation before getting pregnant?
The interviews were conducted individually and in a private environment. Among the researchers, there was a PhD-qualified professor with experience in the DSC technique who conducted the analysis of the interviews, as well as undergraduate and graduate students. No one had any kind of bond with the participants.
The ICF contained the researchers’ information provided to the patients when the latter were invited to participate in the study. The transcripts of the interviews could not be sent back to participants for comments.
After the 39 interviews, the discourses were transcribed and the discourse analysis was started, using the methodological approach of the Discourse of the Collective Subject (DSC) 10 Methodological figures such as central ideas and anchoring, as well as their respective key expressions were used for transcription. Key expressions and anchoring are pieces or fragments of material (discourse) comprising literal descriptions of the testimonies, disclosing the essence of the representation content and their underlying theories. The central idea is a name or expression disclosing and describing, in a brief and accurate manner, the meanings behind the testimonies, which will result in the DSC 10).
The methodological steps followed from the interviews to the synthesis of the discourses were:
Reading of the testemonies collected from the interviews;
Reading of the answer to each question, writing down the key expressions selected;
Identification of the central ideas of each answer;
Analysis of all key expressions and central ideas, homogeneously grouping their similarities;
Identification and designation of the central idea of the homogeneous group, constituting the synthesis of the central idea of each discourse;
Construction of discourses of the collective subject after spotting the central ideas and key expressions that named these discourses. The discourse of the collective subject proposes reconstructing an empirical collective subject, whose opinions are expressed through a discourse in the first person singular.
After analyzing the transcripts, the recordings were deleted.
The data were obtained after approval of the project by the Research Ethics Committee of the institution under No. 3911/2011, and the participants signed the informed consent form after being assured of anonymity.
Results
The participants were 39 pregnant women with a mean age of 25.3 years. Nearly half (53.5%) had completed high school and only two (7.1%) had higher education. Regarding marital union, most had a partner (30; 76.9%), that is to say, they were married and lived with a partner. In addition, more than half of the interviewees (27; 69.2%) were progenitors.
Regarding clinical and obstetric variables, 13 (33.3%) pregnant women had previous abortions and 25 (64.1%) had not planned the current pregnancy. In addition, 26 (66.6%) had already been pregnant, and most of them (73.0%) had been pregnant more than once. The mean gestational age was 27 weeks (SD = ± 2.69). Most of the participants (84.6%) did not participate in family-planning groups and did not use a contraceptive method (82.0%).
Regarding the etiology of heart diseases, 16 (41.0%) pregnant women had a predominant rheumatic fever, followed by valvular heart disease (14;35.8%), arrhythmias (4; 10.2%), mitral valve prolapse (2; 5.1%), myocardiopathies (2; 5.1%), and congenital heart disease (1; 2.5%).
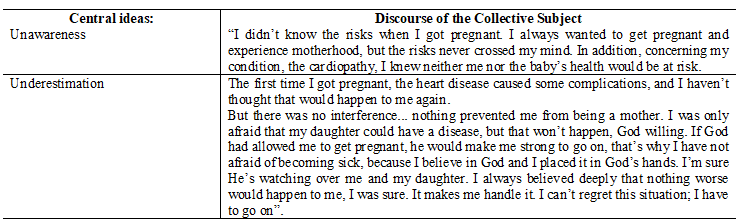
By analyzing the transcripts, key expressions and central ideas were identified, and the discourses of both themes, derived from the leading questions, were constructed. Quadro 1. Quadro 2.
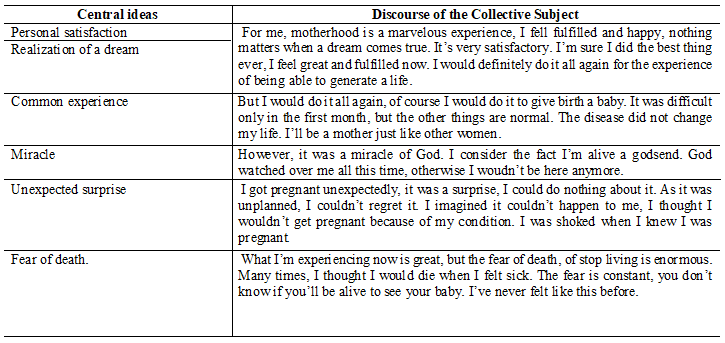
Quadro 1: Synthesis of central ideas and collective subject discourse related to the theme meanings of high-risk pregnancy.
Discussion
The limitations of this study are related to the fact that it was developed in a single health service with local characteristics. However, the results provide an understanding of the magnitude and the complexity of a relevant public health problem that affects developing countries, in which the sequelae of fever represent 60% of all cardiovascular diseases in children and young adults 11.
This disease is often associated with poverty and poor living conditions, with a high socioeconomic burden not only for the health services, but also for patients and their families due to chronic sequelae in the early life stages 12. A Brazilian study performed in a cardiology hospital involving 650 pregnant women with heart disease showed 50% of the participants had valvular heart disease 13.
However, in spite of the recognized importance of the problem and the existence of proven effective strategies of prevention and treatment of the disease, the health actions developed to date in Brazil have proved to be insufficient for the adequate control of the fever, as shown in this study, in which 41% of participants had rheumatic heart disease 14.
In this sample, adult women with an average age of 25 years, who had a partner and a complete secondary education level predominated. These data were corroborated in a study carried out with healthy pregnant women, in which the education level of most of the participants was over 11 years 15. The pregnant women’s education level is relevant, given that it is associated with neonatal mortality, especially in developing countries, in addition to reflecting the mother’s socioeconomic status 16. Despite the complexity involved in gestation in women with heart disease, this fact should also be considered when interpreting the results.
Although gestation is a dynamic, subjective and diverse process, the testimony showed it was the crowning of some participants’ personal desire, and even a dream, built from the perspective of the sociocultural and family context experienced by these women. In addition, one must consider that pregnancy can sustain and consolidate the feminine identity for many of these women, despite the fact that it is a choice and the fear of the real consequences for the mother-child binomial 17.
In some situations, even if it is properly oriented, the desire to bear children contradicts the medical indication, as shown in the literature and in the results of this investigation 8. This attitude is likely linked to the intimate need to adhere to the female role of procreation, which seems to be associated with their model of feminine identity.
In addition, pregnancy can also help them in overcoming their personal limits, so it is not planned but desired. This may be linked to the fact that more than 80% of the participants did not use contraceptive methods.
This reality is a very different from that of a recent study conducted in North America involving 505 women with complex congenital heart disease. In this investigation, although 86% of the interviewees used contraceptive methods, the authors recognized that health education and family planning practices were still deficient for these patients 18).
Another interesting element revealed by the study participants was the negative feelings about the developments that permeate a high-risk pregnancy, ratified by the fears, uncertainties, and insecurity present in the interviewees’ discourse. A qualitative research conducted with 19 women with peripartum cardiomyopathy in Sweden corroborated these data. In this investigation, anguish, insecurity, and emotional discomfort were the most prevalent feelings in the pregnant women’s discourse, besides not feeling properly cared for and informed by health professionals 19.
This study also highlighted the ignorance of the risks of gestation indicated by the participants. The absence or insufficiency of knowledge that women have about their health and complications interferes with their autonomy, often preventing them from making decisions about gestation, delivery, and treatment. A national study involving pregnant women with preeclampsia and specific gestational hypertensive disease showed they were unaware of the disease and its risks during this period, which contributes to aggravating the consequences of high-risk pregnancy 20.
However, when risks become a concrete possibility, one realizes that religion/spirituality is the protection they seek to face a situation marked by impotence and uncertainties. The attachment to religion/spirituality revealed in the interviews reaffirms the premise that this can be a source of relief and protection to address difficulties.
A recent study involving 17 cardiac patients showed the need to transcend the care relationship based on the biomedical model to reach an existential relationship in which women are considered to be endowed with possibilities. In this investigation, the authors highlight the importance of a care consistent with the real objective and subjective needs of pregnant women with cardiopathy 21.
Therefore, the management of pregnancy in these circumstances requires a humanized care, from the perspective of integral care, guided by reception and guidance.
Despite the concern with high-risk pregnancies in the country, there is still a gap with regard to the establishment of public policies that ensure care associated with the unique expectations and needs of these women. The study contributes so that health professionals perceive the problem, considering the subjective aspects involved in high-risk pregnancy. Furthermore, this study highlights a neglected social and health problem in Brazil, with family, socioeconomic and cultural influences.
Conclusion
The results of the study indicate that high-risk gestation is a process associated with personal satisfaction and fulfillment of a dream, often permeated by negative feelings about the inevitable risks to the mother-child binomial.
The risks are not always known and may be underestimated; for these women, the risk seems to be less important than being a mother. However, religion/spirituality support them in facing adversity and overcoming fears. Thus, health professionals should approach high-risk pregnancies focused on subjective issues experienced by these women. In addition, this study became a neglected social and health problem in this country visible. This fact demonstrates the importance of establishing public policies that ensure reception and multidisciplinary care in the health care network for these women.

