










Serviços Personalizados
Journal

Artigo
 texto em
texto em  Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
Links relacionados
Compartilhar

 Permalink
PermalinkEnfermería: Cuidados Humanizados
versão impressa ISSN 1688-8375versão On-line ISSN 2393-6606
Enfermería (Montevideo) vol.9 no.2 Montevideo dez. 2020 Epub 01-Dez-2020
https://doi.org/10.22235/ech.v9i2.2041
Original articles
Profile of elderly patients assisted by mobile emergency service
1
 http://orcid.org/0000-0002-0765-8089
http://orcid.org/0000-0002-0765-8089
1
http://orcid.org/0000-0002-1093-1437
1 Universidade Estadual do Sudoeste da Bahia. Brasil
2 Universidade do Estado da Bahia. Brasil
This study aimed to outline the profile of emergency-medical care performed to the elderly population through the prehospital regional medical-emergency regulation center and the mobile emergency-care system. The data analyzed here was extracted from a database of the emergency-calls made to reach out the of the regional medical-emergency regulation center and the mobile emergency-care system over the year of 2013 at the city of Jequié, Brazil. The absolute and relative frequencies were calculated for the variables evaluated. the regional medical-emergency regulation center received 3,505 calls and 2,066 ambulance units were sent out. Both at the regional medical-emergency regulation center and the ambulance crew the age of the patients assisted ranged from 60 to 79 years old, and most of the emergency-calls were attended during weekdays and during the morning shifts. Most of the elderly assistment were at their households, having clinical assistance, and afterwards they were conducted to a public hospital network. Hypertensive crisis, chronic pain, neurological and dyspnoea issues have prevailed among other diagnosis. Thus, we conclude here that the emergency- prehospital care is essential to meet the urgent demands of the elderly population.
Keywords: Health Services for the Aged; Health Services; Comprehensive Health Care; Aged; Emergency Medical Services
O presente estudo objetiva traçar o perfil do atendimento aos idosos pela central de regulação pré-hospitalar e pelo serviço de atendimento móvel de urgência. Caracterizou-se como estudo epidemiológico, descritivo realizado com idosos residentes em Jequié, Bahia. Utilizou-se banco de dados dos atendimentos da central de regulação e do serviço móvel de ambulância do ano de 2013. Calculou-se as frequências absoluta e relativa para as variáveis avaliadas. A Central de Regulação recebeu 3.505 chamadas, e encaminhadas 2.066 atendimentos de ambulâncias. Na regulação e nas equipes de ambulância prevaleceram idosas, de 60 a 79 anos, atendidas durante dias úteis da semana e no turno matutino, atendidos em domicílio, com realização de atendimento clínico, e conduzidos para rede hospitalar pública. Entre os agravos prevaleceram crise hipertensiva, dor, neurológicos e dispneia. No município, o atendimento pré-hospitalar móvel de urgência é essencial para atender as demandas de urgência dos idosos.
Palavras chave: Serviços de Saúde para Idosos; Serviços de Saúde; Assistência Integral à Saúde; Idoso; Serviços Médicos de Emergência
Este estudio tuvo como objetivo esbozar el perfil de la atención a las personas mayores a través del centro de regulación prehospitalario y el servicio móvil de atención de emergencia. Se caracterizó como estudio epidemiológico, descriptivo realizado con ancianos residentes en Jequié, Bahía. Se utilizó la base de datos de las atenciones de la central de regulación y del servicio móvil de ambulancia del año 2013. Se calcularon las frecuencias absoluta y relativa para las variables evaluadas. La Central de Regulación recibió 3.505 llamadas, y se encaminaron 2.066 llamadas de ambulancias. En la regulación y en los equipos de ambulancia prevalecieron ancianas, de 60 a 79 años, atendidas durante días hábiles de la semana y en el turno matutino, en domicilio, con asistencia clínica y trasladados a la red pública hospitalaria. Entre las enfermedades prevalecieron las crisis hipertensivas, dolor, enfermedades neurológicas y disnea. En el municipio, la atención prehospitalaria móvil de urgencia es esencial para atender las demandas de urgencia de los ancianos.
Palabras Clave: Servicios de Salud para Ancianos; Servicios de Salud; Atención Integral de Salud; Anciano; Servicios Médicos de Urgencia
Introduction
One of the greatest achievements of mankind is the aging of the global population. Following the United Nations Organization prospects, the number of individuals having 60 years old of age and over will continue to rise in a global scale, following a trend that has happened in the last few decades. This aging phenomenon is due to several factors, and some of them can be listed as following: the increase in average life expectancy; the technological development in treating diseases; the improvements in social conditions and healthy habits; the investment and advancement of preventive health-care; the marked reduction in fertility rate that seems, in some countries, to be the main responsible for the percentage increase in the number of elderly population when compared to other different age groups 1.
Data based on the 2010 Brazilian census specified that the population of elderly people having 60 years old of age and over was around 20 million inhabitants, whereas, in the year of 2000 this population was around 14 million. These population projections estimate that in 2020 Brazil will be the sixth country in the world with the oldest population 2,3. However, it is known that in the year of 1940 the life expectancy in Brazil was around 45.5 years old, and in the year of 2011, it has increased to 74.1 years old, thus, representing a gain of 28.6 years in life expectancy. When accounting for sex (i.e., gender), women have had longer life expectancy (e.g., around 77.7 years) when compared to men (e.g., 70.6 years) 2.
The World Health Organization (WHO) recognizes that people over 65 years old are considered elderly, but this framework has been utilized in developed countries only. In Brazil (e.g., a country in development), people are elderly at the age of 60 years old (i.e., ‘old age’). In developed countries, therefore, according to the WHO people are considered ‘old’ from the age of 65 years old on 4.
The increase in the number of elderly people in the world has brought higher demands on health services provided. These services are considered to be burdened out due to factors as: higher costs for treating chronic non-transmissive conditions (which have a higher incidence among the elderly people); higher and longer rates of hospitalization and higher average cost of hospitalization (when compared to younger people); and the higher need to use extra hospital resources (e.g., medication and equipment) 5.
The chronic non-transmissive conditions among the elderly population have been associated with their lack of functional capabilities which are related to the increasing of their body weakness, walking difficulties, higher risk of failing (and from falling own height). Lately, based on these factors, it has been noted a greater need for special care outside the elderly population households (i.e., institutionalization) 6.
In this context, the elderly population have become more vulnerable to the worsening of their health problems and, therefore, they are demanding more from the medical-emergency care services (e.g., ambulance). Among others, the Brazilian mobile emergency-care system (i.e., SAMU) stands out for having its implementation brought to the population a huge impact on reducing hospitalizations and rates of death 7. Hence, when considering the aging of the population, it is important for health professionals to know better about the health background of their patients in order to deliver better and improved medical services, this way, greatly valuating better and higher care-based professional quality on the needs of the elderly population 8.
In 2003, the National Brazilian Emergency Care Policy introduced the SAMU emergency-care and ever since this public mobile emergency-care system has offered to the population quick and effective access to health care when it comes to clinical, surgical, traumatic, obstetric, and psychiatric emergencies 9. It is relevant to a population over 60 years of age due to their physical condition, especially due to the lack of prevention of chronic diseases that are not transmitted 10.
Even though this mobile emergency-care system was implemented more than a decade ago, just a couple of studies in the literature have identified the characterization of the services provided to the elderly patients together with the type of emergency-care delivered to them 11-13. In this fashion, there is a pressing need to unveil which are the health conditions affecting the elderly population the most, in order to adapt proper care to their necessities during the period of receiving medical-care provided by the health system in general, including the public emergency-care services in Brazil. Thus, the present study aimed to outline what kind of specialized medical-care service was provided by the regional prehospital medical-emergency center and by the mobile emergency-care system (SAMU) at the city of Jequié-Bahia, Brazil.
Methodology
This study was based on a quantitative and epidemiological approach with a cross-sectional design. The data utilized here was originated from the medical-care records of the regional medical-emergency regulation center and SAMU ambulances units in the city of Jequié (South-west part of the Bahia State, Brazil). This city is where a headquarter of a regional SAMU is located, being responsible for assisting a population size of around 530.000 inhabitants (from the city itself and from 25 satellite municipalities). Out of these 25 satellite municipalities, 15 have emergency-rescue ambulances covering the entire region. However, for this study, we utilized only data from the services of emergency-rescue ambulances assisting the elderly population from the city of Jequié.
The city of Jequié is located close by the riverbanks along the Contas River and according to the 2010 census, the city has a population in total size of 151,895 inhabitants (73,612 are men e 78,283 are women). Out of this total size, 17,247 inhabitants have 60 years old and more, and 7,420 are elderly men and 9,827 are elderly women. Additionally, out of the total elderly population, 1.400 l inhabitants live in rural areas and 15,897 in urban areas.
During the period from January to December of 2013, the medical records of the regional medical-emergency regulation center and the records referring to the care provided by two of the SAMU ambulances of Basic Support Units (USB) and Advanced Support Unit (USA) were analyzed. The difference between the two kinds of ambulance is that each of the USB has a team consisting of a nursing technician and a driver, while the USA has a physician, a nurse, and a driver.
For this study, 3,505 emergency call-data sheets were gathered containing the records of patients having 60 years old and over. Out of these data sheets, in 2,066 of the requests for emergency-care the medical team had to decide whether they would send an ambulance unit (USA or USB) to assist the elderly person who was calling for prompt medical-emergency services. All data sheets were firstly filled out by an auxiliary medical technician (TARM). Henceforth, this person is responsible for taking personal information notes of the solicitant (patient), his or her address, date and time of the call, as well as other relevant information observed by the TARM. After this first approach, the TARM hands over the emergency call sheet to the supervising physician who will be the one responsible for entering in those data and he or she will evaluate the severity of the situation (i.e., clinical, traumatic, obstetric, psychiatric or guidance). Finally, the physician will take the decision whether providing only guidance by the phone is enough, or there is a need to send out an ambulance unit to who is calling and demanding for medical assistance.
The data obtained from the regional medical-emergency regulation center and from the emergency-care provided by SAMU to the population of Jequié were the data sources for this study. The database was compiled in a Microsoft Excel spreadsheet and analyzed using frequency distribution (i.e., how frequencies are distributed over values). The database contained information on the profile of the patients (i.e., age and sex) and about all features of the services supplied to the population (i.e., day of the week which the service was provided, time of the working shift, type of vehicle, patient occupation, place where the incident has occurred, type of incident, services required by the patients, and the reason why the ambulance was solicited).
This study was approved by the Ethics and Research Committee of the State University of Southwest Bahia (UESB), under the legal rights: nº 911.309, CAAE nº 39472214.3.0000.005.
Results
The regional medical-emergency regulation center of Jequié, together with the SAMU, were responsible for processing 3,505 emergency-calls made during the year of 2013 which have assisted the elderly population of Jequié (i.e., age bigger or equals to 60 years old). Among the ambulance units of SAMU, it was documented 7,324 incidents, in which 2,066 were documented for the assistance of the elderly population (i.e., 28.2% of all calls). Therefore, it is worth to highlight a couple of inconsistencies found between the information given by the regional medical-emergency center and the municipality ambulance crew. The regional medical-emergency regulation center reported that the USBs drove out of their medical-emergency center 1,788 times, but the ambulance crew have detailed a difference in number (1,605 trips were reported), thus, showing a difference in number of 183 fewer trips. Moreover, the regional medical-emergency regulation center reported 402 trips using the USA, whereas the ambulance crew reported 461, indicating thus a difference in number of 59 extra trips.
Altogether, there was a total in difference of 124 trips reported. Based on these inconsistencies found in the sources of data, we can speculate that: i) the staff responsible for filling out the data sheets on the ambulance did not do it or it may have get lost on the away; ii) the age of the patient was reported differently at the two times when it was requested (i.e., at the regional medical-emergency center or during the assistance on the ambulance trip), thus, perhaps one particular patient (i.e. elderly) did not take part in the pool of data studied; and; iii) there may have been a cancellation of the emergency-service requested during the ambulance trip before it could reach out to the calling destination.
Following the Table 1, both in the regional medical-emergency regulation center and the mobile emergency-care system (SAMU), respectively, the numbers have revealed that the elderly patients assisted were: elderly female (i.e., 56.3%; 54.6%), patients age ranging from 60 to 79 years old (i.e., 64.5%; 62.5%), patient who has solicited the service during weekdays (i.e., 72.2%; 71.2%), patient assisted during the morning shifts (i.e., 32.7%; 31%), and patient who has solicited to received medical-care from a mobile emergency-care unit (USB) (i.e., 81.6%; 77.7%). Also, in the same table, one can observe a seemingly insufficient amount of information associated with some variables related to the regional medical-emergency regulation center (i.e., sex 1.3% and ambulance units utilized for giving assistance 37.5%), and other variables related to the mobile emergency-care units (i.e., sex 3.6%). For the other variables of the regulation (shift n = 1) and the Mobile Unit of assistance (age n = 2) the incompleteness of the information was insignificant.
The Table 2 displayed information of the data gathered from the records of the emergency-call sheets assisted by the mobile emergency-care system. Hence, one can notice that the predominant elderly population assisted was of: retired people (i.e., 81,4%), people assisted in their households (i.e, 88,3%), who has requested for clinical care (i.e., 80,7%), and who has been taken to a public hospital (i.e., 95,9%).
Table 1: Attributes of the medical care provided by the regional medical-emergency regulation center and the mobile emergency-care system (i.e., SAMU).
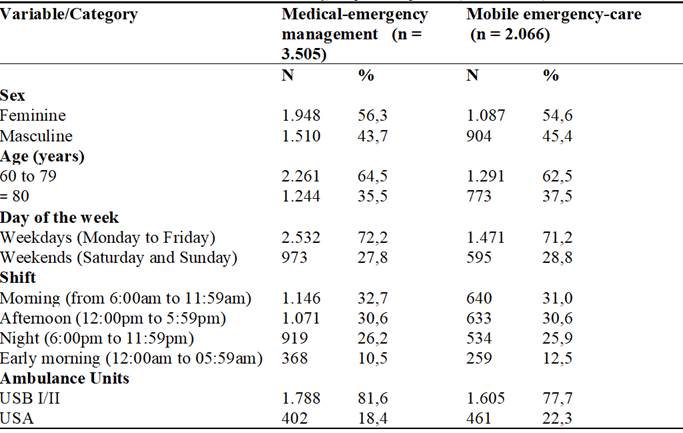
Source: Database of the regional medical-emergency management center and mobile emergency-care system (SAMU), Jequié, Bahia, Brazil, 2013.
Table 2: Characteristics of the information gathered from the emergency-service call sheets assisted by the mobile emergency-care system (SAMU).
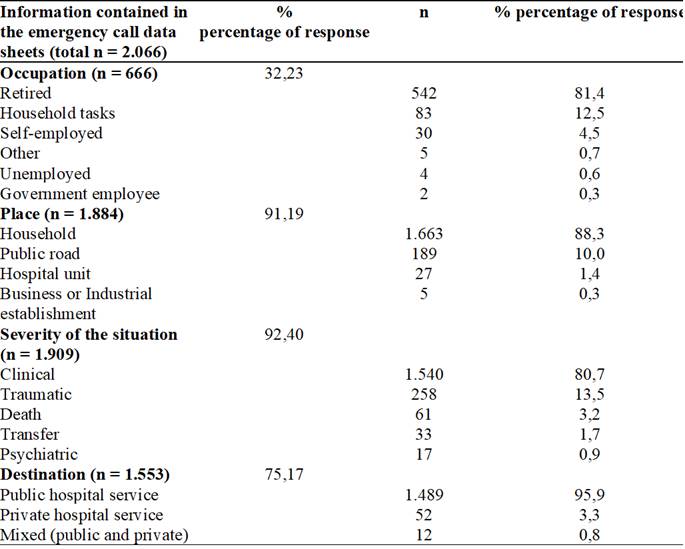
Source: Database of the mobile emergency-care system (SAMU), Jequié, Bahia, Brazil, 2013.
In Table 3, the health problems that affected the elderly population assisted by the mobile emergency-care units (SAMU) were displayed. This table pointed out that the main health issue demanded for emergency-care were hypertensive crisis (22.0%); pain (18.5%); neurological issues (16.2%), shortness of breath (i.e., dyspnea) (15.6%). Nonetheless, it is worth to call attention to the fact that for some of the elderly assisted, more than one health complication was registered.
Table 3: Health complications observed in the elderly population assisted by the mobile emergency-care units (SAMU).
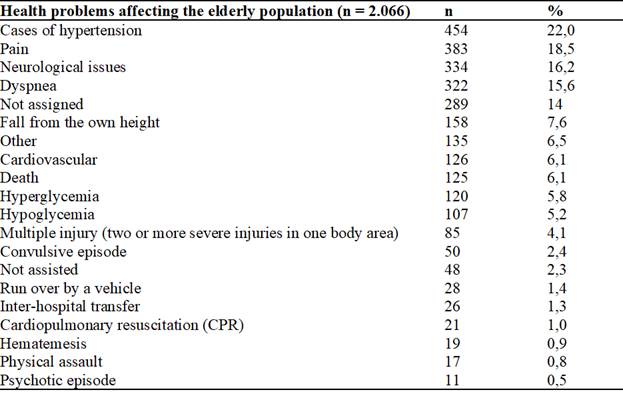
Source: Database of the mobile emergency-care system (SAMU), Jequié, Bahia, Brazil, 2013.
It should be noted that: in the neurological issues category (Table 3) patients affected by fainting, deviation of the labial commissure, hemiplegia (i.e., paralysis of one side of the body), hyperactivity disorder, dizziness, sudden illness, paraesthesia (i.e., sensation of pricking, tingling, or creeping on the skin), disorientation, anisocoria (i.e., pupils showing different sizes at the same time), syncope, and lethargy were included under this category. While within the cardio-circulatory issues category, cases of hypertension, bradycardia, cyanosis, tachycardia, and denaturation (i.e., low blood oxygen concentration) were included.
Discussion
This study detected a high percentage of emergency-services provided for the elderly population of Jequié linked to the lacking in the details in the patient registration forms (i.e., 20.5% of information missing from the registration forms). Based on this, we point out that this sort of emergency-services provided to the elderly could be improved if the details on the patient profile would have not been missing or filled out wrongly. Hence, we believe that the amount of missing information related to the emergency-assistance performed which is lacking from the registration forms might be associated with the high demand for emergency-care at certain times; the need for speeding up the calls when going throw each of the patient health issues; and due to quickly making decisions and search for a hospital unit to give continuity to the emergency-care (e.g., because one believes that the information missing or filled out wrongly is of less importance); or a reorganization of the practices involved when performing the patient registration service is missing.
It is worth to highlight that the information obtained from the regional medical-emergency regulation call center is essential for the recognition of the patients, the worsening of their health condition, and how to locate the patient. In October of 2014, a new topic was created under the protocol (i.e., standard set of rules) of SAMU as a “special protocol” which was based on how the emergency-service patient registration forms should be properly filled out 14. A study back in 2011 on elderly men assisted by the SAMU in the city of Teresina-PI-Brazil has referred to the same difficulties when filling out the emergency-service patient registration forms, which makes it difficult to identify the patient’s conditions and the medical assistance to be provided by the medical team 15.
During the period when the data was analyzed, 28.2% of the emergency-medical care provided by the prehospital regulation call center of SAMU in the city of Jequié was supplied for the elderly population, evidencing thus the importance of the emergency-medical care service for this age group. Hence, the improvement in expertise and refinement of the prehospital emergency-care team is essential for delivering a good prognosis for this population age group 16.
The aging process of the world population is accompanied by multiple comorbidity and coexisting conditions, some of which are chronic and make the elderly more susceptible to the need for emergency support. Most of the emergency-care provided for the elderly population surveyed in this study was initiated at their households. For instance, an exceptional care should be taken with the elderly when they are at home, as the risk of trauma due to their own vulnerability could be at most of the times prevented (16) .
To ensure high quality and efficiency in the care provided for the elderly patients, it is therefore necessary to develop measures that might improve the prehospital care 17. In this fashion, it is essential to identify new methods and approaches that might be capable of ascertaining the severity of the health issue earlier and, thus, better guiding the patient to the most appropriate health treatment and support.
In this study, it was identified that 54.6% and 56.3% of the care provided for the elderly by the mobile emergency-care system (SAMU) and by the regional prehospital regulation center, respectively, were for female individuals. These findings give support to a similar study, in which 42.629 elderly individuals were assisted by the SAMU, and 55.5% of these individuals were female 18. Also, another study has showed that 51% of the patients assisted by the SAMU were women 13.
Out of the three emergency ambulances units (SAMU) available, two units (USB) were responsible for 77.7% of the occurrences, while the USA unit took care of for 22.3% of the occurrences, and altogether SAMU has provided assistance for about 2.066 elderly individuals. When compared to all age groups, the USA (i.e., advanced emergency-care support unit) has made to 16.4% of the total occurrences. Based on this, we might suggest that there is a greater tendency to send out advanced emergency-care support when calls come in made by elderly people. Having this in mind, it is necessary to be aware of the needs of the elderly population. Thus, to reduce patient readmission and to improve the general functional capability of the emergency-medical care team, the elderly patients should be adequately assisted while they are still in prehospital emergency-care. Hence, we believe that the emergency-medical care team must be in constant training concerning the particularities required by the elderly population 16,19.
Out of all the elderly individuals assisted, 12.5% were reported as having informal activities and 4.5% as self-employed. Based on this information, one can note that an important portion of the elderly age group have work activities, and that they can emotionally impact their family life history by suffering from health problems which might give to rise disabilities.
In addition, the demand from the elderly population for the mobile emergency-care system service (SAMU) was not influenced by the day of the week. However, when evaluating the time span of the working shifts, it was observed that 31.0% of the occurrences took place during the morning shifts, and 61.6% during the afternoon shifts. This piece of information gives support to a previous study 18, in which the peak of assistance to the elderly individuals occurred at 10:00 am and remained on a plateau until 5:30 pm. Hence, it is worth to mention that, as observed in the results of our study, the working shift in which the regional medical-emergency call center was requested the most has occurred following the same proportion as found for the ambulance units service
The predominant type of occurrence among the elderly population investigated in this study was the clinical type, in which the cases of hypertensive episodes have prevailed. This result is similar to the outcomes of a previous study carried out in the municipality of Botucatu-São Paulo, Brazil, where the clinical occurrences have also predominated but the majority of the elderly patients were assisted due to seizures 20.
However, it should be said that in this age group the prevalence of arterial hypertension episodes is high, and previous studies carried out in the psychogeriatrics sector of a hospital in Itapira-SP, Brazil, have diagnosed 53.0% of the total number of the patients with hypertension 21. Another study has reported a high rate of hypertensive pseudo-episodes and symptomatic elevation of blood pressure in medical-emergency services which have been treated as a hypertensive crisis 22. As of rule of thumb in medical-emergency services, differentiating these kind of diagnosis as it might have a substantial impact regarding the best treatment to be addressed to the patients.
Another major complaint reported by the elderly patients was the chronic pain. A previous study conducted in the city of Florianópolis- Santa Catarina, Brazil, have showed that out of 1.656 patients in total, 29.3% of them had severe chronic pain and it was predominant among women (62.5%) and elderly people ranging in age from 60 to 69 years old (51%) 23. Also, another study carried out in the city of São Paulo-São Paulo, Brazil, has indicated the prevalence of severe chronic pain in 29.7% of the patients. The elderly portion of this same study have reported that the kind of pain which was bothering them the most was the lower back pain, followed by pain in the lower and upper limbs. Nevertheless, it is already known that these sorts of pain have a huge negative impact on daily activities, and especially among the elderly. The elderly individuals in this same study reported that their pain levels have persisted for more than two years and ranged from medium to severe. Hence, the presence of chronic pain was associated with the worsening of their functional capacity assessed through basic and instrumental activities of daily activities and mobility 24.
It has been proved that pain can be felt differently by distinct individuals and it may vary in constancy and intensity. Here in this study, the prevalence of the pain condition was high, demonstrating that this health issue might lead to greater complexities for the elderly population. A situation which is very often seen in Brazilian households can be described as when the professional caregiver or a family member (who takes care after their elderly relatives) start to take over control and making decisions concerning which health practices are the best for the elderly and, many times, they start to intervene as a primary source in providing care (or even emergency care) to these individuals 22. Thus, an increasing in requests for professional support that can deal with something considered to be an emergency such as suffering imposed by chronic pain can be evidenced.
The third reason and apparently the most prevalent symptom that lead the elderly to search for emergency-care assistance was neurological issues. This sort of health issue (e.g., stroke) are among the main conditions that may have a strong impact on the daily life of the elderly and their immediate family. It is noted that the elderly population in the world have rapidly increased, a fact that it is believed to be linked to the prevention and promotion of the elderly well-being 25.
A disability (which could be caused by a stroke) can lead to the need for a family rearrangement to care for this elderly individual, and can decrease their quality of life and negatively compromise intra-family relationships (e.g., division of labor of taking care within the family). When a family faces the need for a professional caregiver, it may burden this family economically. Regardless of whether this situation will be handled by a contracted caregiver or a member of this family, the burden imposed on this individual seems to be related to the level of functional independence of the elderly who requires care 26.
Complications due to dyspnea was widely mentioned among the records of symptoms screened by the prehospital emergency-care center. In a previous study, the symptoms of low-income elderly individuals were inspected during their last year of life, and it has been showed that dyspnea (i.e., 60%) was the third most mentioned symptom 27. Also, the results of the same study suggested that this symptom proved to be important in the prehospital emergency-care processing. Additionally, this symptom (i.e., dyspnea) has proved to be related to a vital condition of the human being: the breathing, as well as it can be an indicative of a general worsening of the health condition or a manifest of the first signs of the finiteness of life.
In this study, it was observed that the worsening of health conditions found by the emergency-care ambulance teams (which was possibly the reason requesting the emergency service) suggested failures in the primary care. The most recurrent records of health issues were related to chronic and non-communicable health conditions that primary care teams are responsible to take care of by the means of preventive measures 5. External factors, such as falling from own height, are also important in the morbidity and mortality of these individuals and in their quality of life 12. The basic health care providers need to be aware of these issues, and the prehospital service has an important role as a source of information to implement preventive-care measures.
Conclusion
The results of this study showed the high percentage of elderly people assisted by the regional mobile emergency-care system (SAMU) in the municipality of Jequié. Regarding the profile of the elderly assisted, it can be seen that both in the regional medical-emergency regulation center and in the mobile emergency-care system the elderly women (i.e, age ranging from 60 to 79 years old) were the individuals who prevailed in requesting emergency-care during the weekdays and during the morning and afternoon. Mobile emergency-care units were the most requested to assist the elderly population at their households, and the most frequent type of occurrence was classified as clinical (then patients were referred to a public support hospital unit. As for the health issues that led the physician regulator (i.e., at the regional regulation center) to refer an emergency-care ambulance unit, the following categories have prevailed: hypertensive crisis, pain, neurological conditions, and dyspnea.
We also could have evidence that the prehospital emergency-care is essential for the treatment of health issues within the elderly population. Consequently, this is an important threshold, for the complex levels of the Brazilian healthcare system. The requests for emergency-care made by the elderly population were most related to chronic and non-transmissible health issues, which are quite common within this age group (elderly). Therefore, it is worth mentioning that these health issues are avoidable when proper measures and preventive care are accessible to the elderly population, thus, it is essential to understand and study better the full profile of this worldwide growing population (i.e. elderly population).
REFERENCES
1. Lamela D, Bastos A. Comunicação entre os profissionais de saúde e o idoso: uma revisão da investigação. Rev Psicol Soc (Internet). 2012 (cited 2018 Nov 11); 24(3): 684-90. Available from: http://www.redalyc.org/html/3093/309326585020/ [ Links ]
2. Nasri F. O envelhecimento populacional no Brasil. Demografia e epidemiologia do envelhecimento. Einstein (Internet). 2008 (cited 2018 Nov 11); 6(1): S4-S6. Available from: https://s3.amazonaws.com/academia.edu.documents/46617649/envelhecimento_popu.pdf?AWSAccessKeyId=AKIAIWOWYYGZ2Y53UL3A&Expires=1535740578&Signature=v5RN4P9QsOkzo2m58ZCGIlZU0Ck%3D&response-content-disposition=inline%3B%20filename%3DDemografi_a_e_epidemiologia_do_envelheci.pdf [ Links ]
3. Miranda GMD, Mendes ACG, Silva ALA. O envelhecimento populacional brasileiro: desafios e consequências sociais atuais e futuras. Rev Bras Geriatr Gerontol (Internet). 2016 (cited 2018 Oct 25); 19(3):507-19. Available from: http://dx.doi.org/10.1590/1809-98232016019.150140 [ Links ]
4. OMS (Organização Mundial de Saúde) Relatório Mundial de Saúde, Banco de Dados. Genebra: Organização Mundial de Saúde, 1999. [ Links ]
5. Rubio VO. La Economia em Sanidad y Medicina: Instrumentos y Limitaciones. Barcelona: Euge, 1990. [ Links ]
6. Maciel ACG, Guerra RO. Influência dos fatores biopsicossociais sobre a capacidade funcional de idosos residentes no nordeste do Brasil. Rev Bras Epidemiol (Internet). 2007 (cited 2018 Nov 11); 10(2): 178-89. Available from: https://www.scielosp.org/article/rbepid/2007.v10n2/178-189/ [ Links ]
7. Luz CC, Junger WL, Cavalini LT. Análise da Atenção Pré-hospitalar ao Acidente Vascular Cerebral e ao Infarto Agudo do Miocárdio na População Idosa. AMB Rev Assoc Med Bras (Internet). 2010 (cited 2018 Dic 12); 56(4): 452-7. Available from: https://www.ingentaconnect.com/content/doaj/01044230/2010/00000056/00000004/art00019 [ Links ]
8. Veras RP, Oliveira M. Envelhecer no Brasil: a construção de um modelo de cuidado. Ciênc saúde colet (Internet). 2018 (cited 2019 Jan 15); 23 (6): 1929-36. Available from: https://doi.org/10.1590/1413-81232018236.04722018 [ Links ]
9. Vieira EB. Manual de Gerontologia: um guia teórico prático para profissionais, cuidadores e familiares. Rio de Janeiro: 2ª ed. Revinter, 2008. [ Links ]
10. Silva JVF, Silva EC, Rodrigues APRA, Miyazawa AP. A relação entre o envelhecimento populacional e as doenças crônicas não transmissíveis: sério desafio de saúde pública. Semina cienc biol saúde (Internet). 2015 (cited 2018 Oct 25); 2(3):91-100. Available from: https://periodicos.set.edu.br/index.php/fitsbiosaude/article/view/2079 [ Links ]
11. Silva HC, Pessoa RL, Menezes RMP. Trauma em idosos: acesso ao sistema de saúde pelo atendimento pré- hospitalar móvel. Rev Latino-Am Enfermagem (Internet). 2016 (cited 2018 Oct 20); 24:e2690. Available from: http://dx.doi.org/10.1590/1518-8345.0959.2690 [ Links ]
12. Franklin TA, Santos HCS, Santos Junior JA, Vilela ABA. Characterization of service of a pre-hospital care service to older persons involved in fall. J res fundam. care Online (Internet). 2018 (cited 2019 Jan 15); 10(1): 62-7. Available in: http://www.seer.unirio.br/index.php/cuidadofundamental/article/view/5977 [ Links ]
13. Lino FS, Costa ECL, Figueiredo MLF, Magalhães JM. Assistência ao idoso pelo serviço de atendimento móvel de urgência. Rev Enferm UFPI (Internet). 2014 (cited 2018 Oct 25); 3(1):25-31. Available from: http://www.ojs.ufpi.br/index.php/reufpi/article/view/1328/pdf [ Links ]
14. Brasil. Ministério da Saúde. Secretaria de Atenção à Saúde. Protocolos de intervenção para o SAMU 192 - Serviço de Atendimento Móvel de Urgência. Brasília: Ministério da Saúde. 2014. [ Links ]
15. Pereira LC, Alencar AA, Figueiredo MLF, Beleza CMF. Caracterização do atendimento de homens idosos pelo serviço móvel de urgência. Rev Cult Cuid (Internet). 2015 (cited 2018 Nov 11); 19(41);126-34. Available from: http://eds.a.ebscohost.com/abstract?site=eds&scope=site&jrnl=11381728&AN=103452505&h=0S%2fDLOStdfmEuHcgh8y8F6fZLLanR6uQPHzGpjp8G0dSTos9LJ00r6PmYh%2fNl9D8g9nbGxnZVcAt4UNCw1buxA%3d%3d&crl=c&resultLocal=ErrCrlNoResults&resultNs=Ehost&crlhashurl=login.aspx%3fdirect%3dtrue%26profile%3dehost%26scope%3dsite%26authtype%3dcrawler%26jrnl%3d11381728%26AN%3d103452505 [ Links ]
16. Gonçalves, AML, Amorim, FMSB LMB, Almeida, MTG, França, AMB. Trauma em idosos: como deve ser realizado o atendimento. Semina cienc biol saúde (Internet). 2018 (cited 2019 Jan 14); 4(2):77-86. Available from: Available from: https://periodicos.set.edu.br/index.php/fitsbiosaude/article/view/5110/2783 [ Links ]
17. Carpenter CR, Platts-Mil TF. Evolving Prehospital, Emergency Department, and “Inpatient” Management Models for Geriatric Emergencies. Rev Clin Geriatr Med (Internet). 2013 (cited 2018 Nov 11); 29(1):31-47. Available from: https://www.geriatric.theclinics.com/article/S0749-0690(12)00083-3/pdf [ Links ]
18. Gonsaga RAT, Silva EM, Brugugnolli ID, Cabral JL, Thomé Neto O. Padrão e Necessidades de Atendimento Pré-hospitalar a Idosos. Rev Bras Geriatr e Gerontol (Internet). 2015 (cited 2018 Oct 25); 18(1)19-28. Available from: Available from: http://www.redalyc.org/pdf/4038/403839881003.pdf [ Links ]
19. Marques GQ, Lima MADS, Ciconet RM. Agravos clínicos atendidos pelo Serviço de Atendimento Móvel de Urgência (SAMU) de Porto Alegre - RS. Acta Paul Enferm (Internet). 2011 (cited 2018 Nov 11); 24(2): 185-91. Available from: Available from: https://www.lume.ufrgs.br/bitstream/handle/10183/38530/000776233.pdf?sequence=1&isAllowed=y [ Links ]
20. Almeida PMV, Dell'Acqua MCQ, Cyrino CMS, Juliani CMCM, Palhares VC, Pavelqueires S. Análise dos atendimentos do SAMU 192: Componente móvel da rede de atenção às urgências e emergências. Esc Anna Nery (Internet). 2016 (cited 2018 Oct 25); 20(2):289-295. Available from: http://www.redalyc.org/html/1277/127745723012/ [ Links ]
21. Longo MAT, Martelli A, Zimmermann A. Hipertensão arterial sistêmica: aspectos clínicos e análise farmacológica no tratamento dos pacientes de um setor de psicogeriatria do Instituto Bairral de Psiquiatria, no município de Itapira, SP. Rev Bras Geriatr Gerontol (Internet). 2011 (cited 2018 Nov 11); 149(2): 271-84. Available from: http://www.redalyc.org/pdf/4038/403834042008.pdf [ Links ]
22. Silva DM, Vilela ABA, Nery AA, Duarte ACS, Alves MR, Meira SS. Dinâmica das relações familiares intergeracionais na ótica de idosos residentes no Município de Jequié (Bahia), Brasil. Ciênc Saúde Coletiva (Internet). 2015 (cited 2019 Jan 10); 20(7): 2183-91. Available from: http://www.redalyc.org/pdf/630/63039870024.pdf [ Links ]
23. Santos FAA, Souza JB, Arantes DL, Orsi E. Prevalência de dor crônica e sua associação com a situação sociodemográfica e atividade física no lazer em idosos de Florianópolis, Santa Catarina: estudo de base populacional. Rev Bras Epidemiol (Internet). 2015 (cited 2019 Jan 15); 18(1): 234-47. Available from: Available from: https://www.scielosp.org/article/rbepid/2015.v18n1/234-247/en/ [ Links ]
24. Dellaroza MSG, Pimenta CAM, Duarte YA, Lebrão ML. Dor crônica em idosos residentes em São Paulo, Brasil: prevalência, características e associação com capacidade funcional e mobilidade (Estudo SABE). Cad Saúde Pública (Internet). 2013 (cited 2018 Nov 11); 29(2): 325-34. Available from: Available from: https://www.scielosp.org/scielo.php?pid=S0102-311X2013000600019&script=sci_arttext [ Links ]
25. World Health Organization. World health statistics 2016: monitoring health for the SDGs, sustainable development goals. Geneva: World Health Organization; 2016. Available in: http://www.who.int/gho/publications/world_health_statistics/2016/en/ [ Links ]
26. Pereira RA, Santos EB, Fhon JRS, Marques S, Rodrigues RAP. Sobrecarga dos cuidadores de idosos com acidente vascular cerebral. Rev esc enferm USP (Internet). 2013 (cited 2018 Oct 25); 47(1): 185-92. Available from: http://www.scielo.br/pdf/reeusp/v47n1/a23v47n1 [ Links ]
27. Solano JPC, Scazufca M, Menezes PR. Frequência de sintomas no último ano de vida de idosos de baixa renda em São Paulo: estudo transversal com cuidadores informais. Rev bras epidemiol (Internet). 2011 (cited 2018 Nov 11); 14(1): 75-85. Available from: https://www.scielosp.org/scielo.php?pid=S1415-790X2011000100007&script=sci_arttext [ Links ]
Correspondence: Julival Andrade Santos Junior, e-mail: jasjunior@uesb.edu.br. Adriana Alves Nery, e-mail: aanery@uesb.edu.br. Claudio Bispo de Almeida, e-mail: cbalmeida@uneb.br. Cezar Augusto Casotti,e-mail: cacasotti@uesb.edu.br
How to cite: Santos Junior, J.A., Nery, A.A., Almeida, C.B., Casotti, C.A. Profile of elderly service by mobile emergency service. Enfermería: Cuidados Humanizados. 2020; (9): 100-113. Doi: https://doi.org/10.22235/ech.v9i2.2041
Authors' participation: a) Conception and design of the work; b) Data acquisition; c) Analysis and interpretation of data; d) Writing of the manuscript; e) Critical review of the manuscript. J.A.S.J. has contributed in a, b, c, d,e; A.A.N. in a,b,c,d,e; C.B.A. in a, b,c,d,e.; C.A.C. in c,d,e.
Accepted: August 14, 2020; Received: January 23, 2020
 Este é um artigo publicado em acesso aberto sob uma licença Creative Commons
Este é um artigo publicado em acesso aberto sob uma licença Creative Commons
