










Services on Demand
Journal

Article
 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Related links
Share

 Permalink
PermalinkEnfermería: Cuidados Humanizados
Print version ISSN 1688-8375On-line version ISSN 2393-6606
Enfermería (Montevideo) vol.8 no.2 Montevideo Dec. 2019 Epub Dec 01, 2019
https://doi.org/10.22235/ech.v8i2.1845
Original Articles
Clinical Simulation: nursing student´s opinions, Autonomous University of Chile, Temuco
1
 http://orcid.org/0000-0003-0635-5331
http://orcid.org/0000-0003-0635-5331
2
http://orcid.org/0000-0003-2014-9622
1
http://orcid.org/0000-0002-3668-8180
1Universidad de La Frontera. Temuco, Chile monica.illesca@ufrontera.cl
2Universidad Autónoma de Chile. Temuco, Chile
3Escuela de Enfermería, Facultad de Ciencias, Universidad Mayor, Chile
Keywords: Simulation; Students nursing; Education professional; Nursing Education
Palabras claves: Simulación; Estudiantes de Enfermería; Educación Profesional; Educación en Enfermería
Palavras chaves: Simulação; Estudantes de Enfermagem; Educação Profissionalizante; Educação em Enfermagem
Introduction
Nursing student training is a complex and comprehensive process that requires the incorporation of generic competences (instrumental, systemic and interpersonal) and also specific ones such as knowledge, skills, attitudes and values, together with strategies that allow a comprehensive evaluation of the acquired skills. The ultimate goal is to provide the users with efficient humanistic care focused on achieving expected results through the application of the nursing process 1,3. When the history of the teaching-learning process in this career is reviewed, demonstration and feedback of procedures appear from earlier dates, when students learned by themselves techniques to develop skills before attending to patients, trying to preserve patient safety, a fundamental principle of the profession 4.
Nowadays, with advanced technologies, clinical simulation is used, allowing the interaction of knowledge, skills and human factors in order to provide effective training so students can develop skills to achieve competencies, granting the opportunity for a practice similar to what will happen in reality 5. Learning through clinical simulation gives a clear answer to the need to protect patient safety, playing a very important role in favor of the ethical principle of “non-maleficence”, safeguarding the rights and duties of the user, since it is not performed on real patients or anyone in critical condition 6,7.
Simulation is a dynamic process that involves the creation of a hypothetical opportunity that incorporates an authentic representation of reality, facilitating the active participation and commitment of the student and integrating the complexity of practical and theoretical learning with the possibility of repetition, feedback, evaluation and reflection 8. It is also defined as the recreation of a scenario designed to experience the representation of a real event in order to practice, learn, evaluate, test or acquire knowledge of human systems or actions, or any teaching activity that uses the help of simulators to stimulate and favor the process of learning, imitating as much as possible a more or less complex clinical scenario 9,11. This responds to the concept of meaningful learning based on experience, where the student-centered educational model is supported, also considering that the motivation of the student, during his academic training, is the practical application of the object of study12,13. This requires the teacher to acquire new skills to carry out this methodology, such as the design of scenarios, proper execution and evaluation, under a conception of learning that puts the activity of the student in focus 14. Simulation learning can be divided into three levels of difficulty: low fidelity, carried out in models that allow to practice basic techniques; intermediate, which groups skills that require a level of integration with each other, and high fidelity, which uses interactive technologies that represent reality15. This implies designing appropriate scenarios, becoming a tool with great teaching potential16.
The evaluation of the student's competences in this way is continuous through a session with scenarios unknown to him, which allows assessment in three aspects: observation of the instructor, of a group of students and self-assessment 4. The highlight of teaching by simulation is debriefing, which consists of the self-critical review of all the actions carried out during a clinical experience, led by a physician. It is also expressed as the conversation between several people to review a real or simulated event, in which participants analyze their actions and reflect on the role of thought processes, psychomotor skills and emotional states to improve or maintain their performance in the future 17,18. Hence the importance of debriefing so that the student, in addition to developing specific skills in the profession, acquires generic skills, including self-criticism, learning to learn, critical thinking, ability to analyze, among others. Simulation in general, and high fidelity in particular, although it involves the use of numerous resources, enjoys great acceptance among students and instructors, meets all phases of the acquisition of experience and is the option to practice the necessary skills before critical situations. Various publications prove the relevance of clinical simulation in the training process. Many of them highlight the acquisition of generic skills: greater autonomy, self-efficacy and locus of internal control, trust, teamwork, communication, significant improvement in interpersonal communication skills, interviews and counseling; it increases opportunities for reflection and the acquisition of self-confidence after clinical simulation experience 5,19,23.
In relation to discipline, students achieve an important skill, apply and integrate the acquired knowledge into the clinical experience, associate the task with previous experiences, use sensory information, test their own techniques performed in a practical way reflecting on an action, effectively training prior to clinical care 19,2,22,5. At the same time, it allows the realization of clinical trials in the field of safe practices, execution of invasive diagnostic procedures and nursing complexes, in addition to the development of attitudes such as professional and interdisciplinary responsibility in-patient, family and community care 4. This methodological strategy, the clinical simulation, requires that the curriculum implements protocols that guarantee the reproduction of scenarios to be incorporated gradually throughout the career; thus the student becomes familiar with them, since the confrontation with unknown technologies can enhance the clinical ability. It is important that there is adequate teacher training, which is as close to reality as possible, a sufficient number of practices of the technique that need to be learned, with the corresponding clinical simulation evaluation guidelines 19,20,24. It is important to clarify that the key to success is not only to have high-tech equipment and models, but rather to ensure that teachers are trained in this pedagogical strategy by implementing a model to develop clinical judgment, safeguarding a close collaboration between teachers and students 4,25. As a way to maximize the experiences, it is necessary to create a culture of clinical simulation, as well as to plan and organize them so that they guide the activities of the study plan, according to the level of complexity that the learner finds 4.
Likewise, evaluation constitutes a fundamental tool, because it allows the rectification of errors and increases the degree of realism in the staging of cases. However, there is evidence that the students express their disagreement by suggesting an improvement in the acquisition of real and less simulated material, since performing certain nursing techniques (arterial gasometry, channeling of central peripheral insertion catheters, etc.) in the dummy results sometimes too unreal despite the advanced simulators 5. Work has also been carried out in the field of pediatrics, where nursing students express that it increases self-efficacy and reduces the level of anxiety; they acquire greater confidence, demonstrating as a consequence that higher self-confidence scores represent an increase in the quality of patient care 26,27.
In this context, the Faculty of Health Sciences of the Autonomous University, Temuco, Chile, conducted training in July 2016 in Clinical Simulation to teachers of the Pediatric Area of the Nursing Career, in order to include it in the second semester of the same year, which was incorporated into the Pediatric and Adolescent Medical Nursing Laboratory. Being a first experience and with the goal of contributing to the implementation of this strategy in the training process, it is important to know the opinion of the students about the experience. The objectives are oriented to explore its meaning, the factors that affect it, what they felt when experiencing it and the acquisition of generic skills and the nursing process as disciplinary competence.
Methodology
The exploratory and descriptive qualitative research paradigm is chosen, from the methodological perspective of an intrinsic case study, whose purpose is aimed at describing important aspects of a little known phenomenon and documenting it 28.
The experience was carried out with 90 fourth-year students attending the Pediatric and Adolescent Medical Nursing Laboratory credit in the second semester of 2016. Clinical simulation activities were organized so that all students could acquire skills before attending the patients in the care practice. Two activities of low difficulty level of one hour of duration were carried out, oriented to the control of vital signs-anthropometry and admission in pediatric patients; and four more of medium fidelity, of two hours each, designed for the management of care in pediatric patients with Sepsis, Infection of the Urinary Tract, Respiratory Virosis and Respiratory Depression. The situations were programmed in order to evaluate the skills of knowing, knowing how to do and knowing how to be. After the execution of these activities, the feedback process was carried out with a specific guideline. Two teachers participated, with previous training.
The sample, not probabilistic, intentional of cases by criterion and convenience, was made up of 15 participants, whose inclusion criteria were: fourth year students in 2016 of the Nursing Career of the Autonomous University of Chile, enrolled in the Pediatric and Adolescent Medical Nursing Laboratory, with availability and acceptance to participate voluntarily after signing the Informed Consent 29.
For the data collection, the focus group technique was used (a group of 7 and another of 8 members), which were collected until reaching the saturation point, that is, by repetition of ideas; or, to gather sufficient evidence to guarantee the credibility of the investigation 30. A guideline was used to ensure that all subjects were explored and audio recorder and field notes were used to collect all the information, with the corresponding authorization. The data analysis followed the constant comparison scheme, not grouping into predetermined categories, but rather emerging from an inductive reasoning process, through a generative and constructive method in which the inductive coding of categories was combined with the constant comparison of them 31. Progressively the reduction of the information consistent with the object of study was carried out through three phases that formed different types of operations, segmentation and codification of units of meaning, identification of the main themes or emerging thematic nuclei and integration and interpretation of the results in qualitative domains, structured through three levels, which was performed manually by the researchers 32,33:
Level 1: Identification of units of meaning and segmentation of them for grouping into descriptive categories.
Level 2: From the descriptive categories, a system of emerging thematic nuclei or metacategories was constructed.
Level 3: As a consequence of the previous level, qualitative domains were identified through a sequential and cross-sectional analysis of metacategories.
It should be noted that under this paradigm data collection and analysis was concurrent 34. The categorization and segmentation were two operations executed simultaneously because the criterion used was belonging to a certain concept or topic, where the units that referred to a certain idea were included in the corresponding categories. Scientific rigor was determined by four criteria: credibility (triangulation by researcher, verification with study participants), applicability or transferability (abundant collection of information and detailed description), consistency or dependence (step-by-step replication), and neutrality or confirmability (consensus with other researchers, expert critical judgment) 35. The validation was carried out using the triangulation technique by researchers 28.
The ethical considerations were protected because it was a Project authorized by the Ethics Committee of the Autonomous University of Chile 36. The ethical principles in research were worked on: social value, because the results will allow probable social and scientific benefits; the scientific validity through a rigorous design, whose products were also triangulated by researchers, without the participation of teaching nurses involved in the subject where this research was carried out; the equitable selection of subjects was protected by identifying the key informants, that is, those who contributed to the study since they were directly related to it; the favorable risk-benefit ratio focused on minimizing potential risks and increasing benefits proportionally was met respecting the principles of non-maleficence and beneficence, without any conflict for the participants; the independent evaluation refers to the non-distortion of the research product of the interests of the authors, which was endorsed by the Ethics Committee of the University; the informed consent, sanctioned by said Committee that included respect for a voluntary and conscious participation of the subjects, offering them the opportunity to ask questions, doubts and withdraw from the study if they wished; respect for the enrolled subjects through the possibility of changing their minds, ensuring confidentiality of the data and delivery of the study results 37.
Results
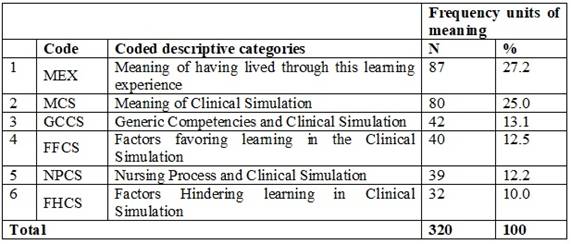
Level 1: 320 units of meaning relevant to the study were revealed, grouped into 6 emerging categories, which can be seen in Table 1.
As a result of this process, each of the six emerging categories is presented in Table 2, Table 2 (continuation).
Table 2: Frequency distribution of the units of meaning of the six emerging categories
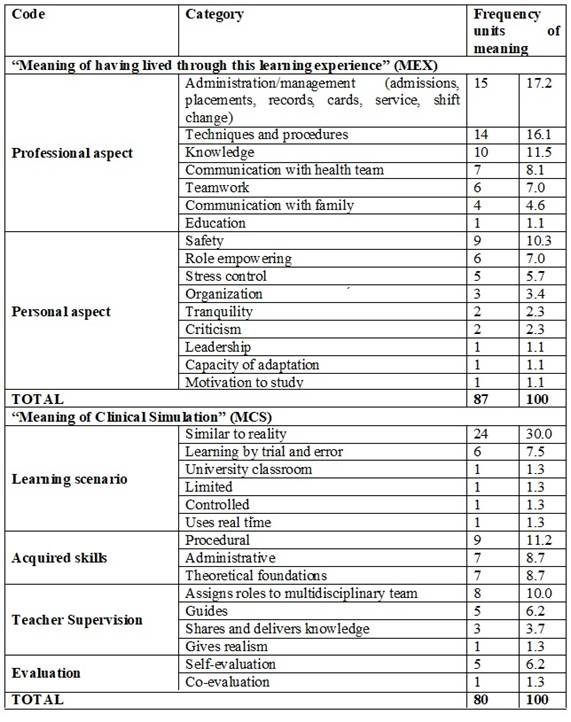
Source: Personal Collection (2018)
Table 2: (continuation) Frequency distribution of the units of meaning of the six emerging categories
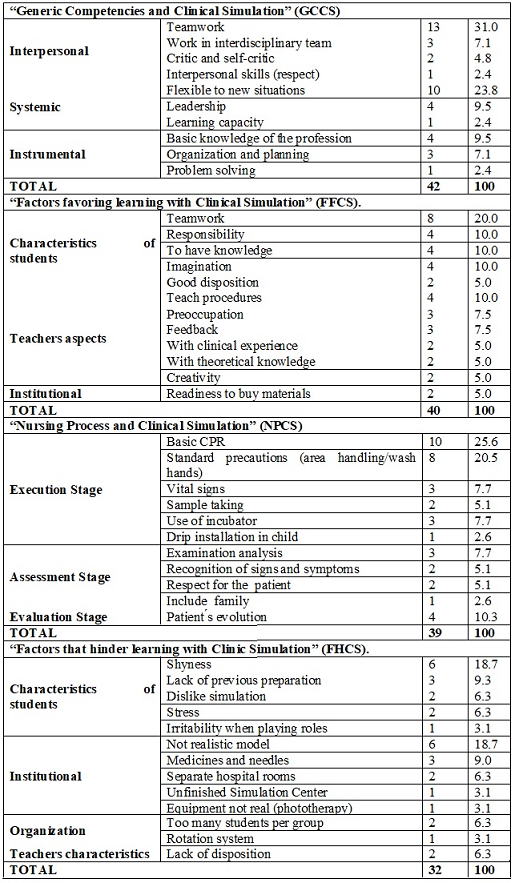
Source: Personal Collection (2018)
1. Experience of the students of the Nursing Career in relation to the Clinical Simulation: perception around the concept and experience as a learning strategy in their professional training in the Nursing Career (MEX - MCS). 2. Factors that facilitate and hinder learning with Clinical Simulation: appreciation in relation to aspects that contribute and hinder learning, related to aspects of students, teachers, supplies, infrastructure and organization of the activity (FFCS - FHCS). 3. Skills developed in nursing students, through Clinical Simulation: opinions linked to specific competencies within the nursing and generic processes (instrumental, systemic and interpersonal) (NPCS - GCCS).
1. Contributions of nursing students to implement the Clinical Simulation: it represents the opinions in relation to the experience that allowed them to conceptualize it and identify concurrent factors in its application (MEX - MCS - FFCS - FHCS). 2. Contribution of the Clinical Simulation as a learning strategy for the development of disciplinary and generic competences for its future professional performance: it evidences the assessment regarding the development of the nursing process as disciplinary and generic competences (instrumental, systemic and interpersonal) (NPCS) - GCCS).
Discussion and Final Considerations
In Level 1, the units of meaning for the first two categories "Meaning of having lived through this learning experience" and "Meaning of Clinical Simulation" with 27.2% and 25% respectively, reflect the relevance of the topic within training of key informants. The first one shows, as in other studies, two major aspects: a professional one (knowledge acquisition, techniques, procedures and administration / management and education functions and other personnel) 4,5,22, and another one, personal, the achievement of generic skills 5,20,21,23. The second category coincides with what is stated in the literature, stating that these are learning scenarios in which knowledge is acquired supervised by a teacher and where the evaluation of both process and result is applied 4,5,8. This reflects how significant it is to work with this learning strategy: without having a theoretical class of Clinical Simulation, they managed to define it only with its development.
In relation to “Generic Competences and Clinical Simulation”, findings were classified according to Tunning 1 in Interpersonal, Systemic and Instrumental. When identifying them it is observed that only teamwork is assimilable with another study 5. Skills such as autonomy 19 , self-efficacy 20 , communication 21 and reflection 22 do not emerge in the discourses; however they do identify respect, adapting to new situations, leadership, ability to learn, organize, plan and resolve problems, which could be explained by the fact that in these studies another type of generic competence classification was used. Also, it should be considered that the students were subjected to a new learning situation and evaluation process. In any case, the findings are relevant since the current educational guidelines aim to strengthen these qualities as a factor of human capital 2.
Regarding the "Nursing Process and Clinical Simulation", three stages are identified, assessment, execution and evaluation, execution being mostly recognized; the undeclared ones, diagnosis of needs and planning, is probably due to the low level of difficulty of the clinical simulation scenarios, taken into consideration by the teachers for this first experience as a way of gradually rehearsing the methodology 3,15. The key informants consider the application of the Nursing Process, reaffirming that at their curricular level they are clear about what they can integrate in relation to the degrees of difficulty that are presented to them for their learning.
Regarding the category “Factors that favor learning with Clinical Simulation”, three aspects emerge; characteristics of students, teachers and Institution, recognizing the first one as the most relevant with 22 units of meaning, highlighting teamwork, very important as a generic competence. What emerges about the opinions of teachers is described by Quiroz and Vargas, who argue that they must be trained in relevant pedagogical aspects and be concerned and creative at the time of carrying out the educational action 4. Regarding the provision of materials by the Institution, they indicate only two units of meaning in the same sense as that proposed by Juguera, Díaz, Pérez et al., regarding simulators closer to reality 5.
Regarding the category “Factors that make learning difficult”, they are mainly related to the personal characteristics of the students, which could be reduced if this methodology was gradually incorporated throughout the course 20. Regarding the Institutional factor, the informants refer to insufficient means, non-real symptoms and infrastructure not appropriate for these effects, which is consistent with the study by Juguera, Díaz, Pérez et al. where the students suggested an improvement in the acquisition of more realistic material 5. Likewise, they find that in the organization of the activity the number of students should be reduced to facilitate the process by planning and organizing it according to the growing complexity of the study plan and protocols that guarantee the reproduction of scenarios, in order to gradually establish a culture of clinical simulation considering also the collaboration between teachers and students 4,19,25.
Finally, we must point out that the information obtained in this study is consistent with that shown by several authors mentioned above, in the sense that it is a relevant strategy when integrating knowledge and skills, that previous experience is an important aspect when executing this methodology, reduces the gap between theory and practice, strengthens generic competencies and allows the student to assume responsibility in their training
REFERENCES
1. Tuning Educational Structures in Europe. Informe Final Proyecto Piloto-Fase 1. Bilbao: Edición y Cultura. Sócrates. 2003. [ Links ]
2. Barrios S, Masalán P, Cook MP. Educación en Salud: en la búsqueda de metodologías innovadoras. Cienc. Enferm. 2011; 17(1): 57-69. [ Links ]
3. Alfaro-Lefevre R. Aplicación del proceso enfermero: fomentar el cuidado en colaboración. Quinta Edición. México: Masson. 2003. [ Links ]
4.Quirós S, Vargas A. Simulación clínica: una estrategia que articula prácticas de enseñanza e investigación en Enfermería. Texto & Contexto - Enferm. 2014; 23 (4): 815-816. [ Links ]
5. Juguera L, Díaz J, Pérez Mª L, Leal C, Rojo A, Echevarría P. La simulación clínica como herramienta pedagógica: percepción de los alumnos de Grado en Enfermería en la UCAM (Universidad Católica San Antonio de Murcia). Enfermería Global. 2014; 13 (33): 175-190. [ Links ]
6. Ministerio de Salud de Chile (MINSAL, 2016). Ley de Derechos y Deberes del Paciente N°20.584 2019 may. 15. Disponible en: http://www.ssmso.cl/tmpArchivos/participacion/Escuelas/Leyes/Ley%20de%20Derechos%20y%20Deberes%20de%20los%20pacientes%20Superintendencia%20de%20Salud.pdf [ Links ]
7. Galindo J, Visbal L. Simulación, herramienta para la educación médica Simulation, a teaching aid for medical education. Salud Uninorte. Barranquilla (Col.). 2007: 23(1): 79-95. [ Links ]
8. Bland A, Topping A, Wood B. A concept analysis of simulation as a learning strategy in the education of undergraduate nursing students. Nurse Education Today. 2011; 31(7): 664-670. [ Links ]
9. Del Moral I, Díaz de Terán J, Rabanal J, Quesada A, Rodríguez J, Teja J, et al. Nuevos procedimientos de entrenamiento en el manejo de crisis y emergencias médicas. En Procedimientos técnicos en urgencias y emergencias. Editores Quesada A, Rabanal JM, editores. Madrid 2003 pp; 479-86. [ Links ]
10. De la Horra I. La simulación clínica como herramienta de evaluación de competencias en la formación de enfermería. Reduca (Enfermería, Fisioterapia y Podología). Serie Trabajos Fin de Máster. 2010; 2(1): 549-580. [ Links ]
11. Ziv A. Simulators and simulation-based medical education, en Dent, J. y Harden, R.M. (eds.) A Practical Guide for Medical Teachers, Edinburgh; 2009. P 217-222. [ Links ]
12. Ausubel D, Novak J, Hanesian H. Psicología educativa. Un punto de vista cognitivo. Segunda Edición. México: Trillas; 2000. [ Links ]
13. Dewey J. Experiencia y educación Libro de John. Estados Unidos: Kappa Delta Pi; 1938. [ Links ]
14. Ruiz M. Enfoque integral del currículo para la formación de profesionales competentes. México: Instituto Politécnico Nacional; 2000. [ Links ]
15. Vázquez-Mata G, Guillamet-Lloveras A. El entrenamiento basado en la simulación como innovación imprescindible en la formación médica. Educ Med. 2009;12(3): 149-155. [ Links ]
16. Velazco-Martín A. Simulación Clínica y enfermería creando un ambiente de simulación (Tesis de Grado). Universidad de Cantabria. Disponible en https://repositorio.unican.es/xmlui/bitstream/handle/10902/3949/VelascoMartinA.pdf. 2013. [ Links ]
17. Maestre J, Manuel-Palazuelos J, del Moral I, Simond Robert. La simulación clínica como herramienta para facilitar el cambio de cultura en las organizaciones de salud: aplicación práctica de la teoría avanzada del aprendizaje. Rev colomb. Anestesiol. 2014; 42(2): 124-128. [ Links ]
18. Maestre J, Rudolph J. Teorías y estilos de debriefing: el método con buen juicio como herramienta de evaluación formativa en salud. Rev Esp Cardiol. 2015;68(4): 282-5. DOI: 10.1016/j.recesp.2014.05.018 [ Links ]
19. Niño CA, Vargas NG, Barragán JA. Fortalecimiento de la simulación clínica como herramienta pedagógica en enfermería: experiencia de internado. Rev Cuid. 2015; 6(1): 970-5. http://dx.doi.org/10.15649/cuidarte.v6i1.161 [ Links ]
20. Barrios S, Urrutia M, Rubio M. Impacto de la simulación en el desarrollo de la autoeficacia y del locus de control en estudiantes de enfermería. Educación Médica Superior. 2017; 31(1):125-136. [ Links ]
21. Ching-Lan E, Shiah-Lian Ch, Shu-Yuan Ch, Yueh-Chih Ch. Using standardized patient with immediate feedback and group discussion to teach interpersonal and communication skills to advanced practice nursing students. Nurse Education Today. 2013; 33(6): 677-683. [ Links ]
22. Johannesson E, Silén Ch, Kvist J, Hult H. Students’ experiences of learning manual clinical skills through simulation. Adv in Health Sci Educ. 2013; 18(1):99-114. [ Links ]
23. Tagwa O. Nursing Students’ Perceptions of Satisfaction and Self-Confidence with Clinical Simulation Experience. Journal of Education and Practice. 2016; 7(5): 131-138. [ Links ]
24. Ruiz S. Simulación Clínica y su utilidad en la mejora de la seguridad de los pacientes. Trabajo Fin de Grado. 2012. Departamento de Enfermería, Universidad Cantabria. Disponible en http://www.asepur.org/wp-content/uploads/2014/06/Simulacion-Clinica-y-su-utilidad-en-la-mejora-de-la-seguridad-de-los-pacientes.pdf [ Links ]
25. Zhang J. Perceptions of simulation-assisted teaching among baccalaureate nursing students in Chinese context: Benefits, process and barriers. Journal of Professional Nursing. 2017; 33(4): 305-310. [ Links ]
26. Tas F, Sonay A, Celen R, Özkan S, Altıparmak D, Sahin A. Comparing Traditional and Simulation-Based Experiences in Pediatrics with Undergraduate Nursing Students in Turkey. Clinical Simulation in Nursing. 2018; 16: 62-69. [ Links ]
27. Lubbers J, Rossman C. The effects of pediatric community simulation experience on the self-confidence and satisfaction of baccalaureate nursing students: A quasi-experimental study. Nurse Educ Today. 2016; 39: 93-98. [ Links ]
28. Latorre A, Del Rincón D, Arnal J. Bases metodológicas de la investigación educativa. Barcelona: Hurtado; 1999. [ Links ]
29. Polit D, Hungler BP. Investigación Científica en Ciencias de la Salud. Sexta Edición. México: Mc Graw- Hill; 2000. [ Links ]
30. Martínez-Salgado C. El muestreo en investigación cualitativa: principios básicos y algunas controversias. Ciênc. Saúde Coletiva. 2012; 17 (3): 613-9. http://doi.org/b9qn. [ Links ]
31. Glaser BG, Strauss AL. El método de comparación constante de análisis cualitativo. In The discovery of Grounded Theory: strategies for qualitative research New York: Aldine; 1967. P 45-77. [ Links ]
32. Gil-Flores J, Perera-Rodríguez VH. Análisis informatizado de datos cualitativos. Sevilla: Kronos; 2001. [ Links ]
33. Miles MB, Huberman AM. Qualitative data analysis: A sourcebook of new methods. Beverly Hills: Sage; 1984. [ Links ]
34. Latorre A. La investigación-acción: conocer y cambiar la práctica educativa. Barcelona: Graó; 2003. [ Links ]
35. Guba EG, Lincoln YS. Naturalist Inquiry. London: Sage; 1985. [ Links ]
36. Universidad Autónoma de Chile. Acta de Evaluación N° 0131-16. 2016. [ Links ]
37. Lolas F, Quezada A, (eds.). Pautas éticas de investigación en sujetos humanos: nuevas perspectivas. Chile: Programa Regional de Bioética OPS/OMS; 2003. [ Links ]
Received: March 04, 2019; Accepted: July 04, 2019
 Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
