










Servicios Personalizados
Revista

Articulo
 texto en
texto en  Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
Links relacionados
Compartir

 Permalink
PermalinkEnfermería: Cuidados Humanizados
versión impresa ISSN 1688-8375versión On-line ISSN 2393-6606
Enfermería (Montevideo) vol.7 no.1 Montevideo jun. 2018
https://doi.org/10.22235/ech.v7i1.1537
Original Articles
Humanized care and psychosocial risks: a relationship perceived by professional nurses in Chile
1Universidad Católica del Maule. Talca, Chile. 140) sramos@ucm.cl
2Universidad Católica del Maule. Talca, Chile
Key words: Humanization of the attention; work-related risks; Nursing Care; Nursing
Palabras clave: Humanización de la Atención; Riesgos Laborales; Atención de enfermería; Enfermería
Palavras-chave: Humanização da Atenção; Riscos no Trabalho; Atenção da enfermagem; Enfermagem
Introduction
Nursing is the science and the art of caring for the health of the individual, family, and community. Its field of action includes the promotion and maintenance of health, the prevention of diseases and the participation in their treatment, including the patient’s rehabilitation, regardless of the stage of growth and development 1. Experts indicate that one of the main objectives of nursing is to maintain the highest physical, mental, social, and spiritual well-being of the human being through care, considered the essence of the profession, built by transpersonal and intersubjective actions to protect, improve and preserve humanity 2. However, this caring apparently has been getting more and more dehumanized. It is not unusual to observe in the daily practice that patients are recognized by their bed number or their pathologies; the needs that they mention are not taken into account, among other aspects. One of the main reasons is that in the health system there is still a biomedical perception. The objective is to cure the disease, leaving aside the patient’s social, family, and emotional environment 3.
Many dehumanized situations are found in the practice; it is important to identify the causes related to these behaviors in order to intervene and improve the cure provided. One of these reasons may be the work related psychosocial factors present in health institutions, which, when perceived as negative, may affect the health of the worker when they become psychosocial risks 4. These risks could affect somehow the quality of the work performed and the quality of care given by the nurses.
In Chile and all over the world these psychosocial risks have generated an increase in mental health problems in workers of all the services field; in this case, health care workers. These risks are related with the new ways of organizing production, labor relations, the computer revolution and the massive introduction of new technologies, resulting in intensification of the workload, excessive physical and mental demand, weakening of labor collectives and erosion of the limits between work and personal life. These new ways of organizing work stresses the worker emotionally and cognitively, increasing their psychical and mental workload 5. Reviewing existing literature shows that there are several theorists supporting studies related to psychosocial risks, but their relationship with the perception of care has been studied just at a qualitative level. The two theoretical models that follow attempt to explain these risks. The first one is the Karasek and Theorell proposal, linking three concepts, “demand-control-social support” 6)(7. Psychological demands are at the mental level. This refers to how much one works: work volume, time pressure, attention level, unexpected interruptions; they are not confined to intellectual work but to any type of task. The model predicts, first, stress related risk of illness; second, it predicts a relationship with active/passive behavior. These two main psychological mechanisms, psychological tension and learning, are independent, which is one of the essential features of the model: its two-dimensional structure 8.
The second theory was proposed by Siegrist, who developed the model “Effort-reward imbalance”; it states that the role of work in adulthood is to link self-regulating functions, such as self-esteem and self-efficacy with the structure of social opportunities 9. This means that the professional and occupational category of the worker is associated to a certain level of retribution and realization: to be rewarded or appreciated, and to significantly belong to a group. Therefore, demands are always present in the workplace and can generate feelings of anxiety, fear, tension, or threat arising during the activities and requiring adaptive responses, which are not always adequate and may become a labor risk 10.
When performing health care, a nurse-patient relationship is established, generating affection, concerns and responsibilities for both of them, uncovering the human side, bringing out values and principles. Professional care is synonymous of humanized care 11. Humanized care has been widely developed by the nursing theorist Jean Watson, who recognized that caring is the fundamental part of being, and is the most primitive act that a human being performs effectively to be in a relationship with another human being that invokes him or her 12. This call from the other, absolute other, is the fundamental foundation of care. This care is structured, formalized, and destined to satisfy the needs of the human being with the purpose of promoting, maintaining, or recovering his/her health 13. Watson states that, faced with the risk of dehumanization of patient care due to the great administrative restructure in most systems in the world, it is necessary to rescue the human, spiritual, and transpersonal aspects in the clinical, administrative, educational, and research practice from nursing professionals. Watson requests that the current nursing practices be improved and provides a disciplinary framework to work with in the daily practice of nursing, seeing the patient from a transformative and integral perspective, moving away from the biomedical model 2.
Therefore, delivering humanized care must be a priority in nursing. It is a profession where one must start with self-knowledge. In addition, it demands a constant reflection on human interaction problems from an ethical, social and political point of view. In this regard, some authors indicate that the society requires this type of care, based on a humane relationship among the participants in the act of caring 14. However, this context, although positive for the patient, can generate occupational risks in professionals. Nurses should know that working with human beings, added to the labor factors that are present in the working environment can affect their physical, mental, or social health, and this can affect the quality of the care given. Consequently, the care given will be of inferior quality, not only in the procedures but also in the way they deal with the patient, which is reflected in dehumanization. Therefore the problem is that the impact that psychosocial labor risks can have on the perception of delivering humanized care by nursing professionals in a public hospital in Chile is unknown. This study has the purpose of evaluating whether there is a relationship between psychosocial risks at work and the delivery of humanized care by the nurses of that hospital.
Methodology
The design of this investigation was non-experimental, cross-sectional, and correlational with a quantitative approach 15. In all the stages of this investigation the ethical principles of Emanuel were respected 16. The data was taken in a public hospital in the Maule Region of Chile between November 2016 and January 2017. The population for this study was obtained through an effective census. Out of the total population of 325 nurses a target population of 258 workers was obtained (the ones who met the inclusion criteria established for this investigation). From this group, 240 were registered for the census, so that the study population corresponds to 93% of the target population. The inclusion criteria were: to be a certified nurse, that works formally (contract, replacement, indefinite), performing care functions, providing direct care to patients and that signed the informed consent, giving authorization to the researcher. The exclusion criteria were: that he/she performed mostly administrative or management tasks, to be on vacation or leave of absence when the data is collected and to be performing tasks with patients with serious mental disorders.
The data collection was carried out after the approval by the Ethics-Scientific Committee of the Universidad Católica of Maule and Health Services of Maule. It began with the reading and delivery of the informed consent, which had to be signed, and a copy was given to the participant. They were informed of the time required for the implementation of the instruments, and then they answered. The implementation was done by the main researcher in order to answer any questions or doubts regarding the instruments. The instruments used for the collection of data consisted in three parts. Part I (Instrument A): “Personal and work record”, created by the researchers, with which the bio-sociodemographic variables and labor data were collected. Part II (Instrument B): “Evaluation questionnaire of psychosocial risks on the job SUSESO-ISTAS 21”. This instrument resulted from the adaptation, validation, and standardization of the ISTAS 21-COPSOQ Method in the population of Chilean workers. The School of Public Health of the Universidad of Chile carried out this procedure in 2008, obtaining a Cronbach’s alpha coefficient higher than 0.80, showing an adequate internal consistency 17. Part III (Instrument C): Nyberg’s Caring Assessment (NCA), developed in 1990 by Jan Nyberg during his doctorate at the Colorado University The version used in the present study is the one translated and validated by Margarita Poblete, Doctor of Nursing, with Chilean population, with a Cronbach’s alpha coefficient of 0.82 18.
The data was processed and analyzed using the SPSS program version 18. An exploratory analysis of the data was performed through descriptive statistics, using the method of frequency tables, measurements of central tendency and variability. Then a statistical analysis was performed with a 95% confidence, for which non-parametric statistics (Chi-square and a classification tree) were used.
Results
Among the personal variables, it was observed that regarding age, nurses are 31.46 years old in average, 60% of them being 23 to 30 years old. Regarding the participants’ sex, 82.9% are females. 67.1% reported having a partner, and regarding to the variable children, 62.9% do not have any. On the other hand, the work variables show that the participating workers report an average of 4.9 years of seniority in the workplace. Specifically, 56.7% have between 1 to 5 years of seniority, followed by 17.5% with 6 to 10 years and 15.8% with less than one year of experience. In relation to the hiring grade, a high percentage was in grade 15, corresponding to 45.8%, followed by grade 14 with 24.6%. In the contractual situation with the company, the majority, 85.8%, are hired for a fixed term (contract). In relation to the work schedule, 73.8% work during the fourth shift; in addition, 87.1% only work for the hospital and 17.5% have postgraduate studies.
In Table N° 1 of psychosocial risk levels, it can be observed that in the Psychological Requirements dimension, 57.1% perceived a high exposure risk. In the active work dimension and development of skills, 46.7% perceived a medium risk. In the social support in the company and leadership quality dimension, 47.5% perceived a high exposure risk. In the compensations dimension 43.3% perceived a medium risk. In the double presence dimension, 55% perceived a high risk.
Table N°1: Psychosocial risk levels perceived by nurses participating in this study
Source: Personal Collection (2017)
In Graph N° 1, it can be observed that in relation to the perception of the delivery of care, the participants reported a high delivery of humanized care (51.67%).
In Graph N° 2, it can be seen that the association to the active work dimension and development of skills and perception of humanized care is significant (p=0.033), and it can be observed that the perceived levels of exposure to low psychosocial risk in this category, a high perception of the delivery of humanized care was reported.
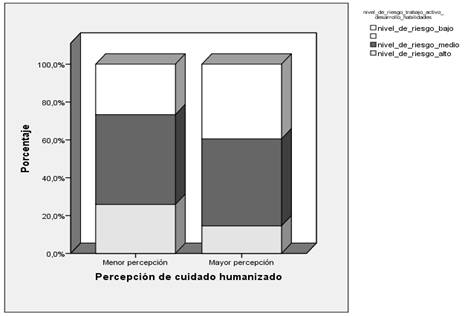
Graph N° 2: Association between the active work and development of skills dimension and the humanized care perceived by the nurses participating in this study
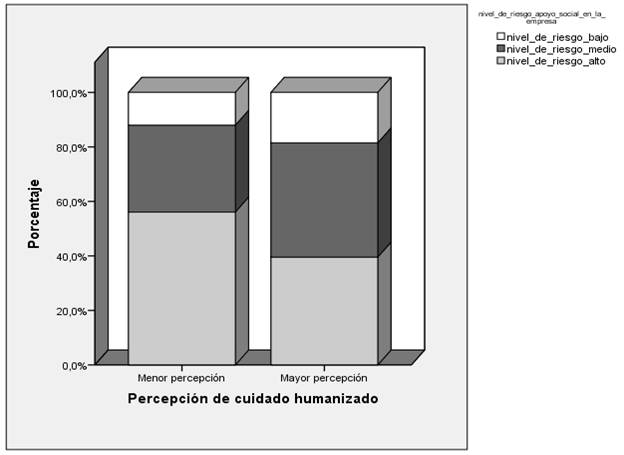
In Graph N° 3, it can be seen that the association of the social support dimension and the leadership quality and perception of humanized care is significant (p=0.035), noting further that participants in this study that perceived levels of exposure to higher psychosocial risks in this category, report a low perception in delivery of humanized care.
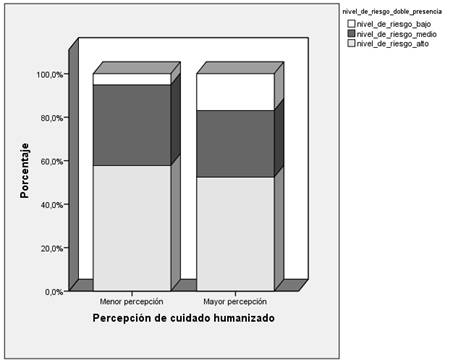
In Graph N° 4, it can be seen that the association of the double presence dimension with humanized care is significant (p=0.015). This result indicates that the participants of the study perceived a high delivery of humanized care.
Discusión
The results of the exposure levels to psychosocial risks analyzed from the Demand-Control-Social support model of the participating nurses show the perception of a very demanding job, reporting high exposure in the psychological requirements dimensions and a low perception of control over what they do 7. In addition, a medium risk level in the active work dimension and development of skills was perceived; a high stress work level is perceived according to this theory. Experts indicate that the buffer that allows to cope with a high stress job is social support, but in the present study, the perception of risk in this dimension is also high, so it becomes a job with high risk that can generate health problems on these workers. The results from the other study are similar, where professionals believe that they do not have the skills to execute certain tasks and to handle some situations in their work. They were more susceptible to mental health conditions 19. On the other hand, the results of this study are opposite to those found by Díaz and Mauro, where health professionals reported a high demand job, but at the same time, a high control and high social support 15. The results under the perspective of the effort-reward model were analyzed, and it was observed that the nurses mainly perceived a medium risk in the compensations dimension and a high risk on psychological requirements. This can generate an imbalance in the worker’s motivation, exposing them to emotional anguish, and therefore, to physical or mental disorders associated with their work 9. 215) In relation to the psychosocial risk dimensions, it is observed that in the psychological requirements and double presence dimensions, the participant workers perceived a high exposure to risks and in the active work and development of skills and compensations dimensions perceived a medium level of exposure to risks. These results are similar to those found by Ceballos et. al., where also applied SUSESO ISTAS-21 questionnaire in a population of nurses of critical units in the south central area of Chile 20. Contradicting the findings made by Moncada et. al., where low scores were reported in the dimensions of double presence and emotions, where the participants were a salaried population from different areas 20)(21. It is emphasized that the daily work of nurses requires contact with a third party, a task with high associated responsibilities; in addition, the majority of the participant workers are females, therefore fulfilling a double social function (worker/housewife). 216) The results obtained in the perception of humanized care indicate that a high percentage of nurses perceive a high delivery of humanized care, despite finding a high level of psychosocial risk perception. This result can be sustained from Watson´s theory 2, who points out that care is a special type of relationship that transcends time and space and continues as part of the larger complex pattern of life in the nurse and the patient. These results show that despite the difficulties of the job, the nurses perceive that they are providing a quality care according to the caritas processes proposed by Watson. Empirically, the results of this study are similar to those reported by other authors, where humanized care is reflected in the act if caring for, serving and treating the patients with affection, but also highlighting that job satisfaction is an important goal to achieve proper care 22. Despite finding more than 50% with a high perception of humanized care, the percentage that presents a low perception is lower: 43.75%. This result is similar to that obtained in other investigations, where it is emphasized that nurses have a clear theoretical meaning of care, but it is difficult to put it into practice due to different factors, such as the organization of the institution, hospital routines, among others that could be associated with the perception of psychosocial risk factors 23)(25. 217) The results obtained when looking for an association between the perception of delivery of humanized care and the psychosocial risks are that the Active work and development of skills, Social support in the company and leadership quality, Compensations and Double presence dimensions present an inversely significant association with the perception of humanized care reported by the workers participating in this study. The nursing professional perceives a high exposure to psychosocial risks and the delivery of low quality humanized care. These results are similar to other studies where the working conditions of nurses were analyzed, concluding that the deficit of human resources, work overload, poor training, low economic retribution and therefore, precarious working conditions, were identified as obstacles to exercise quality care 26)(28. Therefore, having healthy work environments should positively influence care. Considering this, as a nursing unit, it should face the labor problem and strive for healthier work environments, since nurses would have the final impact of the quality of care delivery to the patients, which would then improve the public health of our country.
Conclusions
It can be concluded that psychosocial risks are related to the perception of humanized care, finding a significant association in three dimensions. Thus, the greater the perception of psychosocial risk, less delivery of humanized care. At a professional level, nurses must face the problems regarding work environments, fighting for healthier work environments, thus avoiding high exposure to psychosocial risks and thus improving the quality of the care delivered.
Acknowledgment
The Internal Project postgraduate thesis line 43510, dependent on the Department of Research and Postgraduate of the Catholic University of Maule, financed this work. Part of this article is derived from the Master’s thesis entitled Perception of the Humanized Care delivery by the nursing professionals in relation to psychosocial factors, of the Nursing Master’s Program at the Catholic University of Maule, Chile.
REFERENCES
1) CPE Puerto Rico. Reglamento de la junta examinadora de enfermeras y enfermeros de puerto rico para la implantación de la ley número 9, 1984. Disponible en: http://cpepr.org/images/PDF/REGLAMENTO%205069.pdf [ Links ]
2) Watson J. Watson’s theory of human caring and subjective living Experiences: carative factors/caritas processes as a Disciplinary guide to the professional nursing practice. Texto Context Enferm. 2007; 16(1): 129-35. [ Links ]
3) Ceballos P. Desde los ámbitos de enfermería, analizando el cuidado humanizado, Ciencia y Enfermería. 2010; 16 (1): 31-5. [ Links ]
4) Boada J, Ficapal-Cusí. (2012). Salud y trabajo los nuevos y emergentes riesgos psicosociales. Editorial UOC: Barcelona, España; 2012. [ Links ]
5) Díaz X, Mauro A. Riesgos psicosociales y salud mental de trabajadores y trabajadoras del sector salud en Chile E. Ansoleaga, O. Artaza, & J. Suarez, (Eds.) Personas que cuidan personas: dimensión humana y trabajo en salud. Santiago, Chile: OPS/OMS. 2012: 146-164. Disponible en: http://scielo.proyectoaraucaria.cl/documentos/20130627103555Riesgos%20psicosociales%20y%20salud%20mental%20de%20trabajadores%20y%20trabajadoras%20del%20sector%20salud%20en%20Chile.pdf [ Links ]
6) Karasek R. Job demand, job decision latitude, and mental strain: implication for job redesign. Rev Administrative Science Quarterly. 1979; (24). [ Links ]
7) Karasek R, Baker D, Marxer F, Ahlbom A, Theorrel T. Job Decision latitude, job demands, and cardiovascular disease: A prospective study of Swedish men. AJPH. 1981; 71 (7): 694-705. [ Links ]
8) Vega S. Riesgo psicosocial: el modelo demanda-control-apoyo social. Ministerio del trabajo y asuntos sociales España. 2001. Disponible en: http://www.insht.es/InshtWeb/Contenidos/Documentacion/FichasTecnicas/NTP/Ficheros/601a700/ntp_603.pdf . [ Links ]
9) Siegrist J. Adverse health Effects of high-effort/ low-reward conditions. Journal of occupational health psychology. 1996; 1(1): 27-41. [ Links ]
10) Grazziano E, Ferraz E. Impacto del estrés ocupacional y burnout en enfermeros. Revista enfermería global. 2014; 9(1): s/p. [ Links ]
11) Hinostroza N. El cuidado profesional de enfermería un enfoque humanístico, Rev.enferm.vanguard. 2014; 2 (1):86-97. [ Links ]
12) Watson J. Caring science as sacred science. Philadelphia: F.A. Davis Company; 2005. [ Links ]
13) Urra E, Jara A, García M. Algunos aspectos esenciales del pensamiento de Jean Watson y su teoría de cuidados transpersonales. Ciencia y enfermería. 2011; XVIII (3):11-22. [ Links ]
14) González L, Velandia A, Flores V. Humanización del cuidado de enfermería. De la formación a la práctica clínica. Revista CONAMED 2009; 40- 43. [ Links ]
15) Grove S, Gray J, Burns N. Investigación en enfermería. Desarrollo de la práctica enfermera basada en la evidencia. 6 ed. Barcelona, España: Elsevier; 2016. P 209-246. [ Links ]
16) Emanuel E, Wendler D, Grandy C. ¿What make clinical research ethical?. JAMA: 2701-2711. [ Links ]
17) Alvarado R, Pérez J, Saavedra N, Fuentealba C, Alarcón A, Marchetti N, Aranda W. Validación de un cuestionario para evaluar riesgo psicosocial en el ambiente laboral en Chile. Rev Med Chile. 2012; 140: 1154-63. [ Links ]
18) Poblete M, Valenzuela S, Merino J. Validación de dos escalas utilizadas en la medición del cuidado humano transpersonal basadas en la teoría de Jean Watson. Aquichán. 2012; 12(1):8-21. [ Links ]
19) Juárez A. Factores psicosociales relacionados con la salud mental en profesionales de servicios humanos de México. Revista ciencia y trabajo. 2004; 6(14): 189-96. [ Links ]
20) Ceballos P, Rolo G, Hernández E, Díaz D, Paravic T, Burgos M. Factores psicosociales e carga mental de trabajo: una realidad percibida de los enfermeros en Unidades de Terapia Intensiva. Revista Latino-Americana de Enfermagem. 2015; 23(2), 315-22. [ Links ]
21) Moncada S, Serrano C, Font A, Galtés A, Navarro A. Exposición a riesgos psicosociales entre la población asalariada en España: valores de referencia de las 21 dimensiones del cuestionario COPSQ ISTAS 21. Rev Esp Salud Pública. 2004-2005; 82: 667-75. [ Links ]
22) Afio J, Soares E, Miranda L, Ponte R. Cuidado humanizado en terapia intensiva: un estudio reflexivo. Esc Anna Nery Enferm. 2007; 11(2):325-30. [ Links ]
23) Vila V, Rossi L. Significado cultural del cuidado humanizado en la unidad de terapia intensiva: “Mucho se habla y poco se ve”. Rev Latino-am Enfermagem. 2002; 10(2):137-44. [ Links ]
25) Almeida I, Paes M. Atención humanizada de enfermería: el agir con respeto en un hospital universitario. Revista brasileira de enfermagem REBEn. 2007; 60 (5):546-51. [ Links ]
26) Oliveira S, Queiroz J, Melo R. Cuidando y humanizando: obstáculos que dificultan estas prácticas. Rev. Enferm. UER. 2010; 18 (4): 598-603. [ Links ]
28) Mesa L, Romero M. (2010). Profesionales de enfermería y cuidado en las condiciones laborales actuales. Investigación en Enfermería: Imagen y Desarrollo. 2010; 12(2), 55-92 [ Links ]
Received: September 28, 2017; Accepted: March 08, 2018
 Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
