










Servicios Personalizados
Revista

Articulo
 texto en
texto en  Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
Links relacionados
Compartir

 Permalink
PermalinkOdontoestomatología
versión impresa ISSN 0797-0374versión On-line ISSN 1688-9339
Odontoestomatología vol.24 no.40 Montevideo dic. 2022 Epub 01-Dic-2022
https://doi.org/10.22592/ode2022n40e412
Case report
Solitary maxillary central incisor syndrome: a case report

1Práctica privada.Colombia diana.mamian@correounivalle.edu.co
2Hospital del Día Nova Clínica “El Recreo”, Colombia
Solitary maxillary central incisor syndrome is a rare alteration in the development and formation of organs located mainly in the midline; which occurs early between days 35 to 38 of intrauterine life. Its etiology is unknown, although it has been associated with deletions of chromosomes 7 (7q.36.1) and 8, and mutations in the Sonic Hedgehog gene. It has a prevalence of 1/50,000 live births and although it is a rare anomaly of craniofacial development, its early diagnosis and treatment are important for general dentists or specialists since it can be a sign of other serious congenital or developmental anomalies. Therefore, the objective of this case is to report the initial phase of treatment in a child with solitary maxillary central incisor syndrome who had not been previously diagnosed with this syndrome.
Clinical case:
Male patient, 10 years old, from Jamundí, Valle del Cauca- Colombia. Reports absence of upper dental organ. Intraoral examination shows a solitary central incisor on the maxillary midline, absence of labial frenulum and incisive papilla, oval palate and mandibular retrognathism. He was treated in a first phase with maxillary functional orthopedics to improve class II and is waiting to start the second phase of orthodontic treatment.
Conclusions:
Solitary maxillary central incisor syndrome is a rare syndrome which involves multiple conditions that interfere with the normal development and growth of anatomical structures.
Keywords: solitary maxillary central incisor syndrome; development; craniofacial malformation; congenital anomaly; single incisor
El síndrome del incisivo central maxilar único es una rara alteración en el desarrollo y formación de órganos ubicados principalmente en la línea media; el cual ocurre de manera temprana entre los días 35 al 38 de vida intrauterina. Su etiología es desconocida, aunque se ha asociado a deleciones de los cromosomas 7 (7q.36.1) y 8, y a mutaciones en el gen Sonic Hedgehog. Presenta una prevalencia de 1/50.000 nacidos vivos y aunque es una anomalía poco frecuente del desarrollo craneofacial, su diagnóstico y tratamiento temprano son importantes para los odontólogos generales o especialistas ya que puede ser un signo de otras anomalías congénitas o del desarrollo graves. Por lo tanto, el objetivo de este caso es reportar la fase inicial de tratamiento en un niño con el síndrome de incisivo central maxilar único quien no había sido diagnosticado anteriormente con este síndrome.
Caso Clínico:
Paciente masculino de 10 años de edad, procedente de Jamundí, Valle del Cauca- Colombia. Reporta ausencia de órgano dentario superior. En el examen intraoral se observa un incisivo central único sobre la línea media del maxilar, ausencia de frenillo labial y papila incisiva, paladar oval y retrognatismo mandibular. Fue tratado en una primera fase con ortopedia funcional maxilar para mejorar la clase II y está a la espera de iniciar la segunda fase de tratamiento con ortodoncia.
Conclusiones:
El síndrome de incisivo central maxilar único es un síndrome poco frecuente el cual conlleva múltiples afecciones que interfieren en el normal desarrollo y crecimiento de estructuras anatómicas.
Palabras claves: Síndrome del incisivo central maxilar único; Malformación craneofacial; Anomalía congénita; Incisivo único
A síndrome do incisivo central superior único é uma alteração rara no desenvolvimento e formação de órgãos localizados principalmente na linha média; que ocorre precocemente entre os dias 35 a 38 de vida intrauterina. Sua etiologia é desconhecida, embora tenha sido associada a deleções dos cromossomos 7 (7q.36.1) e 8, e mutações no gene Sonic Hedgehog. Tem uma prevalência de 1/50.000 nascidos vivos e, embora seja uma anomalia rara do desenvolvimento craniofacial, seu diagnóstico e tratamento precoces são importantes para dentistas gerais ou especialistas, pois pode ser sinal de outras anomalias congênitas ou de desenvolvimento graves. Portanto, o objetivo deste caso é relatar a fase inicial do tratamento em uma criança com síndrome do incisivo central superior único que não havia sido previamente diagnosticada com essa síndrome.
Caso clínico:
Paciente do sexo masculino, 10 anos, procedente de Jamundí, Valle del Cauca- Colômbia. Relata ausência de órgão dentário superior. O exame intraoral mostra um único incisivo central na linha média maxilar, ausência de frênulo labial e papila incisiva, palato oval e retrognatismo mandibular. Foi tratado numa primeira fase com ortopedia funcional maxilar para melhorar a classe II e aguarda para iniciar a segunda fase do tratamento ortodôntico.
Conclusões:
A síndrome do incisivo central superior único é uma síndrome rara que envolve múltiplas condições que interferem no desenvolvimento e crescimento normal das estruturas anatômicas.
Palavras chave: Síndrome do incisivo central superior único; Desenvolvimento; Malformação craniofacial; Anomalia congênita; Incisivo único
Introduction
Solitary median maxillary central incisor syndrome (SMMCI) is a rare alteration in the development and formation of organs located mainly in the midline of the dental arch. It occurs early in intrauterine life, between days 35 and 38.1-4 It specifically presents multiple defects in the craniofacial bones, nasal airway, brain and increased risk of malformation and malfunction of the pituitary gland.5-7 An association has been reported with short stature, microcephaly, and epilepsy in 25% of cases.2
The condition was first described by Scott et al. in 1958 as an isolated defect.11 In 1976, Rappaport et al. associated it with short stature and named it “monosuperocentroincisivodontic dwarfism.”8 In 2006, Hall et al. described this condition as solitary median maxillary central incisor syndrome, short stature, choanal atresia/medionasal stenosis, which is now abbreviated as “solitary median maxillary central incisor syndrome.”9 It involves both deciduous and permanent dentition. Although it differs anatomically from the “normal” central incisor, its root and crown are entirely symmetrical.1
Diagnosis
The condition can be diagnosed with ultrasound at 18 to 22 weeks of gestation and with genetic testing, but this is rarely done before birth.4 With our current knowledge, the condition should be detected before eight months with the eruption of the primary maxillary incisor.9
We must specify the following factors to describe the characteristic tooth present in this syndrome accurately:
- Solitary: the tooth is the only central incisor in the maxilla.1,2,9,10
- Median: this tooth is present precisely in the midline of the maxillary alveolus (a single central incisor tooth present to one or other side of the midline indicates that the contralateral tooth has been lost from trauma or disease or did not continue to develop).1,2,10-16
- Maxillary: this characteristic tooth is present only in the maxilla and not in the mandible.1,2,8,10-16.
- Central incisor: the tooth is a central incisor, although the crown is unusually shaped and is not a supernumerary tooth (mesiodens).19
Differential diagnosis
No other conditions with this characteristic incisor tooth are known. One of the three forms of nasal obstruction and short stature will occur in most cases. SMMCI should be considered a predictor of holoprosencephaly, especially if microcephaly and hypotelorism are also present.9
Although generally mildly affected, patients with SMMCI belong to the holoprosencephaly spectrum and are at risk of having children with more severe forms of this disorder. Therefore, molecular diagnosis and genetic counseling are essential for SMMCI patients and their families.12
Etiology and epidemiology
Although its etiology is unknown, it has been associated with deletions of chromosomes 7 (7q.36.1) and 8 and mutations in the Sonic Hedgehog (SHH) gene. It has a prevalence of 1/50,000 live births, which makes it a rare but important anomaly. There is no gender predilection, although more cases are reported in women.1,2,4,8,9,12,16,21-25
SMMCI has five phenotypic characteristics in both dentitions:
1. No labial philtrum and an arch-shaped upper lip5
2. A single symmetrical upper central incisor1,2,5,10,16,20
3. Absence of the upper labial frenulum and the papilla between the upper central incisors5
4. Fusion of the anterior part of the palatal suture5
5. Presence of a bony ridge in the middle of the palate5
Treatment
The American Academy of Pediatric Dentistry (AAPD) acknowledges the importance of proper developmental and occlusal management during the early years of life. Therefore, we can enhance the well-being of infants, children, and adolescents.21,23 Early diagnosis and multidisciplinary management are necessary to achieve such objectives.1 This approach should include these specialties: pediatric dentistry, maxillary orthopedics, orthodontics, periodontics, and in some cases, maxillofacial surgery. Treatment options reported in the literature include functional orthopedics to manage class II malocclusion,7 rapid palatal expansion,7,14,26 distalization of the posterior zone to open the anterior space with orthodontics and then placing an implant to replace the missing incisor.3,5,7,14,21,26 Dental autotransplantation is another reported treatment option, including, e.g., premolars, blending in the transplanted tooth, and replacing the missing incisor.27 A more radical option is removing the single central incisor, closing the space with orthodontics, rehabilitating the lateral incisors with ceramic crowns, and blending in the canines.5
Therefore, this study aims to report the initial treatment of a child with SMMCI who had not been previously diagnosed.
The SMMCI case presented has familial causes.
Clinical case description
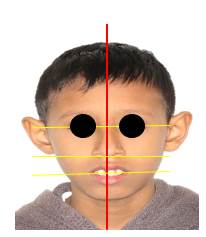
Male patient, 10 years old, weighs 23 kg, height is 123 cm, from Jamundí, Valle del Cauca, Colombia. He attended the office with his aunt, the adult in charge, who stated the following reason for consultation: “My nephew has only one front tooth”. During the interview, she explains that the child is the second of three term pregnancies. Family history: paternal aunt has diabetes, hypertension, and unspecified cancer. The child’s history is not reported. The aunt said the child’s deciduous dentition included only one upper central incisor. She also noted that his other two siblings have the same problem. The extraoral examination showed that the midline does not coincide with the tip of the nose nor the center of the chin; there is no labial philtrum, and the bipupillary plane is not parallel to the commissural line. There is lip incompetence, ears of increased size, projection, and implantation. (Figure 1) The intraoral examination showed a solitary central incisor on the maxillary midline, absence of labial frenulum and incisive papilla, an oval palate, and class II malocclusion with proinclination of the central incisor. (Figure 2 a, b, and c).
Complementary studies are performed to make the right diagnosis and start the treatment: study models, panoramic and lateral skull radiographs, and extra and intraoral photos.

A. Front view showing the solitary maxillary incisor and deep bite. B. Occlusal view showing absence of interincisive papilla. C. Lateral view showing mandibular retrognathism.
The panoramic radiograph (Figure 3) showed a solitary maxillary incisor with a single root and root canal. No formation or impaction of the other central incisor is observed.

Figure 3: Panoramic radiograph showing the absence of the germ of the missing central incisor, which rules out the impaction of the central incisor
In the Lavergne and Petrovick cephalometry, performed taking the lateral cephalograms as a reference (Figure 4), the patient has shown neutral mandibular rotation, maxilla larger than the mandible, a distal anteroposterior relation with a normal vertical relation (R2DN).

Figure 4: Lateral cephalogram showing proinclination of upper incisors and decreased mandibular length
Pont’s analysis (transverse space) was performed to determine the need for space in the upper and lower arches. This showed that the patient had a space deficit in the anterior and posterior zones of the two arches. Moyer’s analysis (eruption space for canines and premolars) shows a space deficit only in the lower arch.
The cephalometric study showed the following:
- A retrognathic profile
- Mandibular retrognathism
- Clockwise jaw rotation
- Vertical growth
- Dental and skeletal Class II
- Short mandibular length
- Dolichofacial type
- Proinclined and protruded upper incisors
- Increased overjet and overbite
- Deep bite
Solitary median maxillary central incisor syndrome is diagnosed based on the studies performed.
There was a functional and esthetic compromise. Therefore, a twophase treatment plan was carried out. The first phase lasted approximately one year and used maxillary orthopedic appliances. Two treatment options were suggested for phase two to replace the missing incisor.
PHASE 1:
1. Maxillary orthopedics with Simoes Network 1 (SN1) to increase mandibular length and correct Class II malocclusion.
PHASE 2:
1. Orthodontics to provide space between the central and lateral incisor for implant placement to replace the missing incisor.
2. Orthodontics to align teeth, close spaces, and blend in the anterior sector.
The child’s guardian chose the orthodontics treatment, and the second phase is still pending due to the costs to cover.
Phase 1 started on 8 June 2021, and the patient was scheduled for monthly checkups for six months. In December 2021, a photographic control was performed, showing a decrease in the overjet and overbite, an improved profile, and a corrected deep bite (Figures 5 and 6). The patient attended checkups until the first year of treatment.

Figure 5: After six months of treatment, the frontal photograph shows an improved deep bite; the central incisor remains in the midline

Figure 6: Lateral photograph after six months of treatment showing correction of mandibular retrognathism
The patient is being treated at the Pediatric Medicine Department.
Discussion
SMMCI is a rare disorder that may occur as an isolated finding or associated with systemic abnormalities and genetic and environmental factors which alter the normal mitotic division during tooth formation.8 The clinical and radiological findings, and the absence of a history of trauma, confirmed that the patient in this clinical case had SMMCI.10
In this case, we can infer that family history affected all three siblings, who reported the same characteristics compatible with SMMCI in both the deciduous and permanent dentition. No other family members had the condition.
Some phenotypic characteristics specific to SMMCI are evident in the case reported above, such as short stature, intellectual deficiency, mandibular retrognathism, arched upper lip, poorly defined philtrum, absence of labial frenulum, and no frenulum.19 Inger et al. also describe the solitary central incisor in the mouth with a symmetrical coronal morphology. They do not specify if it is tooth 1.1 or 2.1.27Systemically, people with this syndrome may suffer from heart and kidney diseases and alterations in the sexual organs, among others.3 Therefore, complementary studies must be conducted on this patient because dysfunctions in the organs involved in this syndrome were not ruled out in the case history.
SMMCI is characterized by Class II malocclusion, hypoplasia, and mandibular posterior rotation.26 As previously reported in the literature, the radiographic examinations showed a skeletal class II with a tendency to hyperdivergence due to growth in the mandibular postrotation, proinclination of the upper and lower incisors, and concave facial profile. This requires comprehensive esthetic and functional management.3,7,9,10,16,20,21
Several clinical procedures have been reported to treat this disorder once the right diagnosis has been made.3,7,14,21,26 The therapeutic options include functional orthopedic appliances—as was done in this case—where the mandibular size was improved, considering the patient’s age and growth potential. Later, when patients have their permanent dentition, esthetic management with fixed orthodontics5,14,21,26 and oral rehabilitation will be performed to complete the dental treatment.26
Conclusion
This case describes a rare syndrome that involves multiple conditions that interfere with the normal development and growth of anatomical structures. Therefore, as dentists and other specialists, we must be attentive to the oral manifestations of SMMCI. These findings can be crucial to correctly diagnose this syndrome since it may go unnoticed throughout the person’s life. Timely treatment at an early age using functional orthopedics will improve the functional and esthetic prognosis, thus achieving better patient satisfaction.
REFERENCES
1. Medellín Pedraza N.; Garrigós Esparza L.D.; Márquez Preciado R. y cols. Síndrome del incisivo central maxilar único y el papel del odontopediatra en el manejo interdisciplinario: Reporte de un caso clínico. Odontol Pediátr. 2018;26 (2): 155-63. [ Links ]
2. Mustafa MM, Zakirulla M, AlShahrani I, Togoo RA, Alkahtani ZM, Ain TS. Clinical Evaluation of Solitary Median Maxillary Central Incisor Syndrome. Case Rep Dent. 2019 Sep 12;2019:2637825. [ Links ]
3. Nalawade TM, Mallikarjuna RM, Sogi HPS, Bhat KG, Kumbar VM. Solitary Median Maxillary Central Incisor: A Case Report with 3-Year Follow-Up and Literature Review. Contemp Clin Dent. 2021 Jul-Sep;12(3):324-327. [ Links ]
4. Johnson N, Windrim R, Chong K, Viero S, Thompson M, Blaser S. Prenatal diagnosis of solitary median maxillary central incisor syndrome by magnetic resonance imaging. Ultrasound Obstet Gynecol. 2008 Jul;32(1):120-2. [ Links ]
5. Schneider UEM, Moser L. Orthodontic space closure in a young female patient with solitary median maxillary central incisor syndrome. Am J Orthod Dentofacial Orthop. 2021 Jul;160(1):132-146. [ Links ]
6. Ilhan O, Pekcevik Y, Akbay S, Ozdemir SA, Memur S, Kanar B, Kirbiyik O, Ozer EA. Solitary median maxillary central incisor, holoprosencephaly and congenital nasal pyriform aperture stenosis in a premature infant: case report. Arch Argent Pediatr. 2018 Feb 1;116(1):e130-e134. [ Links ]
7. Lygidakis NN, Chatzidimitriou K, Petrou N, Lygidakis NA. Solitary median maxillary central incisor syndrome (SMMCI) with congenital nasal puriform aperture stenosis: literature review and case report with comprehensive dental treatment and 14 years follow-up. Eur Arch Paediatr Dent. 2013 Dec;14(6):417-23. [ Links ]
8. Rappaport EB, Ulstrom R, Gorlin RJ. Monosuperocentroincisivodontic dwarfism. Birth Defects Orig Artic Ser. 1976;12(5):243-5. [ Links ]
9. Viana Eda S, Kramer PF, Closs LQ, Scalco G. Solitary median maxillary central incisor syndrome and holoprosencephaly: a case report. Pediatr Dent. 2010 Sep-Oct;32(5):424-7. [ Links ]
10. Utreja A, Zahid SN, Gupta R. Solitary median maxillary central incisor in association with hemifacial microsomia: A rare case report and review of literature. Contemp Clin Dent. 2011 Oct;2(4):385-9. [ Links ]
11. Hall RK. Solitary median maxillary central incisor (SMMCI) syndrome. Orphanet J Rare Dis. 2006 Apr 9;1:12. [ Links ]
12. Chandrasekaran D, Yezdani A, Tajir F, Saravanan B, Rajasekar L. Solitary median maxillary central incisor: A case report of a rare dental anomaly. J Pharm Bioallied Sci. 2015 Apr;7(Suppl 1):S307-8. [ Links ]
13. Poelmans S, Kawamoto T, Cristofoli F, Politis C, Vermeesch J, Bailleul-Forestier I, Hens G, Devriendt K, Verdonck A, Carels C. Genotypic and phenotypic variation in six patients with solitary median maxillary central incisor syndrome. Am J Med Genet A. 2015 Oct;167A(10):2451-8. [ Links ]
14. Garcia Rodriguez R, Garcia Cruz L, Novoa Medina Y, Garcia Delgado R, Perez Gonzalez J, Palma Milla C, Lopez Siles J, Medina Castellano M, Garcia Hernandez JA, Santana Rodriguez A. The solitary median maxillary central incisor (SMMCI) syndrome: Associations, prenatal diagnosis, and outcomes. Prenat Diagn. 2019 May;39(6):415-419. [ Links ]
15. Machado E, Machado P, Grehs B, Grehs RA. Solitary median maxillary central incisor syndrome: Case report. Dental Press J Orthod. 2010 July-Aug;15(4):55-6 [ Links ]
16. Szakszon K, Felszeghy E, Csízy I, Józsa T, Káposzta R, Balogh E, Oláh E, Balogh I, Berényi E, Knegt AC, Ilyés I. Endocrine and anatomical findings in a case of Solitary Median Maxillary Central Incisor Syndrome. Eur J Med Genet. 2012 Feb;55(2):109-11. [ Links ]
17. Barcelos R, Tannure P, Farinhas J, Kahn E, Gleiser R. Solitary median maxillary central incisor in two healthy siblings: case report. J Disability Oral Health 2011; 12(3): 133-135. [ Links ]
18. Mendoza D, Fragoso A, Yamamoto A. Síndrome del incisivo central único de la línea media del maxilar y fusión de incisivos centrales permanentes mandibulares: Reporte de un caso clínico. Revista Odontológica Mexicana a 2005;9 (1): 37-41 [ Links ]
19. Negi A, Negi A, Mohanan M. Solitary median maxillary central incisor syndrome: A rare entity. J Oral Maxillofac Pathol. 2020 May-Aug;24(2):402. [ Links ]
20. Blackmore K, Wynne DM. A case of solitary median maxillary central incisor (SMMCI) syndrome with bilateral pyriform aperture stenosis and choanal atresia. Int J Pediatr Otorhinolaryngol. 2010 Aug;74(8):967-969. [ Links ]
21. Bolan M, Derech CD, Côrrea M, Ribeiro GLU, Almeida ICS. Palatal expansion in a patient with solitary median maxillary central incisor syndrome. Am J Orthod Dentofacial Orthop. 2010 Oct;138(4):493-497. [ Links ]
22. De Lima Pedro R, Kchler EC, Primo LG, de Castro Costa M. Solitary Median Maxillary Central Incisor Syndrome: An esthetic solution in a child. J Dent Probl Solut 2017; 4(4): 072-075 [ Links ]
23. Muñoz Aguilar G, Alcón Sáez J.J., Domingo Triadó I. Síndrome del incisivo central maxilar único. Acta Pediatr Esp. 2014; 72(3): e100-e104. [ Links ]
24. Srivathsa SH. Congenitally missing maxillary central incisor or solitary median maxillary central incisor?. Int J Orofac Res 2018;3:17-9. [ Links ]
25. Nanni L, Ming JE, Du Y, Hall RK, Aldred M, Bankier A, Muenke M. SHH mutation is associated with solitary median maxillary central incisor: a study of 13 patients and review of the literature. Am J Med Genet. 2001 Jul 22;102(1):1-10. [ Links ]
26. Zatonski T, Pazdro-Zastawny K, Morawska-Kochman M, Biela M, Koltowska A, Rydzanicz M, Rozensztrauch A, Kosinska J, Dorobisz K, Ploski R, Smigiel R. Single median maxillary central incisor syndrome and variant in SMO gene associated with SHH pathway. Int J Pediatr Otorhinolaryngol. 2020 Jul;134:110038. [ Links ]
27. Nota A, Ehsani S, Pittari L, Gastaldi G, Tecco S. Rare case of skeletal third class in a subject suffering from Solitary Median Maxillary Central Incisor syndrome (SMMCI) associated to panhypopituitarism. Head Face Med. 2021 Nov 23;17(1):49. [ Links ]
Ethical considerations: It is stated that the patient and his legal representative were informed by means of informed consent of the intention to publish this novel case. The child’s legal representative signs and agrees to make this study available for consideration by the scientific community.
Authorship contribution: 1. Conception and design of study 2. Acquisition of data 3. Data analysis 4. Discussion of results 5. Drafting of the manuscript 6. Approval of the final version of the manuscript DMMT has participated in 1, 2, 3, 4, 5, 6. RFDT has participated in 3, 4, 5, 6.
Received: January 31, 2022; Accepted: September 27, 2022
 Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
