










Servicios Personalizados
Revista

Articulo
 texto en
texto en  Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
Links relacionados
Compartir

 Permalink
PermalinkOdontoestomatología
versión impresa ISSN 0797-0374versión On-line ISSN 1688-9339
Odontoestomatología vol.24 no.39 Montevideo jun. 2022 Epub 01-Ago-2022
https://doi.org/10.22592/ode2022n39e410
Case report
Unusual root and canal morphology of the mandibular first molar as an indication for cone-beam computed tomography: About a “borderline” endodontic case

1Departamento Odontología Integral Adulto, Facultad de Odontología, Universidad de La Frontera, Temuco, Chile.
2Centro de Investigación en Odontología Legal y Forense, Facultad de Odontología, Universidad de La Frontera, Temuco, Chile. gabriel.fonseca@ufrontera.cl
Cone-beam computed tomography (CBCT) is a promising tool in dental practice. CBCT provides three-dimensional images and imaging resolution to be used in endodontics. This enhances the diagnosis of various pathologies. However, guidelines have recommended limiting its use due to overexposure to radiation. This article presents the rare case of a mandibular molar with a single root and canal that benefited from taking a CBCT. A 48-year-old woman is referred for endodontic treatment of the permanent left mandibular first molar. The preoperative radiographic examination showed an unusual canal centered along a single root. Taking a CBCT with the relevant information and the patient’s consent improved her diagnosis and treatment. CBCTs should not be used routinely for these purposes but could be justified in “borderline” cases. This paper discusses its indication and clinical implementation following current recommendations and guidelines.
Keywords: Cone-Beam Computed Tomography; endodontics; diagnosis; bioethics; tooth abnormalities; risk-reduction behavior
La Tomografía Computarizada de Haz Cónico (CBCT) representa una promisoria herramienta para la clínica odontológica. En Endodoncia, CBCT ofrece tridimensionalidad y resolución imagenológica, potenciando el diagnóstico de diferentes condiciones patológicas. Sin embargo, su limitación por sobreexposición a radiación, ha llevado a directrices que recomiendan cautela para su indicación. Se presenta un caso infrecuente de un molar mandibular con una sola raíz y canal, y las circunstancias de uso de CBCT. Mujer de 48 años es derivada para endodoncia del primer molar mandibular izquierdo permanente. El examen radiográfico preoperatorio demostró el hallazgo inusual de un canal centrado en una única raíz. Con la información apropiada y el consentimiento de la paciente, la indicación de CBCT favoreció su diagnóstico y tratamiento. CBCT no debería ser utilizada rutinariamente para estos fines, pero podría justificarse en casos "fronterizos". Se discuten su indicación e implementación clínica, siguiendo actuales recomendaciones y directrices.
Palabras clave: Tomografía computarizada de haz cónico; endodoncia; diagnóstico; bioética; anomalías dentales; comportamiento de reducción de riesgos
A tomografia computadorizada de feixe cônico (TCFC) representa uma ferramenta promissora para a clínica odontológica. Na Endodontia, a CBCT oferece tridimensionalidade e resolução de imagem, potencializando o diagnóstico de diferentes condições patológicas. No entanto, sua limitação devido à superexposição à radiação levou a diretrizes que recomendam cautela em sua indicação. Um caso raro de um molar inferior com uma única raiz e canal é apresentado e as circunstâncias do uso da TCFC. Uma mulher de 48 anos é encaminhada para tratamento de canal para o primeiro molar inferior esquerdo permanente. O exame radiográfico pré-operatório demonstrou o achado incomum de um canal centrado em uma única raiz. Com as devidas informações e o consentimento do paciente, a indicação da TCFC favoreceu seu diagnóstico e tratamento. A CBCT não deve ser usada rotineiramente para esses fins, mas pode ser justificada em casos "fronteiriços". Sua indicação e implementação clínica são discutidas, seguindo as recomendações e diretrizes atuais.
Palavras-chave: Tomografia computadorizada de feixe cônico; endodontia; diagnóstico; bioética; anormalidades dentárias; comportamento de redução de risco
Introduction
Medical imaging technology has advanced rapidly in recent decades, offering significant benefits to patients worldwide. This development has been particularly enhanced by computed tomography (CT), which is now an established tool in many areas of medicine. The new CT applications are a significant advance as a tool for clinical practice and research. Such is the case of cone-beam computed tomography (CBCT), which was designed to meet dental practice needs.1 In endodontics (the dental specialty that studies dental pulp diseases, their impact on periapical tissues, and their treatment), CBCT provides three-dimensional visibility of the region and accurate detail and resolution of the dental and alveolar anatomy.2 This improves the diagnosis of various pulpal and periapical malformations and pathologies.1,3 However, CBCT has known limitations, including potentially overexposing patients to radiation.4 Although the effective dose of CBCT is lower than that of a regular CT, it is much higher than that of conventional periapical intraoral radiographs.2
Various guidelines and directives have been published on the use of CBCT in dental and maxillofacial radiology. All of them recommend that it be used with caution and that quality of care and optimization strategies must be in place to protect radiologists, dentists, physicians, and manufacturers.1,5 These guidelines are supported by sufficient evidence to justify a sound and scientific clinical use of CBCT based on specific indications. In some exceptional cases, when conventional radiographs are negative or patients have contradictory or non-specific clinical signs and symptoms, CBCT may be the imaging modality of choice for diagnosis.1,4 These exceptional cases, also called “borderline,”3 have led some authors to recommend more thorough research to objectively establish the diagnostic accuracy of CBCT and its impact on decision making.1,6
This is the case of a permanent mandibular first molar with a single root and canal. CBCT provided accurate information about the root’s anatomy, making it possible to clean and shape the canal system appropriately. These are essential elements for endodontic treatment to be successful. CBCT should not be routinely used for endodontic diagnosis but may be justified in “special” or “borderline” cases. This paper discusses the use of CBCT as a diagnostic and therapeutic tool in these cases, and its implementation in clinical research, always following current legal recommendations and guidelines.
Background
In routine examinations, dental anomalies in permanent teeth are rare and often incidental findings.3 The anatomical variations of mandibular first molars, both in shape and number of roots or canals, typically present exceptional complexities.7-9 It is infrequent to find a single root and canal. This condition should be addressed carefully to ensure correct endodontic treatment.7,9-12 While multiple preoperative conventional radiographs with different angulations could confirm this abnormal morphology, CBCT has been suggested as an ideal tool to search for hidden accessory canals or avoid excessive dentin removal or even more significant complications.7 Although current published guidelines state that CBCT is not a standard indication for determining root canal anatomy, they also recommend CBCT for the preoperative endodontic treatment of teeth with unusual root or canal morphology. 1,5
Case description
A 48-year-old female patient with no medical history was referred to the Endodontics Area of the Teaching and Assistance Dental Clinic of the Dental School of Universidad de La Frontera (Temuco, Chile) to treat the permanent left mandibular first molar (tooth 46). This procedure was indicated for subsequent prosthetic rehabilitation. The usual clinical tests were performed, and asymptomatic irreversible pulpitis with normal apical tissues was diagnosed. The preoperative radiographic examination showed deep restorations, a slightly retracted pulp chamber, and the unusual finding of a canal along the center of a single root (Figure 1). It was labeled a type I canal according to Vertucci’s classification.13 The patient was informed, and an informed consent was obtained. The routine non-surgical endodontic treatment started with conventional access to the pulp chamber using special burs and rotary instruments. Trepanation macroscopically confirmed a single large canal located in the center of the pulp chamber, which was prepared chemomechanically following the institution’s standard protocols. CBCT was considered before resuming endodontic treatment in a subsequent session, given how peculiar the canalicular anatomy was and to evaluate the potential presence of accessory canals or morphological masking that might compromise the procedure.

Figure 1: Periapical radiograph. Note the diffuse image of a canal centered along a single root in the mandibular first molar(*): an extremely rare finding
Following the legal health standards, the costs and advantages of CBCT compared to the imaging studies already performed were discussed with the patient. She was told that informed consent was required after considering the risks and benefits of CBCT. The patient was also notified of the potential therapeutic errors of endodontics if the practitioner did not have the information provided with a more reliable study. Once all the information was provided and discussed, the patient agreed to undergo the study in the imaging area of the institution.
The CBCT (Vatech Pax Zenith CBCT machine, 120 kVp and 9.0 mA, FOV 8x6 cm, 0.12 mm voxel size) was studied with GALILEOS Viewer 1.9 software (SICAT GmbH & Co. KG, Bonn, Germany). A three-dimensional image of the tooth was obtained to assess its axial, sagittal, and coronal sections. The images confirmed the presence of a single root with a single oval-shaped canal extending from the pulp chamber to the apex. This canal was classified as Vertucci type I (Figure 2).
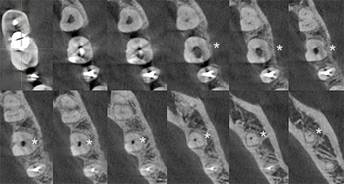
Figure 2: CBCT, multiple images in axial sections. Note the continuity of a single canal without accessory canals (*)
The unusual characteristics were confirmed, and it was established that there were no unfavorable conditions for resuming the procedure. The patient was scheduled for a second session to complete the endodontic treatment. The second session took place seven days later: the temporary filling was removed, and the chemomechanical preparation started in the first session was resumed. The canal was obturated with the cold gutta-percha lateral compaction technique to achieve better apical control and canal sealing, following standard protocols for this type of canal anatomy. The relevant checkups were performed after 7 and 14 days; the absence of clinical and radiographic signs and symptoms was confirmed. The case was referred back to the treating dentist to continue the already planned prosthetic rehabilitation (Figure 3).

Discussion
Permanent molars have significant variability in the morphology of roots and canals, alterations or malformations that can be determined by disturbances during the canal differentiation stage at any point during tooth development.9,14 The anomaly presented in this report has been mentioned as rare in mandibular first molars7,9-11 (Vertucci type I has been explicitly reported to be the rarest of all).15 The number of roots is the most frequent variation among certain ethnic groups.16 In Chile, however, the high migration rates, the high prevalence of people with multiethnic backgrounds, and the recognized phenomena of miscegenation and globalization17 make it extremely difficult to consider this variable without the relevant genetic support, as considered in the current literature.18 This entails an implicit challenge for endodontists, who must plan each case carefully.
Oval canals are complex to treat endodontically, especially during chemomechanical preparation, because they have areas that are difficult to access and favor detritus accumulation and hinder the elimination of microorganisms.19). In addition, the instruments are usually placed in the center of the canal, preventing proper shaping and disinfection, especially in the buccolingual direction.20
Radiographic examination is essential for diagnosis and throughout the endodontic treatment.9 However, two-dimensional conventional intraoral techniques and the resulting superimposition of structures and geometric distortion of anatomical structures are significant problems due to potential morphological masking. This can lead to diagnostic or therapeutic complications. CBCT obtains three-dimensional images that allow us to explore the area in the sagittal and coronal planes. This provides accurate information on root and canal morphology, and its use is recommended when there are root and canal morphology variations.2 The use of CBCT has already been suggested in cases of aberrant root morphology.12 However, and to our knowledge, careful attention to specific CBCT indications has hardly been reported in this type of case.21
This technology is attractive, and additionally, its diagnostic, therapeutic and research applicability is hotly debated in cases such as the one presented here. Current published guidelines state that CBCTs should not be indicated as the standard procedure for showing root canal anatomy nor replace conventional low-dose, low-risk radiological techniques.1,5 However, these same guidelines mention that CBCT may be indicated in “particular” cases where concurrent factors may complicate endodontic treatment, including “atypical pulp anatomy”1 or “root canal and accessory canal anomalies.”5 The first recommendation of the guidelines of the American Association of Endodontists (AAE) and the American Academy of Oral and Maxillofacial Radiology (AAOMR) emphasizes that “intraoral radiographs should be considered the imaging modality of choice in the evaluation of the endodontic patient,” the third recommendation justifies CBCT “for initial treatment of teeth with the potential for extra canals and suspected complex morphology, such as mandibular anterior teeth, and maxillary and mandibular premolars and molars, and dental anomalies.”4 This case is one of the many situations that need to be analyzed carefully and that are often controversial or, at least, “borderline” situations where the published scientific evidence1 still seems too diffuse to classify “atypical pulp anatomy” as a specific indication for CBCT.
The demand for CBCT in dentistry is on the rise. Its benefits are undeniable: equipment costs have decreased significantly, and in a few years, this technology will indeed be considered a diagnostic tool in general dental practice.22 In clinical research, CBCT is undoubtedly a tool that can make significant and valuable contributions. CBCT was introduced to endodontics in 1990 and has enabled highly reliable morphological and morphometric studies, even more so in three-dimensional environments and with population value.23 This is where running tests and precise indications on how to obtain the results are essential. Noffke et al. 5 state that CBCT tests for research, administrative or medico-legal purposes that have no potential health benefits to the patient or their community should not be allowed or recommended. Besides the risks mentioned above regarding unnecessary radiation exposure, there are countless issues regarding radiological interpretation skills, communicating a diagnosis, or the operator’s responsibilities and certifications that remain unresolved.22
It has been emphasized that a CBCT should be ordered only when the benefits outweigh the potential risks of irradiation. Other diagnostic procedures should be discussed with the patient, especially regarding costs. All the information on CBCT and the reasons justifying its use must be adequately provided. Also, patients must consent to the treatment guidelines, which should be documented.5,24 In this case, the patient was informed of the potential of CBCT to examine her condition because the root anatomical variation of the tooth to be treated had complex diagnostic and therapeutic features and because the literature reported its benefits2 to obtain a specific result: identifying the canals (in some cases masked by the same atypical morphology), thus allowing for the complete disinfection of the canal system. Rosen et al.25 carefully reviewed and analyzed the literature on evaluating the diagnostic efficacy of CBCT in endodontics. They concluded that its expected benefits remain unclear and only limited to its technical effectiveness. We felt that in this case, the initial intraoral radiographs did not provide sufficient information and a CBCT was justified for that purpose. Even though CBCT’s pros and cons were carefully evaluated and discussed with the patient regarding current healthcare standards, we agree with Scarfe24 that CBCT should be justified on a case-by-case basis and never proposed as routine. CBCT provides three-dimensional assessment of canalicular morphology, avoiding excessive tissue removal and allowing complete disinfection of the system.7) Therefore, we considered that this rare condition needed to be analyzed, or at least its clinical and radiological characteristics mentioned in the current guidelines for the safe use of dental and maxillofacial CBCT. The criteria for selecting cases where CBCT is indicated as imaging support in endodontics are not sufficiently clear or specific.25
The professional standard for CBCT is the “appropriate care” of “choosing CBCT for each patient,” “wisely based on selection criteria derived from the best available evidence.”24 We agree with Noffke et al. 5 that the selection of CBCT images should be based on the professional’s assessment of the patient’s needs, and should never be performed routinely as a “fishing expedition” for an unsuspected disease.
Conclusions
CBCT is a useful tool whose diagnostic indications should be evaluated according to the current concepts of radiological protection since it is not considered a standard procedure for assessing root canal anatomy. Additionally, morphological alterations such as those of this case justify its diagnostic use since endodontic treatment can be complicated by this type of anomaly in both roots and root canals. The use of CBCT thus relies on good professional judgment and proper assessment of the risks and benefits of exposing the patient to such radiation.
REFERENCES
1. European Commission (EC). Radiation protection No. 172: evidence based guidelines on cone beam CT for dental and maxillofacial radiology. (internet). Luxembourg: Office for Official Publications of the European Communities, 2012 (fecha de acceso: 8 de Agosto de 2021). Disponible en: Disponible en: https://ec.europa.eu/energy/sites/ener/files/documents/172.pdf [ Links ]
2. Patel S, Durack C, Abella F, Shemesh H, Roig M, Lemberg K. Cone beam computed tomography in Endodontics - a review. Int. Endod, J. 2015; 48(1): 3-15. doi: 10.1111/iej.12270. [ Links ]
3. Gulsahi A, Ates U, Tirali RE, Cehreli SB. Use of cone-beam computed tomography in diagnosis of an otherwise undetected periapical lesion in an anomalous tooth. Oral Radiol. 2014; 30: 111-4. doi: 10.1007/s11282-013-0130-8. [ Links ]
4. AAE and AAOMR Joint Position Statement: Use of Cone Beam Computed Tomography in Endodontics 2015 Update. J. Endod. 2015; 41(9): 1393-6. doi: 10.1016/j.joen.2015.07.013. [ Links ]
5. Noffke CE, Farman AG, Nel S, Nzima N. Guidelines for the safe use of dental and maxillofacial CBCT: a review with recommendations for South Africa. SADJ. 2011; 66(6): 262, 4-6. [ Links ]
6. Kiljunen T, Kaasalainen T, Suomalainen A, Kortesniemi M. Dental cone beam CT: A review. Phys. Med. 2015; 31(8): 844-60. doi: 10.1016/j.ejmp.2015.09.004. [ Links ]
7. Sooriaprakas C, Ballal S, Velmurugan N. Mandibular first molar with a single root and single canal. Case Rep. Dent. 2014; 2014: 159846. doi: 10.1155/2014/159846. [ Links ]
8. Filpo-Perez C, Bramante CM, Villas-Boas MH, Húngaro Duarte MA, Versiani MA, Ordinola-Zapata R. Micro-computed tomographic analysis of the root canal morphology of the distal root of mandibular first molar. J. Endod. 2015; 41(2): 231-6. doi: 10.1016/j.joen.2014.09.024. [ Links ]
9. Munavalli A, Kambale S, Ramesh S, Ajgaonkar N. Mandibular first molar with single root and single root canal. J. Conserv. Dent. 2015; 18(4): 346-8. doi: 10.4103/0972-0707.159757. [ Links ]
10. Ioannidis K, Lambrianidis T, Beltes P, Besi E, Malliari M. Endodontic management and cone-beam computed tomography evaluation of seven maxillary and mandibular molars with single roots and single canals in a patient. J. Endod 2011; 37(1): 103-9. doi: 10.1016/j.joen.2010.09.001. [ Links ]
11. Demirbuga S, Sekerci AE, Dinçer AN, Cayabatmaz M, Zorba YO. Use of cone-beam computed tomography to evaluate root and canal morphology of mandibular first and second molars in Turkish individuals. Med Oral Patol Oral Cir Bucal. 2013; 18(4): e737-44. doi: 10.4317/medoral.18473. [ Links ]
12. Raghavendra SS, Napte BD, Desai NN, Hindlekar AN. Single C-shaped canal in mandibular first molar: A case report. J. Conserv Dent. 2015; 18(2): 168-71. doi: 10.4103/0972-0707.153060. [ Links ]
13. Vertucci FJ. Root canal anatomy of the human permanent teeth. Oral Surg Oral Med Oral Pathol Oral Radiol Endodontics. 1984; 58(5): 589-99. doi: 10.1016/0030-4220(84)90085-9. [ Links ]
14. Haridoss S, Swaminathan K, Rajendran V, Rajendran B. Single-rooted primary first mandibular molar. BMJ Case Rep. 2014; 2014. pii: bcr2014206347. doi: 10.1136/bcr-2014-206347. [ Links ]
15. Gaur A, Trivedi HP, Gupta M, Sharma A, Likhyani L, Agarwal M. Mandibular First Molar with Vertucci Type I Canal Configuration diagnosed with the Help of Cone Beam Computed Tomography: A Rare Case Report. J Contemp Dent Pract. 2014; 15(6): 784-7. doi: 10.5005/jp-journals-10024-1618. [ Links ]
16. de Pablo OV, Estevez R, Heilborn C, Cohenca N. Root anatomy and canal configuration of the permanent mandibular first molar: clinical implications and recommendations. Quintessence Int. 2012;43(1):15-27. [ Links ]
17. Torres A, Jacobs R, Lambrechts P, Brizuela C, Cabrera C, Concha G, Pedemonte ME. Characterization of mandibular molar root and canal morphology using cone beam computed tomography and its variability in Belgian and Chilean population samples. Imaging Sci Dent. 2015; 45(2): 95-101. doi: 10.5624/isd.2015.45.2.95. [ Links ]
18. Delgado M, Ramírez LM, Adhikari K, Fuentes-Guajardo M, Zanolli C, Gonzalez-José R, Canizales S, Bortolini MC, Poletti G, Gallo C, Rothhammer F, Bedoya G, Ruiz-Linares A. Variation in dental morphology and inference of continental ancestry in admixed Latin Americans. Am J Phys Anthropol. 2019; 168(3): 438-47. doi: 10.1002/ajpa.23756. [ Links ]
19. Velozo C, Prado VFF, Sousa ISDS, Albuquerque MBA, Montenegro L, Silva S, Silva P, Albuquerque D. Scope of Preparation of Oval and Long-Oval Root Canals: A Review of the Literature. ScientificWorldJournal. 2021; 2021:5330776. doi: 10.1155/2021/5330776. [ Links ]
20. Busquim S, Cunha RS, Freire L, Gavini G, Machado ME, Santos M. A micro-computed tomography evaluation of long-oval canal preparation using reciprocating or rotary systems. Int Endod J. 2015; 48(10): 1001-6. doi: 10.1111/iej.12398. [ Links ]
21. Yendreka VC, Fonseca GM. A »,» ®,® §,§ ­, ¹,¹ ²,² ³,³ ß,ß Þ,Þ þ,þ ×,× Ú,Ú ú,ú Û,Û û,û Ù,Ù ù,ù ¨,¨ Ü,Ü ü,ü Ý,Ý ý,ý ¥,¥ ÿ,ÿ ¶,¶ borderline »,» ®,® §,§ ­, ¹,¹ ²,² ³,³ ß,ß Þ,Þ þ,þ ×,× Ú,Ú ú,ú Û,Û û,û Ù,Ù ù,ù ¨,¨ Ü,Ü ü,ü Ý,Ý ý,ý ¥,¥ ÿ,ÿ ¶,¶ dental trauma with 12 y of evolution justifying CBCT as diagnostic method. Biomed. Res. 2018; 29(13): 2800-5. doi: 10.4066/biomedicalresearch.29-18-728. [ Links ]
22. Noffke CE, Farman AG, Van der Linde A, Nel S. Responsible use of cone beam computed tomography: minimising medico-legal risks. SADJ. 2013; 68(6): 256, 8-9. [ Links ]
23. Naseri M, Safi Y, Akbarzadeh Baghban A, Khayat A, Eftekhar L. Survey of Anatomy and Root Canal Morphology of Maxillary First Molars Regarding Age and Gender in an Iranian Population Using Cone-Beam Computed Tomography. Iran Endod. J. 2016; 11(4): 298-303. doi: 10.22037/iej.2016.8. [ Links ]
24. Scarfe WC. »,» ®,® §,§ ­, ¹,¹ ²,² ³,³ ß,ß Þ,Þ þ,þ ×,× Ú,Ú ú,ú Û,Û û,û Ù,Ù ù,ù ¨,¨ Ü,Ü ü,ü Ý,Ý ý,ý ¥,¥ ÿ,ÿ ¶,¶ All that glitters is not gold »,» ®,® §,§ ­, ¹,¹ ²,² ³,³ ß,ß Þ,Þ þ,þ ×,× Ú,Ú ú,ú Û,Û û,û Ù,Ù ù,ù ¨,¨ Ü,Ü ü,ü Ý,Ý ý,ý ¥,¥ ÿ,ÿ ¶,¶ : standards for cone-beam computerized tomographic imaging. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2011; 111(4): 402-8. doi: 10.1016/j.tripleo.2011.01.006. [ Links ]
25. Rosen E, Taschieri S, Del Fabbro M, Beitlitum I, Tsesis I. The Diagnostic Efficacy of Cone-beam Computed Tomography in Endodontics: A Systematic Review and Analysis by a Hierarchical Model of Efficacy. J. Endod. 2015; 41(7): 1008-14. doi: 10.1016/j.joen.2015.02.021. [ Links ]
Conflict of interest declaration: The authors have no conflict of interest regarding the publication of this paper.
Authorship contribution 1. Conception and design of study 2. Acquisition of data 3. Data analysis 4. Discussion of results 5. Drafting of the manuscript 6. Approval of the final version of the manuscript DM has contributed in 2.4 and 5. GMF has contributed in 1, 3, 4, 5, and 6.
Received: August 08, 2021; Accepted: February 16, 2022
 Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
