










Serviços Personalizados
Journal

Artigo
 texto em
texto em  Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
Links relacionados
Compartilhar

 Permalink
PermalinkOdontoestomatología
versão impressa ISSN 0797-0374versão On-line ISSN 1688-9339
Odontoestomatología vol.24 no.39 Montevideo jun. 2022 Epub 20-Abr-2022
https://doi.org/10.22592/ode2022n39e309
Update
Clinpro XT resin-modified polymerizable glass ionomer varnish: an alternative treatment for tooth sensitivity. A systematic literature review

1Facultad de Odontología, Universidad de Concepción, Chile. 4030000. montsesm85@gmail.com
2Departamento de Prevención y Salud Pública de Facultad de Odontología, Universidad de Concepción, Chile.
Introduction:
Multiple products have been developed to treat dentin sensitivity, including Clinpro XT, a lightcuring resinmodified ionomer glass varnish with fluoride, calcium, and phosphate.
Methodology:
A systematic literature review was conducted. The articles were selected based on title, abstract, and full text according to the inclusion and exclusion criteria.
Results:
Of 299 articles, systematic reviews, metaanalysis, in vivo and in vitro studies, and 2 surveys were selected.
Discussion
Clinpro XT reduces dentin permeability, occludes dentin tubules, inhibits their reopening, increases mineral bioavailability in saliva, and promotes enamel remineralization. This entails greater protection of enamel and dentin immediately and in the long term.
Conclusions:
Clinpro XT was shown to decrease dentin hypersensitivity even six months after application.
Keywords: calcium; phosphates; glassionomer cements; dentin sensitivity; dentin desensitizing agents; Clinpro XT
Introducción:
En respuesta a la sensibilidad dentinaria, se han desarrollado múltiples productos, entre ellos, Clinpro XT, barniz de vidrio ionómero modificado con resina fotopolimerizable con flúor, calcio y fosfato.
Metodología:
Se realizó una revisión sistemática de la literatura. La selección fue en base a título, resumen y texto completo de acuerdo a los criterios de inclusión y exclusión.
Resultados:
De 299 artículos, fueron seleccionados revisiones sistemáticas, metaanálisis, estudios in vivo e in vitro y 2 encuestas.
Discusión:
Clinpro XT reduce la permeabilidad dentinaria, ocluye túbulos dentinarios e inhibe su reapertura, aumenta la biodisponibilidad de minerales en saliva y promueve la remineralización del esmalte. Significando una mayor protección del esmalte y dentina de forma inmediata y a largo plazo.
Conclusiones:
Clinpro XT demostró disminuir la hipersensibilidad dentinaria incluso después 6 meses posterior a su aplicación.
Palabras claves: Calcio; fosfatos; cemento de iónómero de vidrio,sensibilidad dentina; agentes sensibilizadores de dentina; Clinpro XT
Introdução:
Em resposta à sensibilidade dentinária, foram desenvolvidos múltiplos produtos, incluindo Clinpro XT, um verniz de vidro de ionómero modificado com resina fotopolimerizável com flúor, cálcio, e fosfato.
Metodologia:
Foi realizada uma revisão sistemática da literatura. A selecção foi baseada no título, resumo e texto completo de acordo com os critérios de inclusão e exclusão.
Resultados:
De 299 artigos, revisões sistemáticas, meta-análises, estudos in vivo e in vitro e 2 inquéritos foram seleccionados.
Discussão:
Clinpro XT reduz a permeabilidade da dentina, oclui os túbulos dentinários e inibe a sua reabertura, aumenta a biodisponibilidade dos minerais na saliva e promove a remineralização do esmalte. O que significa uma maior protecção do esmalte e da dentina imediatamente e a longo prazo.
Conclusões:
Foi demonstrado que o Clinpro XT diminui a hipersensibilidade da dentina mesmo 6 meses após a aplicação.
Palavras-chave: Cálcio; Fosfatos; Cimentos de Ionómero de Vidro; Sensibilidade Dentina; Agentes Desensibilizadores da Dentina; Clinpro XT
Dentin sensitivity (DS) is a short, sharp pain triggered by thermal, evaporative, tactile, osmotic, or chemical stimuli that cannot be attributed to another form of dental pathology.1 Physiological and morphological studies have shown that dentin sensitivity in noncarious cervical lesions (NCCL) is caused by the exposure of dentinal tubules to the oral environment.2,3
Advances in oral health have made it possible to preserve the teeth in the oral cavity for longer. Additionally, DS has increased,4 with a prevalence of between 1.34% and 82.1%, depending on the population, methodology,5 and diagnostic criteria used.6 The most common age range for DS is between 20 and 50 years.7,8 It appears mainly in female patients,2,7,9 and canines and first premolars are the most frequently affected teeth given their prominent position in the maxillary and mandibular arches.7
This clinical condition can disrupt and restrict people’s daily activities, such as during social interaction, eating, and drinking,1,10 toothbrushing, and even breathing,6 which negatively affects the quality of life.10-12
The most widely accepted theory on the DS mechanism was outlined in Brannstrom’s hydrodynamic theory. He states that tactile, chemical, osmotic, and thermal stimuli on exposed dentinal tubules cause a flow of fluid in the tubules towards or away from the pulp. This stimulates the mechanoreceptors that cause the sensation of pain.13
The aetiological factors of DS and exposure of dentinal tubules to the oral environment by loss of enamel or periodontal tissues14 are stress (abfraction caused by parafunction, disorders, and occlusal loads), corrosion by extrinsic and intrinsic acids (gastrooesophageal diseases and dietary habits), and friction (abrasion with toothbrush or toothpaste).7
In young adults, it has been attributed to erosive factors affecting the enamel, while gingival recession and root surface exposure are the leading causes in older populations. Diagnosis is based on ruling other conditions that cause orofacial pain such as caries, pulpitis, weak dental restorations, postoperative sensitivity, marginal seepage, and gingival inflammation.9
The treatment begins by identifying the aetiological factors, which must be eliminated for effective longterm results. The clinician should investigate and monitor occlusal factors (distribution of occlusal contact and parafunctional habits), oral hygiene habits (brushing technique, strength, and toothpaste), and the presence of acids from different sources in the oral cavity (acid diet and gastrooesophageal disorders).7 Dietary advice and oral hygiene instructions should be provided. Exposed dentin can then be safely managed and treated based on the size of the lesion and the patient’s sensitivity.9
Two treatment approaches—chemical and physical—aim at reducing fluid flow by sealing or occluding dentinal tubules,8 or depolarizing pulp nerve fibers.15 The first entails using household agents such as toothpaste and gels, and mouthwash to a lesser extent.16 The physical approach includes inoffice treatments with adhesives, glassionomer cement (GIC) and sealants, topical application of products containing sodium fluoride, stannous fluoride, potassium nitrate, oxalates, calcium phosphate, oxalic acid (phytocomplexes), arginine/calcium carbonate and bioglass (calcium and sodium phosphosilicate),14 glutaraldehyde, laser therapy, among others.6
Although DS is a widespread dental problem, there are no universally accepted guidelines for differential diagnosis and treatment selection.17 This is reflected in a study conducted in Brazil, where 29% of dentists report not knowing the different classifications of dental desensitizers, including 3.4% who did not know any type, regardless of how long they had been working. Over 80% of the dentists included seemed concerned about dentinsensitivity issues and considered managing the condition a challenge in daily dental practice.6 Along these lines, a study from the United Kingdom showed that 72% of dentists consider it a dilemma.9 Fifty percent of Canadian dentists and hygienists surveyed were not confident in managing dentin sensitivity.17
Desensitizing agents form precipitates or barriers that can be eliminated or dissolve between applications or shortly after that.16 This makes their duration problematic since many do not have a permanent effect because they cannot adequately adhere to the dentin surface.15 Longterm efficacy remains a challenge, as the agents must withstand exposure to various acidic and abrasive challenges in the oral environment.4,16
These drawbacks can be overcome with a minimally invasive material that has an instantaneous effect, used in a single application following an easy and fast protocol. The product should provide longterm efficacy and resist exposure to acid and abrasive challenges of the oral environment.
GIC is a very popular restorative material due to its chemical bonding and fluoride-releasing ability. It provides satisfactory longterm results, especially in the treatment of NCCL. However, conventional GICs are relatively unaesthetic and have some mechanical disadvantages compared to composite resin.15
Resinmodified GICs have been developed to address this issue: they are more tolerant to moisture and have improved ion exchange with the dental substrate, with sustained fluoride release.3
Clinpro XT is a desensitizing glassionomer varnish modified with lightcuring resin containing fluoride, calcium, and phosphate. It is a chemical agent with occlusive action.7 It seals dentinal tubules through the chemical adhesion to dentin4 provided by polyalkenoic acid, which forms ionic bonds with calcium hydroxyapatite, the primary mineral in dentin.10 There follows a chelation mechanism where the carboxylic groups of the polyacrylic acid in Clinpro XT react with the enamel calcium and the dentin apatite. It also contains calcium glycerophosphate, which allows for increased bioavailability of calcium and phosphate in saliva.12 The calcium released from coating or restorative materials may contribute to hardening enamel surfaces.18 Studies report that Clinpro XT releases fluoride in saliva for up to six months.4 Enamel has increased resistance to acid when fluoride is incorporated into the apatite. This reduces enamel degradation.7
The polymerizable monomeric functional group significantly increases the product’s strength when lightactivated.8 It forms stable salts with calcium ions, causing the airtight seal to act as a physical barrier and protect the enamel from acid erosion.18 These characteristics make it an immediate treatment that has longterm efficacy to address DS.4,8
Therefore, this study aims to review the available literature on Clinpro XT—the resinmodified ionomer glass varnish—systematically and thoroughly to determine if it is an efficient option to treat dental sensitivity.
Materials and methods
The study was conducted following the PRISMA statement and its 27 items; we considered its recommendations in each phase of conducting and publishing systematic reviews. The search strategy for the studies entails identifying all the papers published in the last five years, up to August 2020, on hypersensitivity treatment and management with Clinpro XT resinmodified ionomer glass varnish.
The following search terms were used for the two components:
- About dentin sensitivity: dentin sensitivity
- About products or treatments for sensitivity: Calcium, phosphates, glassionomer cements, dentin desensitizing agents, and Clinpro XT.
The search was performed in PUBMED and SCIELO with the search algorithm ((((calcium) OR (Phosphates)) AND (Glass Ionomer Cements)) AND (Dentin Sensitivity)) OR (Dentin Desensitizing Agents) AND “Clinpro XT.”
The papers were added to Mendeley reference manager, where duplicates were eliminated.
Inclusion and exclusion criteria
a) Inclusion criteria: in vivo, in vitro studies, systematic or narrative literature reviews, metaanalyses, and surveys on dentin sensitivity and its management with varnishformat resinmodified ionomer glass published in the last five years, without geographic or linguistic limitations.
b) Exclusion criteria: published studies that do not meet the inclusion criteria, where the dental substrate has been bleached, or if there is no access to the full text.
Study selection
The researchers selected the articles independently and in three phases: reading the title, the abstract, and the full text. The results were compared. When there was disagreement about the studies, the researchers reviewed the inclusion and exclusion criteria together. The results of the final selection are presented below.
Data extraction
A data extraction form including the following items was designed:
- Bibliographic information: first author, year of publication.
- Type of study: Systematic review, metaanalysis, in vivo study, in vitro study, survey.
- Study characteristics: date of study, sample size, longevity studies, effective pain management, mechanism of action, perception, and problems for the dentist.
- Main objective.
- Main results.
Results
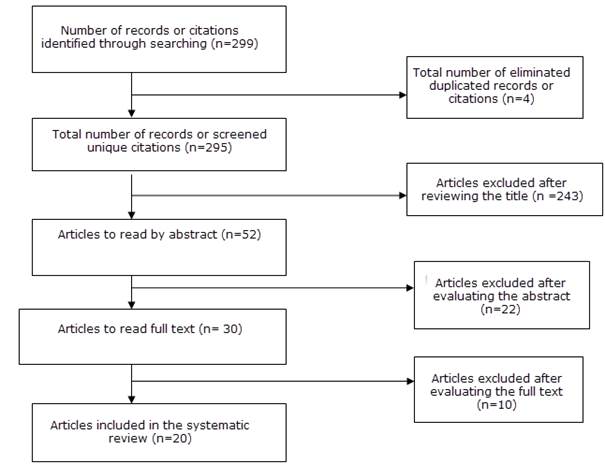
Of 299 articles found, 20 met the inclusion and exclusion criteria, including 4 systematic reviews, 2 metaanalyses, 5 in vivo studies, 7 in vitro studies, and 2 surveys.
Clinpro XT was evaluated for efficacy in reducing dentin permeability (DP), dentinal tubule occlusion, resistance to erosive and abrasive challenges, and changes in dentin surface morphology and roughness.
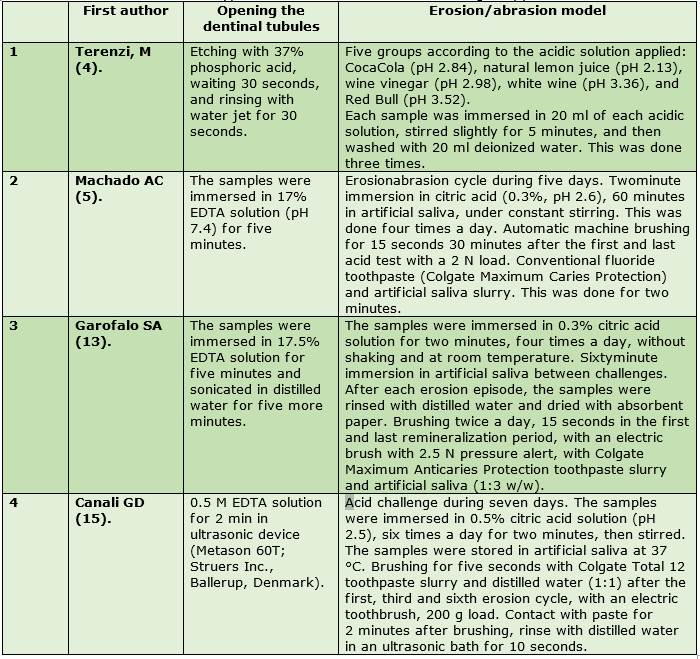
Table 1 describes the methodology used in the in vitro studies to simulate DS: opening the dentinal tubules with phosphoric acid gel and/or EDTA solution, respectively. They obtained maximum permeability4,5,14,16 and the necessary erosion/abrasion models.
Dentin permeability and resistance to erosive/abrasive challenges
Dentin permeability decreased significantly after applying Clinpro XT as protection from the acid challenges described in case 1 (Table 2). The general population widely consumes these acidic solutions. None of these acidic solutions increased DP significantly. Clinpro XT showed excellent acid resistance during very intense contact that does not occur in routine clinical conditions, but rather with a diet with excessive acid consumption and/or in patients with severe hyposalivation.4
The reduction in DP after a single application of Clinpro XT can be explained by the occlusion or sealing effect of the product on the exposed dentinal tubules, which was confirmed by SEM analysis. We may infer that Clinpro XT has the potential to reduce sensitivity by preventing displacement of the tubular contents.4
All the DS treatments applied—Clinpro White Varnish, Clinpro XT Varnish, Tooth Desensitizer, Nano P, Nupro, Duraphat—managed to reduce DP compared to the untreated control group. However, after the erosive/abrasive cycle described in item 2 (Table 2), there were no significant differences in DP and the number of obliterated dentinal tubules between the groups. This implies that the treatments could not withstand the five days of erosive and abrasive challenges. Varnishes were expected to perform better given their higher chemical adhesion to the dentin surface and fluoride, calcium, and phosphate release. The authors suggest that the number of erosive episodes jointly with toothbrushing may have promoted a more vigorous removal of Clinpro XT varnish from the surface. In addition, the study acknowledges its limitations due to the small study area.5
Under the erosion/abrasion model proposed in case 4 (Table 2), DP was similar to the minimum DP in all phases of the study. The same result was obtained with Fluor Protector, and the result was significantly lower than the DP obtained with OxaGel and NanoP after days 4 and 7 of the challenge. This erosion/abrasion challenge simulates a high consumption of acidic beverages combined with regular toothbrushing.16
Scanning electron microscopy (SEM) analysis
Morphological changes
Samples etched with 37% phosphoric acid gel for 30 seconds and washed with water jet for 30 seconds were analyzed with SEM before and after treatment with Clinpro XT. A statistically significant reduction in surface roughness was observed after a single application. This shows that the product is highly effective in occluding dentinal tubules. The surface of the samples from the control group (etching only) had fully open dentinal tubules, while the dentinal samples treated with Clinpro XT showed fully occluded dentinal tubules. This result proves that Clinpro XT would not facilitate dental plaque accumulation from a clinical perspective. However, this experimental design did not consider the possible protective effect of saliva or resistance to brushing procedures.4
Clinpro XT achieved complete obliteration of the dentinal tubules, gradual resin matrix degradation, and glass particles detachment four days after the erosion/abrasion challenge proposed in case 4 (Table 2). The SEM micrographs of the dentinal surface showed a continuous layer obliterating the dentinal tubules during the sevenday erosion/abrasion model, despite the slight deterioration of the surface layer caused by the detachment of some particles. The obliteration pattern could be attributed to resin compounds in the base rather than to the availability of fluoride ions for DP reduction.15
Qualitative and quantitative analysis of open dentinal tubules (ODT)
After applying Clinpro XT, almost no dentinal tubules could be counted qualitatively or quantitatively. These results support the efficacy of calcium phosphate compounds in occluding dentinal tubules, which could be associated with immediate inoffice pain relief. However, a limitation of the study was using a toothpaste containing sodium monofluorophosphate, since this compound requires the enzymatic breakdown of saliva to release fluoride. Toothpaste fluoride is not expected to have a significant role in promoting tubule occlusion.5
The samples of case 3 were analyzed after opening the tubules with EDTA, applying Clinpro XT, and the erosion/abrasion cycle (Table 2) qualitatively and quantitatively. It was found that the number of open dentinal tubules (ODT) was lower after treatment with Clinpro XT. Furthermore, it showed fewer ODT after the cycle than the untreated control group. No surface loss was detected, and there was resistance to the erosive/abrasive challenges, which were intended to simulate the clinical situation of patients with DS. We believe that Clinpro XT released calcium, phosphate, and fluoride into the acidic solution during the erosive challenge, increasing its saturation of dental minerals, thus reducing demineralization. It could release these ions in saliva, increasing remineralization. This may have had a protective effect against erosive dentin wear.14
Inhibition of demineralization
Clinpro XT was evaluated to determine its ability to inhibit demineralization and elemental, inorganic enamel content after treatment. To this end, clinical situations were replicated using a pH regime that simulates demineralization and remineralization episodes in the oral cavity.19 In this context, the product did not inhibit the initial demineralization promoted by the pH cycle, which is consistent with current knowledge on the physicochemical effect of fluoride on caries control: it reduces demineralization but does not prevent it. The demineralization process was less generalized than that of the untreated group, which proves its protective effect.18,19
Studies claim that adding calcium and phosphorus ions to an ionomerglass material increases its availability to bind released fluoride ions. The results point to a synergistic effect of fluoride and the ions released, promoting greater enamel protection. In addition, a lower percentage of calcium and phosphorus was found in the untreated group after the pH cycling regimen. Hydroxyapatite dissolution and mineral loss were confirmed in the absence of remineralizing materials. This influences the mechanical properties of the tooth that depend on the mineralization of hydroxyapatite, where lower Ca/P values indicated less mineralization.19
Efficacy and longevity of pain reduction
Pain is subjective, and assessing the therapeutic effect of a DS treatment can be difficult.15 The VAS scale has proven accurate in recording patient responses.3
The efficacy of three desensitizing agents—Desensibilize KF, Cinpro XT, and Photon Laser III—was evaluated after 4 application sessions with a 24week followup. The three groups had a statistically significant reduction in DS levels from baseline to subsequent followups. After the fourth treatment session, no significant differences in pain were found between treatments, regardless of the evaluation point. In addition, no adverse effects or clinical complications, such as pulp disease or allergic reactions, were reported during the study period. The efficacy of desensitizing agents was maintained at 2, 4, 8, and 24 weeks of followup.8
A randomized clinical trial evaluated the longterm clinical outcome of Clinpro XT compared to a conventional CVI (Vidrion R). It was a splitmouth study with the sagittal midline as a reference. The results showed that both treatments decreased pain symptoms immediately after one application. The effects lasted six months, proving that Clinpro XT was equivalent to conventional CVI up to six months after treatment.15)
We must emphasize the clinical advantages of Clinpro XT compared to conventional IVC. Resinmodified ionomer glass is easy to use; it does not require a rubber dam and is moisture tolerant. This facilitates its clinical use in regions that require strict control, such as in roots, has better esthetic properties, and therefore patients prefer it. Both materials showed similar results in DS reduction. Thus, the practitioner should evaluate which material would be the most suitable for each clinical case, considering factors such as retention rate, staining, gingival response, and plaque accumulation.15
The study that comparatively evaluates the efficacy of Clinpro XT varnish versus Icon resin infiltration in restoring the esthetics of enamel affected by white spot lesions after orthodontic treatment shows that Clinpro XT immediately increased the brightness of the white spots significantly after its application. This improved the optical properties immediately. Both Icon resin infiltration and Clinpro XT varnish provided immediate esthetic results in mild lesions. In moderate lesions, however, although there were progressive improvements in both groups, clinical longterm visible improvements were more frequent with Clinpro XT.20
A study evaluated the efficacy of MI protective varnish and Clinpro XT varnish in DS reduction with a oneweek followup. The MI Varnish had a statistically significant difference over the Clinpro XT Varnish group in reducing dentin hypersensitivity when comparing the values of cold test scores. Although both show a decrease in dentin hypersensitivity, statistically, MI Varnish is a better treatment option when compared to Clinpro XT Varnish. However, the authors acknowledge that this is a oneweek followup study. Studies with a longer observation time frame and sound design are required to help determine how often the varnish should be reapplied.3
One point to consider is that the results may depend on the clinician applying the treatment, as their clinical experience and the correct management of the patient’s needs impact the outcome. In addition, the literature reports a significant psychological component in dentin hypersensitivity. DS management remains inconclusive in the literature. Evaluations with longer followup times are required to analyze stability and longevity, and further clinical investigations are needed on the number of application sessions and clinician experience levels.8
Conclusions
Based on the literature analyzed in this systematic review, it can be concluded that Clinpro XT occluded dentinal tubules, effectively reduced permeability by resisting abrasive or acidic stimuli, and inhibited tubule reopening after erosive/abrasive challenges. Additionally, there was a statistically significant reduction in surface roughness after a single application. Furthermore, the product increased the bioavailability of calcium and phosphate in saliva, demonstrated its ability to release fluoride in saliva over six months, promoted enamel remineralization, partially inhibited enamel demineralization by acid challenge, which meant greater immediate and longterm enamel protection from DS.
Clinically, Clinpro XT managed pain satisfactorily in treating dentin hypersensitivity for up to six months postapplication. It also improved the optical properties of mild and moderate white lesions immediately and in the long term.
Further clinical studies are needed to extrapolate the invitro results to the product’s clinical performance.
REFERENCES
1. Tenuta LMA, Cury JA. Fluoride: its role in dentistry. Braz Oral Res. 2010; 24 (Suppl 1):9 -17. [ Links ]
2. Estupiñán-Day S. Promoting oral health: the use of salt fluoridation to prevent dental caries. Washington: PAHO, 2005. [ Links ]
3. Horowitz HS. Decision-making for national programs of community fluoride use. Community Dent Oral Epidemiol. 2000; 28(5):321-9. [ Links ]
4. Marthaler T, Petersen P. Salt fluoridation- an alternative in automatic prevention of dental caries. Int Dent J. 2005;55(6):351-8. [ Links ]
5. Ditterich RG, Rodrigues CK, Wambier DS. Fluoride salt as a alternative in public oral health: advantages and disadvantages. Rev Inst Ciênc Saúde, 2005; 23(3): 231-4 [ Links ]
6. Uruguay. Ministerio de Salud Pública. Comisión Honoraria de Salud Bucal. Encuesta de Salud Bucal en escolares de 11 a 14 años. Sector Público, 1999 [ Links ]
7. Martínez-Mier EA, Soto Rojas AE, Buckley CM, Stookey GK, Zero DT, Margineda J. Evaluación del contenido de flúor en la sal de mesa fluorada. Salud Pública Mex. 2004 May-Jun; 46(3):2003-4. [ Links ]
8. Walsh K I and Cury J A. Fluoride concentrations in salt marketed in Managua, Braz. Oral Res. 2018;32: e45 [ Links ]
9. Hernández-Guerrero JC, Fuente-Hernández J, Jiménez-Farfán MD, Ledesma-Montes C, Castañeda-Castaneira E, Molina-Frechero N, et al. Fluoride content in table salt distributed in Mexico City, Mexico. J Public Health Dent. 2008; 68(4):242-5. [ Links ]
10. Franco AM, Saldarriaga A, Gonzalez MC, Martignon S, Arbelaez MI, Ocampo A. Concentración de fluor en la sal de cocina en cuatro ciudades colombianas. Revista CES Odontología 2003;16: 21-6. [ Links ]
11. Tovar Valencia S, Castrillon Misnaza S. Perspectiva del uso del flúor vs caries y fluorosis dental. Colombia: Minsalud; 2016 [cited 2017 Sep 29] Disponible en: http://www.minsalud.gov.co/sites/rid/Lists/Bibliotecadigital/RIDE//VS/PP/ENT/perspectiva-uso-fluor.pdf. [ Links ]
12. Walsh KI, Cury JA. Fluoride concentrations in salt marketed in Managua, Nicaragua. Braz Oral Res. 2018; 24, 32:e45. [ Links ]
13. Mier EAM, Rojas AES, Buckley CM, Margineda J, Zero DT. Evaluation of the direct and diffusion methods for the determination of fluoride content in table salt. Community Dent Health, 2009; 26(4): 204-10. [ Links ]
14. Marthaler TM. Salt Fluoridation and Oral Health. Acta Medica Academica, 2013; 42(2): 140-55. [ Links ]
15. Sagheri D, Mcloughlin J, Clarckson J J. A comparison of dental caries levels in two communities with different oral health prevention strategies stratified in different social classes. Journal of Public Health Dentistry, 2007; 67(1): 1-7. [ Links ]
16. Fabruccini A, Alves LS, Alvarez L, Alvarez R, Susin C, Maltz M. Comparative Effectiveness Of Water And Salt Community-Based Fluoridation Methods In Preventing Dental Caries Among Schoolchildren. Community Dent. Oral Epidemiol, 2016; 44(6): 577-85. [ Links ]
17. Mejía R, Espinal F, Vélez H, Aguirre M. Fluoruración de la sal en cuatro comunidades colombianas. VIII. Resultados obtenidos de 1964 a 1972. Bol Oficina Sanit Panam. Colombia, 1976; 80: 205. [ Links ]
18. Alsayed EZ, Hariri I, Nakashima S, Shimada Y, Bakhsh TA, Tagami J, et al. Effects of coating materials on nanoindentation hardness of enamel and adjacent areas. Dent Mater. 2016;32(6):807-16. [ Links ]
19. Scotti CK, Velo MM de AC, Brondino NCM, Guimarães BM, Furuse AY, Mondelli RFL, et al. Effect of a resin-modified glass-ionomer with calcium on enamel demineralization inhibition: an in vitro study. Braz Oral Res. 2019;33(0):e015 [ Links ]
20. Kannan A, Padmanabhan S. Comparative evaluation of Icon® resin infiltration and ClinproTM XT varnish on colour and fluorescence changes of white spot lesions: a randomized controlled trial. Prog Orthod. 2019;20(1):23 [ Links ]
Conflict of interest declaration: The authors have no conflict of interest regarding the publication of this paper.
Authorship contribution: 1. Conception and design of study 2. Acquisition of data 3. Data analysis 4. Discussion of results 5. Drafting of the manuscript 6. Approval of the final version of the manuscript SM has contributed in 1, 2, 3, 4, 5, 6. UP has contributed in 1, 2, 3, 4, 5, 6. AC has contributed in 1, 4, 5, 6.
Received: May 19, 2021; Accepted: November 30, 2021
 Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
