










Serviços Personalizados
Journal

Artigo
 texto em
texto em  Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
Links relacionados
Compartilhar

 Permalink
PermalinkOdontoestomatología
versão impressa ISSN 0797-0374versão On-line ISSN 1688-9339
Odontoestomatología vol.24 no.39 Montevideo jun. 2022 Epub 01-Ago-2022
https://doi.org/10.22592/ode2022n39e307
Update
Oxidative stress in saliva induced by tobacco smoke: impact on periodontitis and perspectives with redox pharmacology

1Centro de Investigaciones Biomédicas, Facultad de Medicina, Universidad de la República. Uruguay
2Departamento de Bioquímica, Facultad de Medicina, Universidad de la República. Uruguay
3Departamento de Nutrición Clínica, Escuela de Nutrición, Universidad de la República. Uruguay
4Cátedra de Bioquímica y Biofísica, Facultad de Odontología, Universidad de la República. Uruguay. valeriavalez@odon.edu.uy
Numerous reports demonstrate the presence of oxidative stress biomarkers in the saliva of smokers and there is a growing interest in correlating these molecular processes with the etiology of some oral diseases, such as periodontitis, a chronic immunoinflammatory disease related to an imbalance of cellular redox homeostasis.
Aims:
Achieve a narrative review on the relationship between the decrease in salivary antioxidant capacity induced by tobacco smoke, periodontitis, and the potential use of redox pharmacology for the treatment of this pathology.
Methods:
A bibliographic search was carried out in databases such as PUBMED (NLM, NIH, NCBI) and SciELO.
Results:
There is evidence that relates the low salivary antioxidant capacity with a delay in the reestablishment of normal conditions in the oral cavity before the development of periodontitis. In turn, the associated inflammatory state collaborates synergistically, causing greater tissue damage with loss of dental support tissues, a phenomenon that could be modulated by the action of redox pharmacology.
Conclusions:
Intervention with redox pharmacology could attenuate the biomarkers of periodontal disease progression, constituting a promising tool to be used in conjunction with traditional treatment strategies.
Keywords: cigarette smoke; oxidative stress; periodontal disease; saliva; redox medicine; periodontitis
Numerosos reportes demuestran la presencia de biomarcadores de estrés oxidativo en la saliva de fumadores y hay un creciente interés en correlacionar estos procesos moleculares con la etiología de algunas enfermedades orales, como la periodontitis, una enfermedad inmunoinflamatoria crónica relacionada con un desequilibrio de la homeostasis redox celular.
Objetivo:
realizar una revisión narrativa sobre la relación entre la disminución de la capacidad antioxidante salival inducida por humo de tabaco, la periodontitis y el potencial uso de farmacología redox para el tratamiento de esta patología.
Métodos:
se realizó una búsqueda bibliográfica en bases de datos como PUBMED (NLM, NIH, NCBI) y SciELO.
Resultados:
existe evidencia que relaciona la baja capacidad antioxidante salival con un retraso en el restablecimiento de las condiciones normales en la cavidad oral ante el desarrollo de periodontitis. A su vez, el estado inflamatorio asociado colabora sinérgicamente, provocando un mayor daño tisular con pérdida de tejidos de soporte dentario, fenómeno que podría ser modulado por la acción de farmacología redox.
Conclusiones:
la intervención con farmacología redox, podría atenuar los biomarcadores de progresión de la enfermedad periodontal, constituyendo una herramienta prometedora para utilizar en conjunto con las estrategias de tratamiento tradicionales.
Palabras clave: humo de cigarrillo; estrés oxidativo; enfermedad periodontal; saliva; farmacología redox y periodontitis
Muitos artigos demonstram a presença de biomarcadores de estresse oxidativo na saliva de fumantes e há um interesse crescente em correlacionar esses processos moleculares com a etiologia de algumas doenças bucais, como a periodontite, uma doença imunoinflamatória crônica relacionada a um desequilíbrio da redox celular homeostase.
Objetivo:
realizar uma revisão narrativa sobre a relação entre a diminuição da capacidade antioxidante salivar induzida pela fumaça do tabaco, periodontite e o uso potencial da farmacologia redox para o tratamento desta patologia.
Métodos:
uma pesquisa bibliográfica foi realizada usando bases de dados como PUBMED (NLM, NIH, NCBI) e SciELO. Resultados: há evidências que relacionam a baixa capacidade antioxidante salivar com o retardo no restabelecimento das condições normais da cavidade oral antes do desenvolvimento da periodontite. Por sua vez, o estado inflamatório associado colabora sinergicamente, causando maior dano tecidual com perda de tecidos de suporte dentário, fenômeno que poderia ser modulado pela ação da farmacologia redox.
Conclusões:
a intervenção com a farmacologia redox poderia atenuar os biomarcadores de progressão da doença periodontal, constituindo-se em uma ferramenta promissora para ser utilizada em conjunto com estratégias tradicionais de tratamento.
Palavras-chave: fumaça de cigarro; estresse oxidativo; doença periodontal; saliva; redox farmacologia e periodontite
Introduction
The oral cavity is an open system and therefore its consequent exchange of energy and matter with the environment must be considered. It is directly exposed to numerous environmental factors such as: food, alcohol, cigarette smoke, drugs, toxins, pathogenic microorganisms, among others 1. The presence of saliva is of vital importance for the maintenance of the health of teeth and soft tissues and is recognized as a reflection of the state of health, due to the fact that it contains proteins, hormones, antibodies composition and other molecules that serve to monitor the overall health status of the individual 2-3. Among the functions of saliva, a very important one is that it constitutes the first defense barrier against external damage agents 1. Saliva is essential for maintaining the health of teeth and soft tissues and is recognized as a reflection of the health condition since it includes proteins, hormones, antibodies, and other molecules that help monitor the individual's general health 2-3. Saliva contains a battery of proteins and compounds with antioxidant capacity that counteract the effects of external and internal oxidizing agents that affect the oral cavity 2-4. Cigarette smoking has a high impact on the composition and function of saliva. In its composition, different oxidizing agents and radical compounds challenge endogenous antioxidant systems in saliva, which, despite their high efficiency, may be insufficient to prevent the repercussions of exposure to tobacco smoke. Consequently, the accumulation of oxidative modifications leads to an imbalance of redox metabolism, determining the appearance of oxidative stress markers such as nitrated or oxidized proteins, lipid peroxidation products, among others, evidenced in numerous reports in smokers 4. In addition, there is a growing interest in the study of the role played by reactive species in the etiopathogenic mechanisms of some oral diseases. In this sense, periodontitis is precisely a disease closely related to an imbalance of redox homeostasis, where the induction of oral dysbiosis and the established inflammatory state collaborate in the formation of more oxidant species and free radicals that damage cellular components 5-6. In this type of pathology, saliva with low antioxidant capacity makes it difficult to restore the salivary redox state and acts synergistically with the underlying proinflammatory state, causing greater tissue and dental damage 7. Therefore, the incorporation of redox pharmacology in the clinical treatments of periodontitis is postulated as a novel alternative to counteract the effects of oxidative stress established in this pathology, attenuating the progression of the disease.
Aims
Carry out a narrative review on the relationship between the production of reactive species and the decrease in salivary antioxidant capacity induced by tobacco smoke. Review the accumulated evidence on oxidative stress in periodontitis and the potential use of redox pharmacology for the treatment of this pathology.
Review and methods
A narrative review was carried out from the PUBMED (NLM, NIH, NCBI) and SciELO databases, with original articles published between 2012-2021 for the subject under study and the original references of some fundamental concepts of redox biology were added. academic relevance not included in this period. To search for articles, the following terms were used: “periodontitis”, “oxidative stress”, “redox pharmacology”, “salivary antioxidants”, “periodontal disease”, “cigarette smoke” and “saliva”. 121 articles were found, of which 50 were included after filtering by title, abstract and full text. Both animal model studies and human studies were included.
Oxidative stress in biological systems
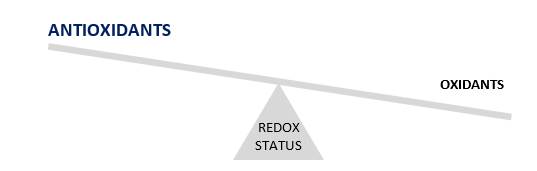
The concept of oxidative stress, coined by Helmut Sies, 8 was introduced just over 30 years ago, encompassing a spectrum of situations in which an imbalance occurs between oxidant formation and cellular antioxidant capacity, in favor of oxidants, leading to redox signaling disruption and molecular damage (Fig. 1) 9-10. The formation of oxidants at the cellular level occurs, in part, because of aerobic metabolism, although it can also occur as a result of environmental exposure to oxidizing agents such as UV radiation, tobacco smoke, smog, among others. Oxidants produced can react with biomolecules, leading to modifications that determine changes in structure and function, generating cell damage. On the contrary, these processes are attenuated by enzymatic and non-enzymatic antioxidant systems 10-11. When these antioxidant systems collapse or are overwhelmed by oxidants, a condition of cellular oxidative stress is established. In recent years, the study of the role of reactive species has led to the incorporation of the concepts of eustres or oxidative distress as substitutes for the concept of oxidative stress. In this way, an attempt is made to discriminate the physiological or pathological roles of the redox imbalance, respectively 12-13.
What are free radicals?
A free radical is a molecule containing an unpaired electron in its outermost orbital. They are short half-life (micro- to milliseconds) and very reactive intermediates (they accept or donate electrons) 11-14. Free radicals and other oxidizing molecules are called “reactive species” and can be derived from oxygen, nitrogen, and other elements 15. They are formed under normal and pathological conditions, and cells have developed different antioxidant systems to attenuate their biological effect. Below we describe the most relevant reactive oxygen and nitrogen species in biological systems.
Reactive oxygen species
The term “reactive oxygen species” (ROS) includes oxygen radicals and some non-radical derivatives 16 and in Diagram 1, the one-electron reduction sequence of molecular oxygen is shown.
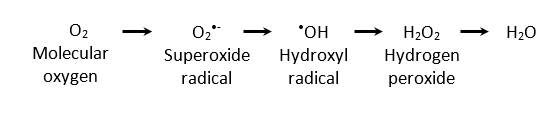
Under normal conditions, the main cellular source of ROS is mitochondrial respiration, generating superoxide anion radical (O2•-) as a by-product of the flow of electrons through the electron transport chain 17. Detoxification of this radical can be spontaneous or enzymatic by the action of superoxide dismutases (SODs, MnSOD, or CuZnSOD), which yields hydrogen peroxide (H2O2). H2O2 is not a free radical because it does not contain unpaired electrons, is more stable than O2•- with a half-life in the order of ~1 ms, and under stationary conditions, it reaches a cell concentration of ~10-7 M 18. Consequently, O2•- is normally consumed at the site of formation generating H2O2 by SOD-mediated enzymatic dismutation (16). Once H2O2 is formed, it can diffuse through membranes reaching different compartments than the site where it is generated. In aerobic organisms, H2O2 is metabolized to water and O2 mainly by two enzyme systems: catalase (CAT) and glutathione peroxidase (GPx). The hydroxyl radical (•OH) is a highly reactive molecule that can oxidize amino acids, lipids, and nucleic acids, resulting in a short half-life (~10-9 s) and a low diffusion capacity 19. It is generated via the Haber-Weiss cycle in presence of proteins containing Fe or Cu metal centers and H2O2. Another source of this radical is the decomposition of the peroxynitrite anion (ONOO-), as explained below.
Reactive nitrogen species
Reactive nitrogen species (RNS) can be radicals or non-radicals. Those of highest interest in biology are nitric oxide (•NO), peroxynitrite anion (ONOO-), and nitrogen dioxide radical (•NO2). •NO is an uncharged molecule with a short half-life (3-5 s) and is considered one of the most important nitrogen radicals. In fact, its discovery earned the Nobel Prize in Physiology or Medicine for L. Ignarro, F. Murad, and R. Furchgott in 1998 20. It is not a strong reducer or oxidizer and therefore does not react rapidly with most biomolecules despite being a free radical (21). It is produced from L-arginine by the action of nitric oxide synthase enzymes (NOS), and the reaction involves N-hydroxy L-arginine as an intermediate. In the presence of O2•-, H2O2 and transition metal centers, it can generate other reactive oxygen species such as ONOO-. Physiologically, is an intracellular messenger and is the cytotoxic agent produced by activated macrophages and neutrophils, it regulates local blood flow, it is an inhibitor of platelet aggregation and adhesion and at low concentrations it works as an anti-inflammatory, but at high concentrations it acts as a pro-inflammatory 21. ONOO- is an anion produced from the rate limited reaction of •NO with O2•-. It is not a free radical, but it has a very short half-life in the order of 10-20 ms 22. It can be formed in biological systems and is a potentially toxic oxidant and nitrating agent 23. When there is an increase in O2•- generation, the reaction of •NO with O2•- is kinetically favored, and •NO competes with SOD for the removal of O2•- to form ONOO- (increased in pathological conditions). •NO2 is a toxic and highly reactive free radical that can nitrate lipids and proteins, causing cellular damage, as the nitration of significant amino acid residues in proteins can compromise its cellular function. It can be formed from the decomposition of ONOO- and from its reaction with CO2, which is very significant in biological systems. Additionally, it can also be formed through NO2- oxidation catalyzed by some peroxidases (e.g., myeloperoxidase) or by the autooxidation of •NO 24.
Free radical sources and cellular damage
Oxidants and free radicals are continuously produced during physiological activities in cells and can participate in redox signaling. Oxidative stress condition can be induced in biological systems by oxidants and radicals from both endogenous and exogenous sources (Fig. 2). In pathological conditions, the formation of these species can significantly increase and mediate oxidative damage to different biomolecules (lipids, carbohydrates, DNA, and proteins). The reactive species generated can cause DNA damage, modification and/or inactivation of proteins and carbohydrates, as well as lipid oxidation. To prevent this damage caused by free radicals, organisms, especially aerobes, have developed defense systems or antioxidant systems during evolution 1-25.
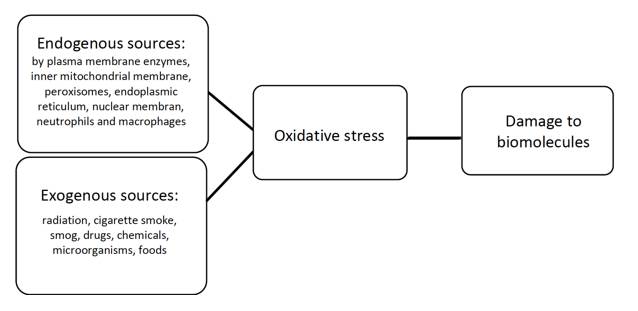
Fig. 2: Main sources of free radicals. They can be classified as endogenous or exogenous. The generation of ROS and RNS causes a redox off-balance in favor of the pro-oxidants, which damages biomolecules
In the case of the oral cavity, many reports on saliva describe antioxidant capacity globally as total oxidative status (TOS) 26. However, it is not specified which system or systems are affected; From then on, the most important antioxidant systems in saliva will be investigated.
Antioxidants in saliva
From a biomedical point of view, an antioxidant can be defined as a compound or protein that, even when is present at low concentrations compared to those of an oxidizable substrate, prevents or significantly delays the oxidation of the substrate initiated by a prooxidant (15-16). Antioxidants present in saliva can be classified as enzymatic or non-enzymatic antioxidant systems (Fig. 3):
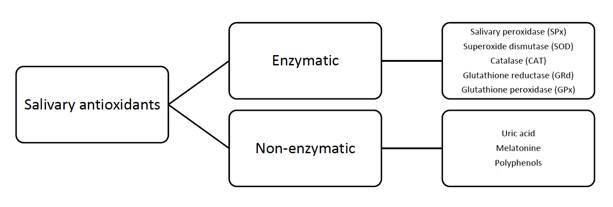
Fig. 3: Main antioxidants present in saliva. They are classified as enzymatic or non-enzymatic. They represent the main barrier against oxidant and radical damage because they exert their protective effect on teeth and the oral cavity tissues
Peroxidases are a family of enzymes that use different substrates as a source of electrons to reduce peroxides. Some of them have a specific substrate, such as reduced glutathione (GSH) for GPx, but most act on several substrates 27. In saliva, salivary peroxidase (SPx) catalyzes the formation of hypothiocyanate (OSCN-) and hypothiocyanous acid (HOSCN-) from hydrogen peroxide (H2O2) and thiocyanate (SCN-). H2O2 can be generated, as mentioned above, by the bacteria that colonize the oral cavity or through rinses and mouthwashes. The main function of SPx is believed to be to remove the H2O2 produced locally by bacteria. SODs are a family of metalloenzymes found in all aerobic organisms and the first enzymes to be involved in antioxidant defense. As mentioned above, SODs protect the cell from ROS by catalyzing the dismutation of O2•- to H2O2 27 being the most important O2•- detoxification pathway in biological systems. Catalases belong to a family of enzymes present in numerous tissues (e.g., abundant in liver cells). As mentioned above, it catalyzes formation of water and oxygen from H2O2 and plays a vital role in metabolism, preventing the alterations induced on proteins and nucleic acids 27. Glutathione peroxidases (Gpx) are a family of selenoenzymes expressed in most cells whose main biological activity is to protect the organism by detoxifying peroxides 27. GPx reduces H2O2 and other hydroperoxides to H2O using reduced glutathione (GSH) as a co-substrate and converting it to oxidized glutathione (GSSG) 28. The glutathione reductase (GRd) enzyme is part of a family of enzymes that catalyze the reduction of GSSG to GSH at the expense of NADPH, which mainly comes from the pentose phosphate pathway 27. One notable non-enzymatic antioxidant is uric acid (waste product of purine catabolism), which effectively eliminates energetically excited species such as singlet oxygen and peroxyl and hydroxyl radicals 16-29. Uric acid is the predominant antioxidant molecule in saliva, representing 85% of the total antioxidant capacity 30. In addition, melatonin, normally secreted by the salivary glands (although it can also be added as an external treatment) and whose maximum secretion is between 12:00 and 2:00 a.m. (following the circadian rhythm of the individual), can neutralize ROS mainly by removing H2O2 31-33. Therefore, it is suggested that its role is CAT and GPrx backup 31. In addition, polyphenols are important exogenous antioxidants obtained from the diet, which are present in various foods and beverages that have shown modulating the activity of the metabolism of reactive species in saliva 34-35.
Oxidative stress caused by tobacco smoke
It is reported that tobacco smoke contains many potentially toxic substances, with nicotine being considered one of the most dangerous and addictive. It also includes many prooxidative and carcinogenic substances. Smoke, a product of tobacco combustion, carries a wide variety of free radicals, making it one of the most powerful inducers of oxidative stress in the oral cavity 4-36. Tobacco smoke increases ROS levels, which are toxic to the human body because they change redox homeostasis 5. Cadmium in cigarette smoke can replace iron and copper in membrane-bound cytoplasmic proteins, thus increasing the amount of free or chelated copper and iron that can further increase oxidative stress through Fenton reactions 37. Reactive species reported as components of tobacco smoke include H2O2, O2•-, •OH, ONOO-, •NO2, ROO•, •NO, acrolein, crotonaldehyde, nitrosamines, among others. Acrolein and crotonaldehyde have been reported as the main triggers in the oxidation of protein thiols in the oral cavity, causing structural and functional modifications 31. Smoking can interfere with the antioxidant systems of periodontal tissues, inhibiting the bacterial plaque defenses, causing vasoconstriction, and slowing down wound healing as well as covering characteristic signs of
periodontitis, such as gingival bleeding 5.
Oxidative stress impact on saliva and periodontitis implications
Periodontitis is defined as a chronic and multifactorial immunoinflammatory disease associated with dysbiosis of the bacterial film (microbiome). It is influenced by the inflammatory response of the host, contained in the gingival crevicular fluid and saliva. In addition, it can be affected by environmental and behavioral factors, and its development can be modified by local factors (e.g., smoking), acquired conditions (systemic diseases), and genetic factors 6,38. The group of microorganisms present in the oral cavity is known as the oral microbiome or oral biofilm. For the development of periodontitis, a dysbiosis in the microbiome is necessary (changes in the composition of the microflora from a healthy state to an unhealthy one), these changes can be influenced by factors such as lack of hygiene, nutrition, exposure to physical agents - chemicals (variations in pH, temperature, tobacco, among others) 39-40. The persistence of a dysbiotic biofilm in periodontal pockets, triggers leukocyte migration (polymorphonuclear neutrophils—PMN—represent between 50% and 70% of the total leukocyte infiltrate) from the bloodstream to the infection site, where they play an essential role in periodontal health and the innate immune system as first barrier cells, acting through several unique defense mechanisms, including degranulation, chemotaxis, phagocytosis, NETosis (neutrophil extracellular traps), and release of ROS 41. Several studies show that the “hyperactive” PMN phenotype characterized by ROS overproduction is linked to periodontitis, making the subset of patients with higher levels of this neutrophil phenotype more susceptible to developing the disease 42. ROS play a significant role in cell signaling, gene regulation, and antimicrobial defense but an overproduction of ROS leads to an increased oxidative burden and an altered or reduced antioxidant capacity. This scenario leads to cellular oxidative stress within the affected tissues, which then causes pathological changes and consequently, destruction of host tissues and loss of dental support tissues 43. Periodontitis, like other chronic inflammatory diseases, is linked to an imbalance of redox homeostasis 44, which has been linked to the etiology and pathogenesis of the disease 11. In addition to an overproduction of ROS, the action of these reactive species is exacerbated in periodontitis due to a weakened antioxidant defense system 30. This breakdown of the antioxidant barrier is directly responsible for the oxidative and nitro-oxidative modifications occurring on oral cavity biomolecules because of the reduction of the neutralization capacity 45. Several studies have shown that oxidative stress is primarily responsible for the degradation of extracellular matrix components of periodontal tissue, including collagen, elastin, proteoglycans, and glycosaminoglycans (e.g., hyaluronic acid), which causes the loss of periodontal integrity 44. But it can also have indirect deleterious effects by generating oxidized fatty acids, which activate adipogenesis, inhibiting osteoblastogenesis by directly impacting osteoclasts 4. Lipid peroxidation markers are the most used to assess oxidative damage associated with periodontal diseases (i.e., malondialdehyde, 4-hydroxynonenal, 8-oxoguanine), because polyunsaturated fatty acids are highly susceptible to ROS attack 46. Considering that oxidative stress plays a major role in the pathogenesis of periodontitis, it has been suggested that supplementation with antioxidants could reduce or delay periodontal damage 47.
Redox pharmacology applied to periodontal disease
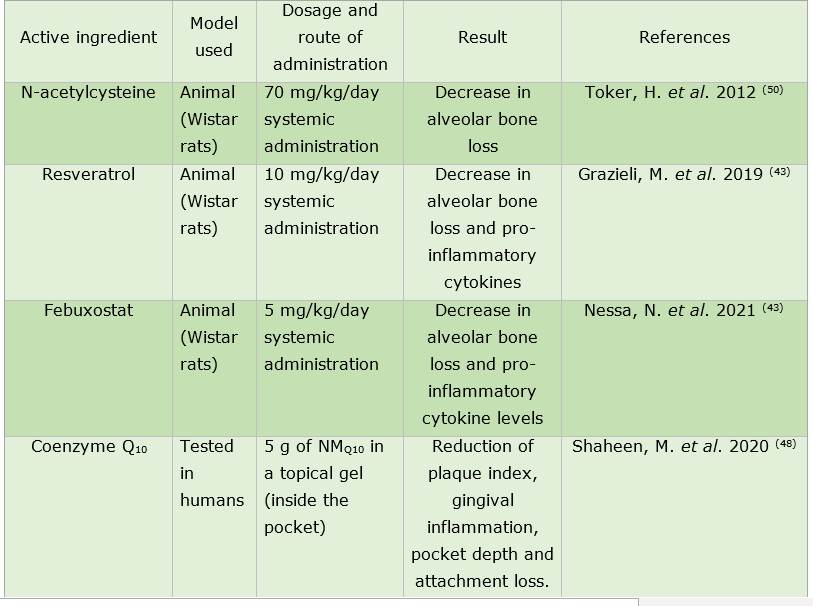
We now see specific interventions using redox medicine, i.e., compounds that can be administered to patients to attenuate the harmful effects of oxidative stress at the local level, based on the evidence of the major role of oxidative stress in periodontitis 48. Table 1 shows the most relevant compounds based on the relevant literature. There are ongoing trials on drugs such as resveratrol, a natural stilbenoid present in different foods which has been shown to be effective in reducing the rate of bone loss in animal models of periodontitis exposed to tobacco smoke when administered systemically as nutraceutical formulations 43. On the other hand, there is evidence that febuxostat, a xanthine oxidase inhibitor, could also be another potential agent for the treatment of periodontitis. As mentioned above, uric acid, an enzyme product of xanthine oxidase, is one of the main low molecular weight antioxidants in saliva. Paradoxically, despite the inhibition of this enzyme and, consequently, the decrease in uric acid production, febuxostat has been shown to be capable of slowing down bone loss and reducing the levels of proinflammatory cytokines and biomarkers of oxidative damage (i.e., HNE) 44. In contrast, most conventional antioxidants have drawbacks such as low water solubility, stability, and short duration of action when applied topically 48. On the other hand, redox pharmacology is also being tested in the production of nanomaterials (drug-loaded nanoparticles) and has the advantage that the component is released specifically at the therapeutic site (topical application), with high biocompatibility and low toxicity 49. Although the use of antioxidant-loaded nanoparticles is in the early stages of development, the few reported examples, including those loaded with coenzyme Q10, showed great potential for the treatment of periodontitis 48.
Discussion
As a result of technological progress in analytical methods and the accumulation of knowledge about the biological role of the different components of saliva, we have expanded our understanding of the association between salivary composition and the maintenance of oral health. The antioxidant components of saliva provide the first defense barrier (due to the presence of low molecular weight compounds and proteins) against ROS and ERN that arrive or are formed in the oral mucosa.
These oxidants cause an imbalance in cellular redox homeostasis that can determine a pathological scenario. Specifically, because of the combustion of tobacco, a wide variety of free radicals are transported that induce oxidative stress in the oral cavity. In fact, smoking is a major risk factor for periodontitis, a disease that is aggravated by the host's inflammatory response and changes in microbial populations, along with several factors mentioned in the text. ROS play a very important role in periodontal disease and lead to a scenario where endogenous antioxidant defenses fail due to overproduction of oxidants. This leads to further damage to nearby tissues and progression of the disease, which is why not only the molecular mechanisms involved are being explored more and more, but the use of redox pharmacology for its treatment is also being evaluated. Despite the need for more randomized clinical trials to examine the impact of redox-active pharmacological agents, recent results suggest that this strategy could prevent the progression of periodontal disease.
Conclusions
Knowledge of salivary antioxidant systems is of great importance to understand the development of many local and systemic diseases associated with oral health.
Periodontitis, which has been extensively studied in redox terms, could be attenuated using exogenous antioxidants. In this sense, the evidence analyzed here paves the way for the application of redox pharmacology (Fig. 4) as an adjuvant therapy to traditional techniques in the treatment of periodontitis and shows how valuable is to study the underlying molecular mechanisms in order to make more effective and accurate decisions.
Acknowledgments
We are grateful to Professor Dr. Rafael Radi from Facultad de Medicina, for his contributions to implement this research field on our group in Facultad de Odontología
REFERENCES
1. Maciejczyk M, Zalewska A, Ladny JR. Salivary Antioxidant Barrier, Redox Status, and Oxidative Damage to Proteins and Lipids in Healthy Children, Adults, and the Elderly. Oxid Med Cell Longev (Internet). 2019;2019(Salivary Redox Homeostasis and Oxidative Stress):12. Available from: https://doi.org/10.1155/2019/4393460 [ Links ]
2. Edgar M, Dawes C, O'Mullane D. Saliva and Oral Health (Internet). 4ta ed. Stephen Hancocks Limited; 2012. Available from: https://wrigleyoralhealth.com/content/docs/SHL_S_OH_A5_2015_FINAL.pdf [ Links ]
3. Knas M, Maciejczyk D, Zalewska A. Oxidative stress and salivary antioxidants. Dent Med Probl. 2013;50(4):5 [ Links ]
4. Zukowski P, Maciejczyk M, Waszkiel D. Sources of free radicals and oxidative stress in the oral cavity. Arch Oral Biol. 2018;92:8-17. [ Links ]
5. Huang Chang C, Lun Han M, Teng NC, Yu Lee C, Ting Huang W, Tong Lin C, Kai Huang Y. Cigarette Smoking Aggravates the Activity of Periodontal Disease by Disrupting Redox Homeostasis- An Observational Study. Sci Rep. 2018;8(11055). [ Links ]
6. Toczewska J; Konopka T, Zalewska A, Maciejczyk M. Nitrosative Stress Biomarkers in the Non Stimulated and Stimulated Saliva, as well as Gingival Crevicular Fluid of Patients with Periodontitis: Review. Antioxidants (Basel, Switzerland). 2020;9(3):14. [ Links ]
7. Dahiya P, Kamal R, Gupta R, Bhardwaj R, Chaudhary K, Kaur S. Reactive oxygen species in periodontitis. J Indian Soc Periodontol. 2013;17(4):411-6. [ Links ]
8. Sies H. Oxidative Stress: Introductory Remarks, in Oxidative Stress. 1era ed. Sies H, editor. Academic Press; 1985. 1-8 p. [ Links ]
9. Sies H, Berndt C, Jones D. Oxidative stress. Annu Rev Biochem. 2017:715-48. [ Links ]
10. Radi R. Evolución del concepto de "Estrés Oxidativo": medio siglo de aportes de la Facultad de Medicina, Montevideo, Uruguay. Anales de Facultad de Medicina (Internet). 2014: 9-22. Available from: https://revistas.udelar.edu.uy/OJS/index.php/anfamed/article/view/225/216 [ Links ]
11. Iannitti T Rottigni V, Palmieri B. Role of free radicals and antioxidant defences in oral cavity-related pathologies. J Oral Pathol Med. 2012;41(9):649-61. [ Links ]
12. Sies H. Oxidative eustress: On constant alert for redox homeostasis. Redox Biol. 2021;41(101867):8. [ Links ]
13. Sies H, Jones D. Reactive oxygen species (ROS) as pleiotropic physiological signalling agents. Nat Rev Mol Cell Biol. 2020;21(7):363-83. [ Links ]
14. Radi R. Oxygen radicals, nitric oxide, and peroxynitrite: Redox pathways in molecular medicine. Proc Natl Acad Sci U S A . 2018;115(23):5839-48. [ Links ]
15. Halliwell B. Reactive Species and Antioxidants. Redox Biology Is a Fundamental Theme of Aerobic Life. Am Soc Plant Biol. 2006;141:312-22. [ Links ]
16. Battino M, Ferreiro MS, Gallardo I, Newman HN, Bullon P. The antioxidant capacity of saliva. J Clin Periodontol 2002 Mar;29(3):189-94 [ Links ]
17. Valez V. Producción de radicales libres en sistemas biológicos y su detección mediante quimioluminiscencia. Tesis de grado. Montevideo: Universidad de la República, 2006. [ Links ]
18. D'Autréaux B, Toledano MB. ROS as signalling molecules: mechanisms that generate specificity in ROS homeostasis. Nat Rev Mol cell Biol. 2008;8:813-824. [ Links ]
19. Augusto O, Miyamoto S. Radicals and related species. In: Pantopoulus K, Schipper H, editor. Principles of free radical biomedicine. New York: Nova biomedical; 2012 [ Links ]
20. Poderoso JJ. El Premio Nobel 1998: la resurrección de un gas inorgánico como una molécula de alta significación biológica. Med UBA (Internet). 1999; 59: 205-7. Available from: http://www.medicinabuenosaires.com/revistas/vol59-99/2/v59_n2_205_207.pdf [ Links ]
21. Ignarro LJ. Biosynthesis and Metabolism of Endothelium-Derived Nitric Oxide. Annu Rev. 1990;50:535-60. [ Links ]
22. Denicola A, Souza J, Radi R. Diffusion of peroxynitrite across erythrocyte membranes. Proc Natl Acad Sci USA. 1998;95:3566-357. [ Links ]
23. Radi R, Peluffo G, Alvarez MN, Naviliat M, Cayota A.Unraveling peroxynitrite formation in biological systems. Free Radic Biol Med. 2001;30(5):463-88. [ Links ]
24. Trujillo M, Ferrer-Sueta G, Radi R. Peroxynitrite detoxification and its biologic implications. Antioxid Redox Signal. 2008;9:1607-20. [ Links ]
25. Waszkiewicz N, Bejda G, Zalewska A, Maciejczyk M. Diagnostic Value of Salivary Markers in Neuropsychiatric Disorders. Dis Markers (Internet). 2019;6. Available from: https://doi.org/10.1155/2019/4360612 [ Links ]
26. Akalin FA, Baltacioglu E, Alver A, Karabulut E. Lipid peroxidation levels and total oxidant status in serum, saliva and gingival crevicular fluid in patients with chronic periodontitis. J Clin Periodontol. 2007;34:558-65. [ Links ]
27. Halliwell B, Gutteridge JMC. Free radicals in biology and medicine. 4ta ed. New York: Oxford University Press Inc.; 2010. 79-178 p. [ Links ]
28. Fridovich I. Superoxide dismutases. An adaptation to a paramagnetic gas. J Biol Chem. 1989;264(14):7761-4. [ Links ]
29. Narendra S, Das UK, Tripathy SK, Sahani NC. Superoxide Dismutase, Uric Acid, Total Antioxidant Status, and Lipid Peroxidation Assay in Chronic and Aggressive Periodontitis Patients. J Contemp Dent Pr. 2018;19(7):874-80. [ Links ]
30. Sardaro N, Della Vella F, Incalza MG, Di Stasio D, Lucchese A, Contaldo M, Laudadio C, Petruzzi M. Oxidative Stress and Oral Mucosal Diseases: An Overview. In Vivo (Brooklyn). 2019;33(2):289-96. [ Links ]
31. Permuy M, López-Peña M, González-Cantalapiedra A, Muñoz F. Melatonin: A Review of Its Potential Functions and Effects on Dental Diseases. Int J Mol Sci. 2017;18(865):13. [ Links ]
32. Meenakshi S, Malaiappan S. Role of melatonin in periodontal disease - A systematic review. Indian J Dent Res. 2020;31(4):593-600. [ Links ]
33. Ghallab N, Hamdy E, Shaker O. Malondialdehyde, superoxide dismutase and melatonin levels in GCF of aggressive and chronic periodontitis patients. Aust Dent J. 2016;61(1):53-61. [ Links ]
34. Neslihan Avan A, Demirci Çekiç S, Uzunboy C, Apak R. Spectrophotometric Determination of Phenolic Antioxidants in the Presence of Thiols and Proteins. Int J Mol Sci. 2016;17(1325):16. [ Links ]
35. do Valle I, Roweth H , Malloy M, Moco S, Barron D, Battinelli E, Loscalzo J Barabási A-L. Network Medicine Framework Shows Proximity of Polyphenol Targets and Disease Proteins is Predictive of the Therapeutic Effects of Polyphenols. BioRxiv (pre-print). 2020.08.27.270173. https://doi.org/10.1101/2020.08.27.270173 [ Links ]
36. Javed F, Rahman I, Romanos G. Tobacco-product usage as a risk factor for dental implants. Periodontol 2000. 2019;81(1):48-56. [ Links ]
37. Gutierrez Maydata A. Oxidantes en el humo del cigarro y enfermedades cardiopulmonares. Rev Cuba med (Internet). 2003;42(5). Available from: http://scielo.sld.cu/scielo.php?script=sci_arttext&pid=S0034-75232003000500009&lng=es [ Links ]
38. van der Velden U, Abbas F Armand, S Loos BG, Timmerman MF, Van der Weijden GA, Van Winkelhoff AJ ,Winkel EG. Java project on periodontal diseases. The natural development of periodontitis: risk factors, risk predictors and risk determinants. J Clin Periodonto. 2006;33(8):540-8. [ Links ]
39. Ali Mosaddad S, Tahmasebi E, Yazdanian A, Bagher Rezvani M, Seifalian A, Yazdanian M, Tebyanian H. Oral microbial biofilms: an update. Eur J Clin Microbiol Infect Dis. 2019;38(11):2005-19. [ Links ]
40. De Luca F, Shoenfeld Y. The microbiome in autoimmune diseases. Clin Exp Immunol. 2019;195(1):74-85. [ Links ]
41. Landzberg M, Doering H, Aboodi GM, Tenenbaum HC, Glogauer M. Quantifying oral inflammatory load: oral neutrophil counts in periodontal health and disease. J Periodontal Res. 2015;50(3):330-6 [ Links ]
42. Chapple IL, Brock GR, Milward MR, Ling N, Matthews JB. Compromised GCF total antioxidant capacity in periodontitis: cause or effect? J Clin Periodonto. 2017;34(2):103-10. [ Links ]
43. Grazieli Correa M, Absy S, Tenenbaum, H, Vieira Ribeiro F, Ribeiro Cirano F, Casati MZ, Perez Pimentel S. Resveratrol attenuates oxidative stress during experimental periodontitis in rats exposed to cigarette smoke inhalation. J Periodontol Res 2019;54(3):225-232 [ Links ]
44. Nessa N, Kobara M, Toba H, Adachi T, Yamamoto T, Kanamura N, Pezzotti G, Nakata T. Febuxostat Attenuates the Progression of Periodontitis in Rats. 2021; 106 (5-6): 294-304. [ Links ]
45. Tóthová, L, Kamodyová N, Cervenka T, Celec P. Salivary markers of oxidative stress in oral diseases. Front Cell Infect Microbiol. 2015;5(73) [ Links ]
46. Poprack P, Jomova K, Simunkova M, Kollar V, Rhodes C, Valko M. Targeting free radicals in oxidative stress- related human diseases. Trends Pharmacol Sci. 2017;38(7):592-607. [ Links ]
47. Ambati M, Rekha Ran K, Veerendranath Reddy P, Suryaprasanna J, Dasari R, Gireddy H. Evaluation of oxidative stress in chronic periodontitis patients following systemic antioxidant supplementation: A clinical and biochemical study. J Nat Sci Biol Med. 2017;8(1):99-103. [ Links ]
48. Shaheen M, Elmeadawy S, Bazeed F, Anees M, Saleh N. Innovative coenzyme Q 10-loaded nanoformulation as an adjunct approach for the management of moderate periodontitis: preparation, evaluation, and clinical study. 2020;8:548-564. [ Links ]
49. Sui L, Wang J, Xiao Z, Yang Y, Yang Z, Ai K. ROS-Scavenging Nanomaterials to Treat Periodontitis. Front Chem. 2020;8(595530):6. [ Links ]
Conflict of interest declaration: The authors have no conflict of interest regarding the publication of this paper.
Source of funding: VS received funding from the Espacio Interdisciplinario and VV from the research consolidation program of Facultad de Odontología.
Authorship contribution: 1. Conception and design of study 2. Acquisition of data 3. Data analysis 4. Discussion of results 5. Drafting of the manuscript 6. Approval of the final version of the manuscript. VS has contributed in 2, 3, 4, and 5. AA has contributed in 1, 4, and 6. VV has contributed in 1, 2, 3, 4, and 6.
Received: July 20, 2021; Accepted: August 31, 2021
 Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
