










Servicios Personalizados
Revista

Articulo
 texto en
texto en  Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
Links relacionados
Compartir

 Permalink
PermalinkOdontoestomatología
versión impresa ISSN 0797-0374versión On-line ISSN 1688-9339
Odontoestomatología vol.24 no.39 Montevideo jun. 2022 Epub 01-Ago-2022
https://doi.org/10.22592/ode2022n39e219
Research
Tooth eruption and caries activity: is it a risk factor in adolescents?
1
 http://orcid.org/0000-0003-2273-4470
http://orcid.org/0000-0003-2273-4470
1
http://orcid.org/0000-0002-2940-4039
1Facultad de Odontología, Universidad de la República, Uruguay
2Cátedra de Odontopediatría, Facultad de Odontología, Universidad de la República, Uruguay. dra.alvarezloureiro@gmail.com
Objective:
to describe the behavior, distribution, and severity of lesions on the occlusal surfaces of the second permanent molars. Relate it to its stage of eruption and presence of activity in the rest of oral cavity.
Methodology:
A descriptive study was conducted in a convenience sample of 100 adolescents of both sexes (mean age = 13.39 ± 0.94 years). The parents answered a questionnaire on socioeconomic characteristics and general health, and the adolescents, one on food and hygiene habits. Two calibrated examiners recorder caries according to ICDAS II on all the dental surfaces . They also mapped the occlusal surface and eruption stage of the second permanent molars.
Results:
the prevalence of caries was 97%, and the extension (modified DMFT) was 8.45 ± 5.10. Eighty-two percent of the adolescents with caries experience had active lesions, and 62% of those with caries had lesions only on the occlusal surfaces of the second permanent molars. A higher prevalence of active caries lesions was observed in eruption stages I and II of the second permanent molars. The most affected sites were the central and mesial fossa and the central and distal fossa.
Conclusions:
Active molar eruption entails a risk stage that should be considered when prioritizing and developing oral health programs.
Keywords: occlusal caries; caries activity; eruption; second permanent molar
Objetivo:
describir el comportamiento, distribución y severidad de las lesiones de caries en las superficies oclusales de los segundos molares permanentes. Relacionarlo a su etapa de erupción y presencia de actividad en el resto de la cavidad bucal.
Metodología:
Se realizó un estudio descriptivo en una muestra de conveniencia de 100 adolescentes, de ambos sexos, (edad promedio=13,39±0,94 años). Los padres respondieron un cuestionario sobre aspectos socioeconómicos y salud general y los adolescentes sobre dieta y hábitos de higiene. Dos examinadoras calibradas realizaron el examen clínico de acuerdo a los criterios de ICDAS II en todas las superficies erupcionadas, así como el mapeo de la cara oclusal y la etapa de erupción de los segundos molares permanentes.
Resultados:
la prevalencia de caries fue de un 97% y la extensión (CPOD modificado) de 8,45± 5,10. El 82% de los adolescentes con experiencia de caries presentaba lesiones activas y el 62% de los carioactivos presentaban lesiones únicamente en las caras oclusales de los segundos molares permanentes. Se observó mayor prevalencia de lesiones de caries activas en los estadíos I y II de erupción de los segundos molares permanentes, siendo los sitios más afectados la fosa central y mesial y la fosa central y distal, respectivamente.
Conclusiones:
La erupción activa de molares significa una etapa de riesgo para las personas que debe ser considerada al momento priorizar y establecer programas de salud bucal.
Palabras clave: caries oclusales; actividad de caries; erupción dentaria; segundos molares permanentes
Objetivo:
descrever o comportamento, distribuição e severiidade das lesões de cárie nas superfícies oclusais dos segundos molares permanentes. Relacionar com seu estágio de erupção e presença de atividade no resto da cavidade oral.
Metodologia:
Foi realizado um estudo descritivo em uma amostra de conveniência de 100 adolescentes, de ambos os sexos, (média de idade = 13,39 ± 0,94 anos). Os pais responderam a um questionário sobre aspectos socioeconômicos e de saúde geral e os adolescentes sobre alimentação e hábitos de higiene. Dois examinadores calibrados realizaram o exame clínico de acordo com os critérios do ICDAS II em todas as superfícies erupcionadas, além de mapear a superfície oclusal e o estágio de erupção dos segundos molares permanentes.
Resultados:
a prevalência de cárie foi de 97% e a extensão (CPOD modificado) de 8,45 ± 5,10. 82% dos adolescentes com experiência de cárie tinham lesões ativas e 62% dos carioativos tinham lesões apenas nas superfícies oclusais dos segundos molares permanentes. Maior prevalência de lesões de cárie ativas foi observada nos estágios I e II de erupção dos segundos molares permanentes, sendo os locais mais acometidos a fossa central e mesial e a fossa central e distal, respectivamente.
Conclusões:
A erupção ativa de molares representa uma etapa de risco para as pessoas que deve ser considerada na priorização e estabelecimento de programas de saúde bucal.
Palavras-chave: cárie oclusal; atividade de cárie; erupção dentária; segundos molares permanentes
Introduction
Dental caries is a multifactorial, noncommunicable, and socially modulated disease.1 It is among the ten most prevalent noncommunicable diseases worldwide.2,3 However, a decrease in its prevalence has been observed in different populations and age groups since the mid-1970s.4,5 Uruguay has experienced the same trend in the population aged 12, with a 34.75% decline in the prevalence of dental caries found when comparing the 1999 and 2010 epidemiological studies.6
In addition to the decline in prevalence, the severity of carious lesions has decreased.7-9 This phenomenon is attributed to the increased bioavailability of fluorides in the oral environment 3,4,10 associated with the widespread use of toothpaste. Fluoride in the oral environment helps slow down the progression of lesions, with long periods of time observed between the detection of the initial lesion (IL), the active non-cavitated lesion (ANCL), and the cavitation. In low-prevalence populations, ANCLs can be the only clinical manifestation of the disease (20% of the population),11,12 giving rise to the need for specific and more sensitive diagnostic criteria.
The decreasing prevalence and the slowing down of lesion progression simultaneously change the distribution pattern of the lesions. The occlusal surfaces of permanent molars are the sites most susceptible to caries in children and adolescents.13 In 1989, Carvalho et al. showed the relationship between the eruption period of the first molars, their functional stage, as well as the specific dental anatomy, the presence/amount of dental biofilm, and caries activity in a population with low prevalence.12,13 The period of active eruption of molars (from their emergence into the oral cavity until they have made contact with the antagonist molar) stands out as a time of high risk for developing carious lesions. Therefore, the period of life that includes the active eruption of permanent molars is considered a “risk age” for developing carious lesions12-14. Some researchers have recently included it as a specific risk factor in children/adolescents.15)
Early detection of carious lesions, particularly in these risk periods, is a great challenge for clinical dentistry since it helps control the progression of the disease, delaying the need for invasive treatments, thus preventing patients from entering into a continuous restorative cycle.11,13,14
This study aims to describe the carious lesions on the occlusal surfaces of the second permanent molars and their eruption stage in a population of adolescents in Montevideo. To describe their severity and distribution concerning the dental anatomy and correlate the findings and the presence or absence of caries activity in the rest of the oral cavity.
Materials and method
This cross-sectional, descriptive study results from a convenience subsample (n = 100) from the Project “Oral health care program based on the control of caries and periodontal diseases in adolescents: a controlled clinical trial” (No. 091900-000016-16) of the School of Dentistry, UdelaR, conducted in a socioeconomically disadvantaged community. This project included adolescents from the first and second years of basic secondary school aged between 12 and 14.
Data collection
Data were obtained from two structured questionnaires and the clinical examination. Parents and/or legal representatives provided the data on general health, socioeconomic status, sociodemographic characteristics, and access to health services. The adolescents completed a questionnaire to learn about oral health habits and behaviors. Adolescents taking chronic medication that might reduce salivary flow and those who were unable to perform oral hygiene independently or did not respond to the inquiry in the first three calls were excluded from the study.
The clinical examination was performed at the school attended by the adolescents by two trained and calibrated examiners (LA, AF). The procedure was conducted on exam tables, with the adolescent laying supine, using artificial light, a mirror, and a CPI periodontal probe, following the necessary biosafety guidelines to avoid cross-infection. Intra-examiner Kappa values were 0.78 for AF and 0.89 for LA. The inter-examiner value was 0.79.
Data from the clinical examination were recorded in a systematized manner:
1) Visible Plaque Index (VPI) recorded for all teeth present;
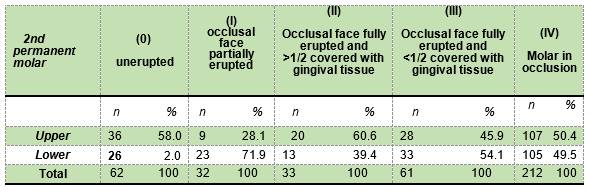
2) stage of eruption of the second molars recorded according to the criteria in Carvalho J.C., Ekstrand K.R., and Thylstrup A., 1989 (unerupted molar = 0; the occlusal surface partially erupted = I; the occlusal surface fully erupted, but more than half of the facial surface was covered with gingival tissue = II; the occlusal surface was erupted, and less than half the facial surface was covered with gingival tissue = III; eruption complete = IV, molar in full occlusion);
3) Biofilm was recorder on the occlusal surface of the second molars mapped according to the anatomical sites of the same author (no visible plaque “0”, hardly detectable plaque, restricted to grooves and fossae “1”, plaque easily noticeable in grooves and fossae “2”, and occlusal surface partially or totally covered with plaque “3”;14
4) Gingival Bleeding Index (GSI) was recorded for all teeth.16 Biofilm was removed mechanically with a toothbrush from all tooth surfaces for the clinical visual-tactile diagnosis of carious lesions. The surface was dried using cotton gauze and illuminated with artificial LED light.
The ICDAS II (International Caries Detection and Assessment System) criteria18 were used to describe the severity of the lesions as follows: sound surface (ICDAS “0”), non-cavitated lesion (ICDAS “1”+“2”), cavity in enamel (ICDAS “3”), shadow lesion (ICDAS “4”), and cavity in dentin, CL, (ICDAS “5”+“6”). The lesions were then classified based on this diagnosis as initial (non-cavitated lesion): IL, moderate (cavitated lesion in enamel + shadow lesion): ML, and severe (cavity in dentin): SL.
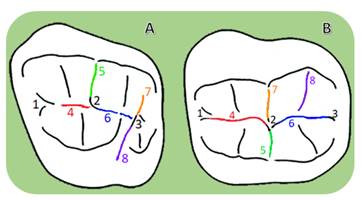
We recorded the carious lesions in each anatomical site of the occlusal surface of the upper and lower second molars in detail and mapped them in the first permanent molars adapting the criteria used by Carvalho et al. 1989 (Figure 1).14
Lesion activity was classified according to clinical features such as surface roughness and light reflection, following the criteria in Nyvad et al.18 Filled and missing surfaces were recorded.
Data analysis
The data were entered into conditional electronic spreadsheets (LibreOffice software), and the data were kept confidential. Descriptive analyses of all variables were performed. The prevalence of caries was defined as the percentage of individuals who had at least one cavitated or non-cavitated carious lesion, regardless of the diagnosis of activity. The extent of the disease was calculated based on the modified DMFT index according to the described criteria (sum of decayed, cavitated or non-cavitated, missing, and filled teeth). Stratified bar charts were used to describe the lesions in the upper and lower second molars by site and degree of eruption.
All analyses were performed using R Core Team 2012 software.
Ethical considerations: The study followed the guidelines issued by the MERCOSUR Medical Ethics Committee, and it was approved by the Ethics Committee of the School of Dentistry under number 091900-000016-16. All participants and/or their legal guardians signed the assent and informed consent.
The adolescents involved were instructed on oral hygiene and received a hygiene kit (toothbrush, dental floss, and fluoride toothpaste). They were also given a written report on their oral health and were treated at the school.
Results
The adolescents examined were in the first and second grades of secondary education (51 and 49 students, respectively). The average age was 13.39 ± 0.94 years, and 51 of them were female. Almost all the adolescents examined (n = 97) had at least one carious lesion (cavitated or non-cavitated), regardless of activity. Of those, 82 adolescents had at least one active caries lesion, and among them, 62% (n = 51) only had active lesions on the occlusal surfaces of the second permanent molars. No differences were found by sex. Additionally, only 41 adolescents had at least one cavitated carious lesion.
The mean modified DMFT (sum of the number of teeth with cavitated or non-cavitated carious lesions, missing teeth, and filled teeth) was 8.45 ± 5.10. Considering only teeth with active carious lesions, the modified DMFT was 5.19 ± 4.51, and 1.76 ± 2.13 when counting only teeth with cavitated lesions.
Despite the average age of the sample studied, only 49 adolescents had their four second molars fully erupted (stage IV), 25 of whom were female. Seven adolescents had no erupted molars (four of whom were male).
Table 1 shows the eruption stages of permanent second molars in the population studied. Sixty-two second molars were unerupted, 36 in the upper jaw and 26 in the lower jaw (58% and 42%). Eruption stages I and II were found in approximately the same number of second molars (32 and 33, respectively). However, 72% of those in eruption stage I were lower molars, while 61% of those in eruption stage II were upper molars. Finally, 212 second molars, in equal proportion in the upper and lower jaw, were in eruption stage IV (Table 1).
A total of 337 occlusal surfaces were mapped, 164 for upper molars and 173 for lower molars. Figures 2 and 3 show the distribution of carious lesions (severity and activity) by occlusal surface planimetry in the different eruption stages of the upper and lower molars.
Figure 2: Distribution of carious lesions in the upper second permanent molars (n = 164), by eruption stage, in the eight sites detailed by Carvalho et al. in the occlusal surface planimetry.
The central fossa is the anatomical site most affected by caries when the molar is in stage I of eruption (molar with the occlusal face partially erupted), (site 2), followed by the mesial fossa (site 1) and the groove extending from the central fossa towards the facial surface (site 5). The carious lesions observed were exclusively active initial lesions (AIL) (Figure 2). The lesions diagnosed in eruption stage II continued to be mostly AILs and were predominantly located in site 2, followed by sites 5, 3, and 1.
In eruption stage III, however, the number of AILs decreased, and the sound surfaces and inactive initial lesions (IIL) increased. When full occlusion was reached in stage IV, the number of sound sites and IILs continued to be widely prevalent, and sealants and restorations were observed. Active ML and SL were observed to a lesser extent in sites 2, 3, 7, and 8.
Figure 3: Distribution of carious lesions in the lower second permanent molars (n = 173), by eruption stage, concerning the eight sites detailed by Carvalho et al. in the occlusal surface planimetry.
Figure 3 shows the distribution of AILs in the different sites of the occlusal surface of lower molars. The behavior of the lesions was similar to that observed in the upper molars in stages I and II. Although in stage III most of the sites were diagnosed as healthy or with IILs, sealants and restorations were observed, unlike the upper sites.
Healthy sites and IILs prevailed in stage IV, and ML and/or SL were observed in all analyzed sites, unlike in the upper molars.
Discussion
A higher prevalence of active carious lesions was found in the population studied in eruption stages I and II of the second permanent molars, predominantly in the anatomical sites of the occlusal surface where more biofilm is accumulated. The most affected sites in stages I and II were the central and mesial fossa (sites 2, 1) and the central and distal fossa (sites 2, 3). An unexpected finding was that 62% of the adolescents with caries only had active carious lesions on the occlusal surface of the second molars. This showed that the prevalence of cavitated carious lesions is low for subjects in this age group, from a socioeconomically disadvantaged community, with access to fluoridated salt and toothpaste.
The period starting immediately after the onset of eruption and ending when full occlusion is achieved has been identified as a predictor of caries, mainly for permanent molars.19 It varies according to the molar studied: two or three years for the first and second permanent molars.19
In this study, 62% of the adolescents with caries had AILs on the occlusal surfaces of the second molars during active eruption as the only manifestation of dental caries. Therefore, two aspects must be considered: the systematization of the diagnosis of non-cavitated lesions (careful, methodologically detailed and validated diagnosis) and active eruption as a predictor of risk.20,21
Since the 1990s, different epidemiological studies have shown an increasing prevalence of ILs. Even in low-prevalence populations, these may be the only manifestation of the disease.22,23 ILs can be slowed down and even remineralized by controlling the sites of biofilm stagnation (non-operative treatment of dental caries),22 although they require a more sensitive diagnostic method, professional training, and more clinical time. The importance of diagnosing carious lesions early lies in the possibility of using a timely minimal intervention approach. The diagnosis requires removing the biofilm (clean surface), especially for this type of lesion, and adhering to a standardized examination process (dry and well-lit field). These basic diagnostic requirements are not always met in public health services, leading to an underdiagnosis of ILs. Among the adolescents examined, 75% reported visiting a dentist in the previous three months and stated that they had not been informed they had carious lesions.
Several studies have sought to find objective diagnostic criteria to determine the severity of carious lesions and the likelihood of progression: activity.17,24,25). In the early 2000s, a group of researchers developed a new system for classifying lesions (based on their severity) and addressing them: the International Caries Detection and Assessment System (ICDAS), with an objective and radiographically and histologically validated method.17 However, the severity diagnosis is insufficient to determine the need for treatment; it always needs to be accompanied by an activity diagnosis (current degree of mineral loss). The clinical parameters described in the literature by Nyvad et al. (1999) for diagnosing the lesion’s activity are shine, color, and texture, always relative to sites of biofilm accumulation on the lesion surface.18)
Determining the lesion’s activity is critical for therapeutic decision-making in dental caries, regardless of the severity of the lesion that requires a restorative decision.
According to the literature, half of the caries experience of young people is located on the occlusal surface, although it accounts for only 15% of the total tooth surface.25) The molars are the most affected teeth, followed by the premolars.26,27 The first molars are more severely affected than the second molars. As described in the paper by Carvalho et al. (1989), a relationship was found between occlusal functionality (eruption stage) and caries activity.14) As mentioned above, the most affected sites in stage I and II are the central fossa, followed by the mesial fossa in upper molars and the distal fossa in lower molars. These lesions persist to a lesser degree in stages III and IV. They correspond to the deepest sites of the molar anatomy. They are the areas that are first exposed to the oral environment and/or remain in infraocclusion the longest.
In addition, during stages III and IV, sites 5, 6, 7, and 8 are most affected. They are the anatomical area that remains the longest without contact with the antagonist. Second molars need up to 72 months to reach the occlusal plane, with the distal part of the occlusal surface remaining at the gingival level for longer.
The accumulation of sugar-rich biofilm is the key etiological factor for understanding the development of carious lesions. The anatomy of the occlusal surface and the long period of active eruption of the molars, which means their mechanical function remains reduced, favor the adhesion and stagnation of biofilm. This leads the biofilm to mature and causes a lesion underneath when dysbiosis occurs.14,28
As the molar erupts, the occlusal surface becomes more accessible to hygiene, and as it reaches occlusion, the masticatory function performs this action. As it is possible to manage biofilm more efficiently, AILs can slow down their progression or remineralize. This partly explains the appearance of IILs in stage III, reaching the highest percentage in stage IV in this study (Figure 3). Two studies have shown that the percentage of active lesions decreases as the occurrence of inactive lesions increases when the molar reaches occlusion.14,21 Therefore, the period of active eruption of molars needs to be considered a risk stage for patients and should be considered when implementing oral health programs. Managing carious lesions consists of controlling their progression through noninvasive treatments and reducing the number of individuals that undergo restorative treatment.12
REFERENCES
1. Lencova EBZ. Psychosocial, behavioural and oral health indicators: review of the literature. Prague Med Rep. 2006; 107(3): 305-316. [ Links ]
2. Frencken JE, Sharma P, Stenhouse L, Green D, Laverty D, Dietrich T. Global epidemiology of dental caries and severe periodontitis - a comprehensive review. J Clin Periodontol 2017; 44 (Suppl. 18): S94-S105. [ Links ]
3. Ayala CDL. Los pediatras en la prevención de enfermedades bucales. Arch. Pediatr. Urug. 2016 Set; 87(3):257-262. [ Links ]
4. Costa FCMD, Freitas Fernández HL, Freitas De Farias Moura E, Costa Aguiar YP, Gomez Dos Santos F, Leite Cavalcanti A. Oral health habits, prevalence of dental caries and dental erosion in adolescents. Rev Gaúch Odontol 2017 jul/set; 65 (3): 202-207. [ Links ]
5. Espinoza C, Romero Saavedra M, Giacaman Sarah R. Evolución de la prevalencia de caries y gingivitis en niños de 6 y 12 años de Peralillo, VI Región,entre el año 2000 y el 2010. Rev. Clin. Periodoncia Implantol. Rehabil. Oral 2011; 4(3); 102-105. [ Links ]
6. Angulo M, Bianco P, Cuitiño E, Silveira A. Relevamiento y análisis de caries dental, fluorosis y gingivitis en adolescentes escolarizados de 12 años de edad en la República Oriental del Uruguay. Montevideo, Uruguay. ; 2015. [ Links ]
7. Marthaler TM. Changes in dental caries 1953-2003. Caries Res 2004 May-June; 38(3):173-181. [ Links ]
8. Bernabé E, Sheiham A. Extent of differences in dental caries in permanent teeth between childhood and adulthood in 26 countries. Int Dent J. 2014; 24:241-245. [ Links ]
9. WHO. Country/Area Project Profile Database. WHO Collaborating Center for Education, Trainen and Research in Oral Health. Malmo University. Online, 2015 cited 2017 Noviembre. Available from: http://www.mah.se/capp. [ Links ]
10. Fabruccini A, Alves R, Alvarez L, Alvarez R, Susim C, Maltz M. Comparative effectiveness of water and salt community-based fluoridation methods in preventing dental caries among school-children. Community Dent Oral Epidemiol. 2016; 44(6): 577-585. [ Links ]
11. Baelum V, Heidemann J, Nyvad B. Dental caries paradigms in diagnosis and diangostic research. Eur J Oral Sci. 2006 August; 114(4): 263-277. [ Links ]
12. Carvalho JC, Dige I, Machiulskiene V, Qvist V, Bakhshandeh A, Fatturi-Parola C, et al. Occlusal Caries: Biological Approach for Its Diagnosis and Management. Caries Res. 2016 December; 50(6): 527-542. [ Links ]
13. Carvalho JC. Caries Process on Occlusal Surfaces: Evolving Evidence and Understanding. Caries Res. 2014 July; 48(4): 339-346. [ Links ]
14. Carvalho JC; Ekstrand K; Thylstrup A. Dental Plaque and Caries on Occlusal Surfaces of First Permanent Molars in Relation to Stage of Eruption. J Dent Res. 1989 May;68(5):773-779. [ Links ]
15. Martignon S; Pitts NB; Goffn G; Mazevet M; Douglas GVA; Newton JT; et al. Caries Care practice guide: consensus on evidence into practice. Br Dent J. 2019 Sep; 227(5): 353-362. [ Links ]
16. Ainamo J, Bay I. Problems and proposals for recording gingivitis and plaque. Int Dent J. 1975 Dec; 25(4): 229-235. [ Links ]
17. Ismail A, Sohn W, Tellez M, Amaya A, Sen A, Hasson H. The International Caries Detection and Assessment System (ICDAS): an integrated system for measuring dental caries. Community Dent Oral Epidemiol. 2007 May; 35: 170-178. [ Links ]
18. Nyvad B, Machiulskiene V, Baelum V. Reliability of a New Caries Diagnostic System Differentiating between Active and Inactive Caries Lesions. Caries Res. 1999;(33): 252-260. [ Links ]
19. Mejàre I, Axelsson S, Dahlén G, Espelid I, Norlund A, Tranæus S, et al. Caries risk assessment: a systematic review. Acta Odontol Scand 2014; 72:81-91. [ Links ]
20. Braga, M. M., Mendes, F. M., Ekstrand, K. R. Detection activity assessment and diagnosis of dental caries lesions. Dent Clin North Am 2010; 54(3), 479-493 [ Links ]
21. Zenkner L; Alves L; de Oliveira RS, Bica RH; Maltz M. Influence of eruption stage and biofilm accumulation on occlusal caries in permanent molars: a generalized estimating equations logistics approach. Caries Res 2013; 47: 177-182. [ Links ]
22. Ismail A. Clinical diagnosis of precavitated carious lesions. Community Dent Oral Epidemiol. 1997 Feb; 25(1): 13-23. [ Links ]
23. Amarante E, Raadal M, Espelid I. Impact of diagnostic criteria on the prevalence of dental caries in Norwegian children aged 5, 12 and 18 years. Community Dent Oral Epidemiol. 1998 april; 26(2): 87-94. [ Links ]
24. Holmen L, Thylstrup A, Artun J. Clinical and histological features observed during arrestment of active enamel carious lesions in vivo (Part. 1). Caries Res. 1987; 21: 546-554. [ Links ]
25. Norrisgaard PE, Qvist V, Ekstrand K. Prevalence, risk surfaces and inter-municipality variations in caries experience in Danish children and adolescents in 2012. Acta Odontologica Scandinavica 2016; 74 (4), 291-297. [ Links ]
26. Carvalho J, Van Nieuwenhuysen J, D¨Hoore W. The decline in dental caries among Belgian children between 1983 and 1998. Community Dent Oral Epidemiol. 2001; 29(1): 55-61. [ Links ]
27. Carvalho J, D¨Hoore W, Van Nieuwenhuysen J. Caries decline in the primary dentition of Belgian children over 15 years. Community Dent Oral Epidemiol 2004 August; 32(4): 277-282. [ Links ]
28. Fejerskov O , Bente N, Kidd E. Dental Caries: the disease and its Clinical Management. 3rd ed.: Willey-Blackwell; 2015. [ Links ]
Conflict of interest declaration: The authors have no conflict of interest regarding the publication of this paper.
Authorship contribution 1. Conception and design of study 2. Acquisition of data 3. Data analysis 4. Discussion of results 5. Drafting of the manuscript 6. Approval of the final version of the manuscript RAL has contributed in 2.3, 4, 5, and 6. YOR has participated in 2, 3, 4, 5, and 6 AF has participated in: 3, 4, 5, and 6. LAL has participated in: 1, 3, 4, 5, and 6.
Received: September 12, 2021; Accepted: March 15, 2022
 Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
