










Services on Demand
Journal

Article
 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Related links
Share

 Permalink
PermalinkOdontoestomatología
Print version ISSN 0797-0374On-line version ISSN 1688-9339
Odontoestomatología vol.23 no.38 Montevideo 2021 Epub Dec 01, 2021
https://doi.org/10.22592/ode2021n37e305
Update
Hyoid bone position, tongue position, and pharyngeal airway dimension according to skeletal malocclusion
1Universidad Nacional Mayor de San Marcos, Perú. miriam.espada@unmsm.edu.pe
This study reviewed the articles that evaluated hyoid bone position, tongue position, and pharyngeal airway dimension according to skeletal malocclusion cephalometrically to determine a connection between these structures.
Method:
Publications were identified in the following databases: PubMed, Virtual Health Library (VHL), Scielo, and Scopus. Keywords: hyoid bone, tongue, airway, malocclusion. The articles were screened by title, abstract and full text, written in English and Spanish.
Results:
We found 75 articles; 30 were discarded because they lacked a direct connection with the topic. Finally, 45 articles were selected. There is still no general consensus on the relationship between the position of the hyoid bone, the tongue, and the dimension of the upper airway according to skeletal malocclusion.
Keywords: hyoid bone; tongue; airway; malocclusion
Esta investigación se centró en revisar los artículos que evaluaron cefalométricamente la posición de hueso hioides, posición lingual y la dimensión de la vía aérea faríngea según maloclusión esquelética, a fin de determinar si existe una relación entre estas estructuras.
Método:
Se identificaron publicaciones en las bases de datos: PubMed, Biblioteca Virtual en Salud (BVS), Scielo y Scopus. Palabras clave: Hueso hioides, Lengua, Vía aérea, Maloclusión. Se realizó un cribado de los artículos por título, resumen y texto completo, escritos en los idiomas inglés y español.
Resultados:
Se encontraron 75 artículos; se eliminaron 30, por no tener una relación directa con el tema. Finalmente, se seleccionaron 45 artículos. Se concluye que aún no hay un consenso absoluto, sobre la relación existente entre: la posición del hueso hioides, la lengua y la dimensión de la vía aérea superior; según maloclusión esquelética.
Palabras clave: Hueso Hioides; Lengua; Vía Aérea y Maloclusión
Esta investigação centrou-se na revisão dos artigos que avaliaram cefalometricamente a posição do osso hióide, a posição linguística e a dimensão da via aérea faríngea de acordo com a maloclusão esquelética, a fim de determinar se existe uma relação entre estes estruturas.
Método:
As publicações foram identificadas nas seguintes bases de dados: PubMed, Biblioteca Virtual em Saúde (BVS), Scielo e Scopus. Palavras-chave: Osso hióide, Língua, Via aérea, Maloclusão. Os artigos foram analisados por título, resumo e texto completo, escritos em inglês e espanhol.
Resultados:
Foram encontrados 75 artigos, 30 foram eliminados porque não estavam directamente relacionados com o tema. Finalmente, foram seleccionados 45 artigos. Conclui-se que ainda não existe consenso absoluto sobre a relação entre: a posição do osso hióide, a língua e a dimensão da via aérea superior, de acordo com a maloclusão esquelética.
Palavras-chave: Osso Hioide; Língua; Via Aérea; e Maloclusão
Introduction
Diagnosis is essential in orthodontics to treat malocclusions comprehensively. Several techniques and diagnostic tools are available for this purpose, such as radiographs, study models, and photographs.
The hyoid bone plays a key role in chewing, phonation, and swallowing. It also helps keep the airways unobstructed due to the attachment of the infrahyoid (omohyoid) muscle to the shoulder girdle. In addition, this bone is closely related to the tongue, as the genioglossus and the geniohyoid muscle join them. In turn, the tongue holds a large space in the oral cavity and performs movements in various oral functions such as swallowing, phonation, and breathing.1 Therefore, the analysis of the hyoid bone and tongue positions would indicate the pharyngeal airway passage. The pharyngeal airway, also known as the nasopharyngeal space, is a complex and multifunctional structure regulating different body processes. It coordinates breathing, ventilation, gastric, and phonation functions.2
McNamara3 admits that there is controversy in the relationship between respiratory function, facial morphology, and occlusion, as he fully recognizes that environmental factors could alter respiratory function.
According to Moss,4 the concepts of functional matrix and bone growth appear in response to the functional behavior of an individual's craniofacial mass. In this sense, alterations in the airway and tongue posture can affect maxillofacial growth. However, there is still insufficient research to support airflow as a determinant of craniofacial growth and development. Decreased airway patency alters breathing and modifies normal craniofacial and dentofacial development. Therefore, a good diagnosis and early treatment can prevent, restore, or correct craniomaxillofacial growth.5
This work aimed to review the articles that evaluated the hyoid bone position, tongue position, and pharyngeal airway dimension according to skeletal malocclusion cephalometrically to determine a connection between these three structures in each skeletal malocclusion.
Review and method
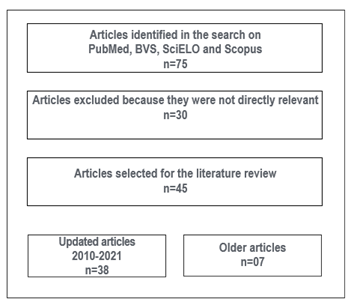
A literature search was conducted to review the articles relevant to this study. Medline, Lilacs, SciELO, and Scopus were used to search for these keywords: hyoid bone, tongue, airway, malocclusion. The articles selected included information on hyoid bone position, tongue position, and pharyngeal airway dimension in skeletal malocclusions. The data was extracted from cephalometric radiographs and CBCTs. The research papers chosen were written in English and Spanish between 2010 and 2021. Older articles were also included given the relevance of the information. The articles selected were screened, and then all the titles and abstracts were reviewed. A total of 75 articles were found, 30 of which were discarded because they were not directly relevant to the subject. Finally, 45 original articles were selected (Fig. 1).
a) Importance of studying the hyoid bone position, tongue position, and the pharyngeal airway
The analysis and evaluation of the hyoid bone position, tongue position, and pharyngeal airway in malocclusions have received significant attention in the literature due to the need for a complete diagnosis and an effective treatment plan. This suggests that the stomatognathic system should be evaluated comprehensively and not partially. Hyoid bone position plays an essential and active role in achieving postural balance and patency of the pharyngeal airway.6 The ability to accurately determine tongue position and volume is important for two reasons. First, evaluating hyoid bone position would also determine the state of patency of the pharyngeal airway. Second, this would make it possible to evaluate the influence of tongue size on the morphology of the face, dental arches, and oral function alterations (swallowing, phonation, and breathing). The pharyngeal airway dimensions are essential to evaluate obstructive sleep apnea (OSA) and to assess the possible orthognathic surgical procedures performed due to the risk of airway obstruction.8
In most of the articles studied, the researchers conducted a cephalometric analysis on lateral skull radiographs; in others, they used CBCT.
b) Relationship between hyoid bone position, tongue position, and pharyngeal airway dimension with skeletal malocclusion
Most of the articles relate these variables separately according to skeletal malocclusion hyoid bone position according to skeletal malocclusion,9-11 tongue position according to skeletal malocclusion,12-17 and pharyngeal airway dimension according to skeletal malocclusion15,18-26. Only a small number do so jointly hyoid bone position with pharyngeal airway dimension according to skeletal malocclusion5,7,28-31, hyoid bone position with tongue position according to skeletal malocclusion,32-36 tongue position with pharyngeal airway dimension according to skeletal malocclusion,15 and evidence of the relationship between hyoid bone, tongue position, and pharyngeal airway dimension according to skeletal malocclusion2,37-39
The articles analyzed mention that hyoid bone position differs in each type of malocclusion. The hyoid bone is positioned inferior and anterior in Class I9,11; more inferior and posterior in Class II;2,8,9,11,31-38,41 and more anterior11,30 and superior8,37,39 in Class III. Additionally, an inverse inclination of the hyoid bone (long axis of the hyoid bone not parallel to the mandibular plane) is observed in Class III patients.10 Other studies show a statistically significant difference in the hyoid bone's position and inclination toward the palatal plane and toward the basionnasion line in Class I and III patients.10
Regarding the resting tongue posture according to skeletal malocclusion, we found a more superior and posterior location,12,13,16,37,38 and a smaller volume37,39 in Class II; more inferior,12,14,38 anterior,15,17 and a larger volume37,39 in Class III.12-15,17 Tongue position was also found to be associated with the size of dentoalveolar maxillary and mandibular features.14
Regarding the dimension of the pharyngeal airway according to skeletal malocclusion, Class II patients have a smaller dimension,15,18,20-25,29-31,40 a more backward orientation, and a smaller volume8. Class III patients have a larger airway with a larger volume.6,15,18,21,24,30,31,40 These differences are statistically significant.20-23
Several articles correlate hyoid bone position and tongue position in relation to skeletal malocclusions. Patients with Class II skeletal malocclusion are associated with a more inferior and posterior hyoid bone position, a more superior, posterior tongue position, and a smaller volume. Class III patients have a more anterior and superior hyoid bone position and a more inferior, anterior, tongue position, and a larger volume.33-36,45 A correlation was also found between hyoid bone position and tongue position in people with vertical growth.32
Regarding the relationship between hyoid bone position and pharyngeal airway dimension in skeletal malocclusions, the articles mention that Class I malocclusions present a positive correlation between the lower airway and the horizontal distance from the hyoid bone to the retrognathion.28 Additionally, hyoid bone position is related to pharyngeal airway dimension.8,29 The airway dimension was significantly narrower and the location of the hyoid bone more posterior and inferior in Class II patients.31 It is also mentioned that the more protruding the mandible (SNB), the more anterior the hyoid bone and the larger the pharyngeal airway dimension.32
Evidence of the relationship between hyoid bone, tongue position, and pharyngeal airway dimension in malocclusions indicates that Class III patients have larger tongues.
Regarding Class II, it was found that the anatomical balance (volume proportionality) between the tongue and the oral cavity was greater.38 It was also found that upper oropharyngeal width was narrower and that the tongue dorsum was located more superiorly in hyperdivergent patients. Hypodivergent patients have the tongue and the hyoid bone in a more inferior and posterior position. Variations in upper and lower oropharyngeal width, tongue posture, and hyoid bone position were observed in all growth patterns.33,38
A strong correlation was found between CBCT measurements and lateral cephalograms.7,43-45
Discussion
Almost all the studies reviewed used the ANB angle to establish the anteroposterior relationships of the mandible. However, this has wellknown limitations and is influenced by many variables such as the morphology of the nasion area, the facial vertical dimensions, the inclination of the anterior cranial base, and the inclination of the jaws. If only the ANB angle is used to measure the position of the maxilla and mandible relative to each other, the location of points A and B in the vertical plane will influence the size of the angle and not the actual sagittal relationship of the jaws. However, the ANB angle is still recognized as a traditional way of determining anteroposterior malocclusions and was also accepted in this work.
This review found that hyoid bone position varies in different malocclusions according to the relationship between each structure and skeletal malocclusion8,9,11,31-38,40. However, Nejaim et al.6 found that hyoid bone position according to its anteroposterior, vertical, and angular dimensions did not present statistically significant differences among the three types of skeletal malocclusions. Furthermore, José et al.28 evaluated only hyoid bone position in the anteroposterior dimension and found no statistically significant differences between the three skeletal malocclusions. We believe that these differing results are due to the application of different cephalometric analysis methodologies and variations in sample characteristics.
The tongue resting posture was found to be different according to skeletal malocclusion.2,12-17,38 However, Fatima et al.12 found no significant differences between tongue posture and skeletal malocclusions. Although no statistically significant difference was found, the results suggest the potential existence of moderate to large variations in sagittal skeletal relationship with different tongue postures. Therefore, it is necessary to make clinical inferences and monitor tongue posture during interceptive and comprehensive orthodontic treatment to have better and more stable long-term results.
Several studies found statistically significant differences in pharyngeal airway dimension according to skeletal malocclusion.5,6,8,15,18,20,21,23,24,30-32 In this regard, Kaur et al.44) compared the three ANB groups statistically and found a significant difference in pharyngeal airway volume. They also concluded that the decreased pharyngeal airway dimension in Class II patients is due to the different location of the tongue and mandible. They also found that increased pharyngeal airway dimension in Class III is due to the anterior position of the mandible and the lower tongue position. However, Clokotiya et al.26 concluded that pharyngeal airway dimensions are not affected by ANB angle changes.
Regarding the connection between these structures and skeletal malocclusion, several studies established a relationship between hyoid bone position and tongue position according to skeletal malocclusion. They found that hyoid bone position before and during orthodontic treatments guides us regarding tongue position and function29,34-37 due to an anterior displacement of the hyoid bone, which leads to changes in tongue movement. However, Seok33 found that the relationship between hyoid bone position and tongue position according to skeletal malocclusion was not statistically significant. However, he did find a positive correlation among patients with vertical growth. The studies consulted also mention a functional relationship between the tongue, the mandible, and the hyoid bone, represented by the existing muscular connections between these parts, such as the genioglossus, pharyngeal constrictor, geniohyoid, mylohyoid, and the two longitudinal muscles. These interrelationships should be considered during clinical diagnosis and treatment.28
Shokri et al.8 and Ulusoy et al.29 found that hyoid bone position correlates directly with pharyngeal airway dimensions and should be considered during orthognathic surgery because of the risk of airway obstruction. However, Ramos et al.30 concluded that the hyoid position is highly variable, so it was impossible to determine these dimensions accurately. They acknowledged, however, that there is insufficient evidence to state whether there is a statistically significant correlation between the hyoid bone and pharyngeal airway dimension.
Iwasaki et al.,2 Nejaim et al.,6 Shokri et al.,8 Lakshmi et al.,19 Tianhu et al.,20 Mendoza et al.,21 Silva et al.,22 Lopatiene et al.,23 Zadzeviciute et al.,31 and Tarkar et al.39 found significant differences in hyoid bone position, tongue position, and pharyngeal airway dimension in the three skeletal malocclusions. However, Chauhan et al.39 found no differences between angular measurements of the hyoid bone and Class I and Class II Division I malocclusions. They evaluated the relationship between pharyngeal airway dimension, tongue position, and hyoid bone in patients with different dentofacial patterns. They found no differences in either the anteroposterior dimension of the pharyngeal airway or in the position and relationship of the hyoid bone and tongue between patients with Class I and Class II Division I malocclusions. This may be due to the fact that only anteroposterior dimensions were considered. The anatomical landmarks and subdivision of the anatomical regions of the pharyngeal airway used in this study were different from those recommended, which makes it difficult to compare this with most other studies. The lack of a precise subregional definition of the pharyngeal airway in the literature limits its evaluation, making interstudy comparison difficult.
Liégeois et al.7 found a strong correlation between measurements obtained via CBCT and lateral cephalograms. Kaur et al.43 also concluded that both measurements are reliable and reproducible, but lateral cephalometric radiographs do not provide information on upper airway volumetric measurements. They confirmed that the CT airway volume shows more variability than the airway corresponding to the area. Abramson et al.44 correlated three-dimensional computed tomography findings between airway dimensions and lateral cephalometric measurements. The results showed that three-dimensional CT and lateral cephalometric measurements are reliable and reproducible. Vizzotto et al.45 evaluated the accuracy of airway measurements from lateral cephalograms, lateral CBCT reconstructions, and CBCT axial planes. They demonstrated that linear airway measurements are reliable with both lateral cephalograms and CBCT reconstruction.
Conclusions
There is no general consensus on the relationship between hyoid bone position, tongue position, and the upper airway dimension according to skeletal malocclusion in the articles reviewed.
Cephalometric and CBCT measurements are reliable and reproducible, with the difference that the latter also provides information on transverse and volumetric measurements.
The stomatognathic system should be evaluated, related, and assessed comprehensively and not partially. Additionally, cephalometric analysis techniques and regional anatomical subdivisions of the pharyngeal airway should be standardized. This will make it easier to compare the results of future studies.
REFERENCES
1. Proffit WR. Ortodoncia contemporánea. 4ta Ed. España: Editorial Elsevier; 2008 [ Links ]
2. Iwasaki T, Suga H, Minami A, Sato H, Hashiguchi M, Tsujii T. Relationships among tongue volume, hyoid position, airway volume and maxillofacial form in paediatric patients with Class-I, Class-II and Class-III malocclusions. Orthod Craniofac. 2019;22(1):9-15. [ Links ]
3. McNamara JA. Influence of respiratory pattern on craniofacial growth. Angle Orthod. 1981;51:269-300. [ Links ]
4. Moss M. The primary role of functional matrices in facial growth. Am J Orthod. 1959;55:566-567. [ Links ]
5. Kaur S, Rai S, Kaur M. Comparación de la confiabilidad del cefalograma lateral y la tomografía computarizada para la evaluación del espacio de las vías respiratorias. Niger J Clin Pract. 2014;17:629-36. [ Links ]
6. Nejaim Y, Johan K, Groppo F, Neto F. Evaluation of pharyngeal space and its correlation with mandible and hyoid bone in patients with different skeletal classes and facial types. American Journal of Orthodontics and Dentofacial Orthopedics. 2018;153(6):825-833. [ Links ]
7. Liégeois F, Albert A, Limme M. Comparison between tongue volume from magnetic resonance images and tongue area from profile cephalograms.Eur J Orthod. 2010; 32(4): 381-6. [ Links ]
8. Shokri A, Mollabashi V, Zahedi F, Tapak L. Position of the hyoid bone and its correlation with airway dimensions in different classes of skeletal malocclusion using cone-beam computed tomography. Imaging Science in Dentistry. 2020;50:105-15. [ Links ]
9. Mortazavi S, Asghari H, Dehghani M, Aboutorabzade M, Yaloodbardan B, Tohidi E. Hyoid bone position in different facial skeletal patterns. J Clin Exp Dent. 2018;10(4):346-51. [ Links ]
10. Adamidis L, Meropi N. Hyoid bone position and orientation in Class I and Class III maloclusions. Am J Orthod Dentofac, 1992;101:308-12. [ Links ]
11. Seher A, Neval D, Jalen k. Cephalometric Investigation of First Cervical Vertebrae Morphology and Hyoid Position in Young Adults with Different Sagittal Skeletal Patterns. Sci World J. 2014;1:1-8. [ Links ]
12. Fatima F, Mubassar F. The assessment of resting tongue posture in different sagittal skeletal patterns. Dental Press J Orthod. 2019;24(3):55-63. [ Links ]
13. Verma S, Tandon P, Agrawal D, Prabhat K. A cephalometric evaluation of tongue from the rest position to centric occlusion in the subjects with class II division 1 malocclusion and class I normal occlusion. J Orthod Sci. 2012; 1 (2): 34-9 [ Links ]
14. Primozic J, Farcnik F, Perinetti G, Richmond S, Ovsenik M. The association of tongue posture with the dentoalveolar maxillary and mandibular morphology in Class III malocclusion: a controlled study. Eur J Orthod. Junio de 2013; 35 (3): 388-93. [ Links ]
15. Iwasaki T, Sato H, Suga H, Takemoto Y, Inada E, Saitoh I, et al. Relationships among nasal resistance, adenoids, tonsils, and tongue posture and maxillofacial form in Class II and Class III children. Am J Orthod Dentofacial Orthop. 2017;151:929-40. [ Links ]
16. Yilmaz F, Sagdiç D, Karaçay S, Akin E, Bulakbasi N. Tongue movements in patients with skeletal Class II malocclusion evaluated with real-time balanced turbo field echo cine magnetic resonance imaging. Am J Orthod Dentofacial Orthop. 2011;139(5):e415-25. [ Links ]
17. Gorgülü S, Sagdic D, Akin E, Karacay S, Bulakbasi N. Tongue movements in patients with skeletal Class III malocclusions evaluated with real-time balanced turbo field echo cine magnetic resonance imaging. Am J Orthod Dentofacial Orthop. 2011; 139 (5): 405-14. [ Links ]
18. Oh K, Hong J, Kim Y, Cevidanes L, Ho P. Three-dimensional analysis of pharyngeal airway form in children with anteroposterior facial patterns. Ortod de ángulo. 2011; 81 (6): 1075-82. [ Links ]
19. Lakshmi K, Yelchuru S, Chandrika V, Lakshmikar O, Sagar V, Reddy G. Comparison between growth patterns and pharyngeal widths in different skeletal malocclusions in South Indian Population. J Int Soc Prevent Communit Dent. 2018;8:224-8. [ Links ]
20. Wang T, Yang Z, Yang F, Zhang M, Zhao J, Chen J, et al. A Three Dimensional Study of Upper Airway in Adult Skeletal Class II Patients with Different Vertical Growth Patterns. PLoS ONE. 2014; 9(4):955-44. [ Links ]
21. Mendoza J. Comparación de la dimensión del espacio aéreo faríngeo según las deformidades esqueléticas Clase I, II y III en radiografías cefalométricas de pacientes que asistieron a la clínica docente UPC entre los años 2011 al 2014 Pregrado. Universidad Peruana de Ciencias Aplicadas;2017. [ Links ]
22. Silva N, Lacerda R, Silva A, Ramos T. Assessment of upper airways measurements in patients with mandibular skeletal Class II malocclusion. Dental Press J Orthod. 2015;20(5):86-93. [ Links ]
23. Lopatiené K, Sidlauskas A, Vasiliauskas A, Cecyte L, Svalkauskiene V, Sidlauskas M. Relationship between malocclusion, soft tissue profile, and pharyngeal airways: A cephalometric study. Medicina (Kaunas). 2016;52(5):307-314. [ Links ]
24. Zheng ZH, Yamaguchi T, Kurihara A, Li HF, Maki K. Three-dimensional evaluation of upper airway in patients with different anteroposterior skeletal patterns. Orthod Craniofac Res. 2014;17(1):38-48. [ Links ]
25. Claudino LV, Mattos CT, Ruellas AC, Sant' Anna EF. Pharyngeal airway characterization in adolescents related to facial skeletal pattern: a preliminary study. Am J Orthod Dentofacial Orthop. 2013;143(6):799-809. [ Links ]
26. Chokotiya H, Banthia AKSR, Choudhary K, Sharma P, Awasthi N. A Study on the Evaluation of Pharyngeal Size in Different Skeletal Patterns: A Radiographic Study. J Contemp Dent Pract. 2018;19(10):1278-1283 [ Links ]
28. Jose N, Shetty S, Mogra S, Shetty V, Rangarajan S, Mary L. Evaluation of hyoid bone position and its correlation with pharyngeal airway space in different types of skeletal malocclusion. Contemp Clin Dent. 2014;5(2):187-9. [ Links ]
29. Ulusoy C, Canigur Bavbek N, Tuncer BB, Tuncer C, Turkoz C et al. Evaluation of airway dimensions and changes in hyoid bone position following class II functional therapy with activator. Acta Odontol Scand. 2014; 72 (8): 917-925. [ Links ]
30. Ramos M, Morales R, Samanamú S, Gómez A, Alva C. Posición del hueso hioides en relación al volumen de la vía aérea en los diferentes patrones esqueletales. Kiru. 2018;1(3):106-112. [ Links ]
31. Sadzeviciute E, Nazimova J, Trakiniene G. The impact of the hyoid bone position on the pharyngeal airway characteristics among different facial skeletal patterns. Stomatologija. 2019; 21(4):99-106. [ Links ]
32. Cheng J, Hsiao S, Chen C, Hsu K. Relationship between hyoid bone and pharyngeal airway in different skeletal patterns. J Dent Sci. 2020;15(3):286-293. [ Links ]
33. Seok J. Correlation analysis between tongue posture and hyoid bone position and cephalometric analysis variables in adult female patients. Korea J Orthod.2014;30(5):579-89. [ Links ]
34. Tallgren A, Solow B. Hyoid bone position, facial morphology and head posture in adults.Eur JOrthod.1987;9:1-8. [ Links ]
35. Haralabakis N, Toutountzakis N, Yiagtzis S. The position of the hyoid bone in adult individuals with an open bite and normal occlusion. Eur J Orthod.1993;15:265-271. [ Links ]
36. Subtelny J, Sakuda M. Open bite: diagnosis and treatment. Soy J Orthod.1964;50:337-358. [ Links ]
37. Castrillo A, Alonso M. Perez L, Colome G, Alaloya C, Medina S. Biotipo facial y posición hioidea en pacientes que inician tratamiento ortodóncico. Revista ADM. 2016;73(6):297-302. [ Links ]
38. Tarkar J, Parashar S, Gupta G, Bhardwaj P, Maurya R, Singh A et al. An evaluation of upper and lower pharyngeal airway width, tongue posture and hyoid bone position in subjects with different growth patterns. J Clin Diagn. 2016;10(1):79-83. [ Links ]
39. Chauhan A, Autar R, Lata K, Yadav V. Comparison of pharyngeal airway dimension, tongue and hyoid bone position based on ANB angle. Natl Maxillofac Surg. 2015;6(1):42-51. [ Links ]
40. Zou Y, Fu QM, Xu XY. Relationships among tongue volume, hyoid position, airway volume and maxillofacial form in pediatric patients with Class ?, Class ? and Class ? malocclusions. Shanghai Kou Qiang Yi Xue. 2020;29(6):632-637. [ Links ]
41. Tseng Y, Tsai F, Chou S, Hsu C, Cheng J, Chen C. Evaluation of pharyngeal airway volume for different dentofacial skeletal patterns using cone-beam computed tomography. J Dent Sci. 2021;16(1):51-57. [ Links ]
43. Kaur S, Rai S, Kaur M. Comparación de la confiabilidad del cefalograma lateral y la tomografía computarizada para la evaluación de las vías respiratorias. Niger J Clin Pract.2014;17:629-36. [ Links ]
44. Abramson ZR, Susarla S, Tagoni JR, Kaban L. Análisis tomográfico computarizado tridimensional de la anatomía de las vías respiratorias. J Oral Maxillofac Surg 2010; 68: 363-71. [ Links ]
45. Vizzotto MB, Liedke GS, Delamare EL, Silveira HD, Dutra V, Silveira HE. Un estudio comparativo de cefalogramas laterales e imágenes de tomografía computarizada de haz cónico en la evaluación de la vía aérea superior. Euro J de Ortodoncia 2011; 34: 390-3. [ Links ]
Authorship contribution 1. Conception and design of study 2. Acquisition of data 3. Data analysis 4. Discussion of results 5. Drafting of the manuscript 6. Approval of the final version of the manuscript MJEDLC has contributed in 1, 2, 3, 4, 5, and 6. LCSG has contributed in 1, 6. MMV has contributed in 5, 6.
Received: February 15, 2021; Accepted: August 06, 2021
 Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
