










Services on Demand
Journal

Article
 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Related links
Share

 Permalink
PermalinkOdontoestomatología
Print version ISSN 0797-0374On-line version ISSN 1688-9339
Odontoestomatología vol.23 no.38 Montevideo 2021 Epub Dec 01, 2021
https://doi.org/10.22592/ode2021n37e211
Research
Perception, knowledge, and attitude towards interceptive orthodontics among pediatric dentists, orthodontists, and dental surgeons in Peru

1Escuela de Odontología, Facultad de Medicina, Universidad Católica Santo Toribio de Mogrovejo, Perú
2Escuela de Posgrado, Doctorado en Investigación Clínica y Traslacional, Universidad Privada Antenor Orrego, Perú. marianoorpi@gmail.com
Objectives:
To compare the perception, knowledge, and attitude towards interceptive orthodontics among pediatric dentists, orthodontists, and dental surgeons.
Methods:
The sample included 52 men and 56 women, aged 39.75 ± 9.32 years: 36 pediatric dentists, 36 orthodontists, and 36 dental surgeons. The 14-question survey administered had validity, internal consistency, and stability. Survey Monkey was used to administer the survey. The data was analyzed using the chi-square test at a 5% significance level.
Results:
No differences were found among professionals regarding perception and attitude towards the treatment (p > 0.05). There was a difference regarding the level of knowledge about specific aspects of interceptive treatment (p < 0.05).
Conclusions
The professionals had similar perceptions and attitudes towards interceptive treatment. However, there was a significant difference regarding the level of knowledge of pediatric dentists, orthodontists, and dental surgeons.
Keywords: interceptive orthodontics; orthodontists; pediatric dentists; dentists
Objetivos:
Comparar la percepción, conocimiento y actitud hacia la ortodoncia interceptiva en odontopediatras, ortodoncistas y cirujanos dentistas.
Métodos:
La muestra se conformó por 52 hombres y 56 mujeres, con una edad de 39.75 ± 9.32 años e incluyó a 36 odontopediatras, 36 ortodoncistas y 36 cirujanos dentistas. Se utilizó un cuestionario de 14 preguntas con características de validez, consistencia interna y estabilidad. El instrumento fue enviado mediante el software Survey Monkey. El análisis de datos se realizó mediante prueba de Chi Cuadrado al 5% de significancia.
Resultados:
Los profesionales no mostraron diferencias en la percepción y en la actitud hacia el tratamiento (p>0.05). Existió una diferencia con respecto al nivel de conocimiento sobre aspectos puntuales del tratamiento interceptativo (p<0.05).
Conclusiones:
Los profesionales tuvieron similares percepciones y actitudes frente al tratamiento interceptativo. Sin embargo, existió una diferencia significativa con respecto al nivel de conocimientos entre odontopediatras, ortodoncistas y cirujanos dentistas.
Palabras clave: ortodoncia interceptiva; ortodoncistas; odontopediatras; dentistas
Objetivos:
Comparar a percepção, o conhecimento e a atitude em relação à ortodontia interceptiva em odontopediatras, ortodontistas e cirurgiões-dentistas.
Métodos:
A amostra foi composta por 52 homens e 56 mulheres, com idade de 39,75 ± 9,32 anos e incluiu 36 odontopediatras, 36 ortodontistas e 36 cirurgiões-dentistas. Foi utilizado um questionário de 14 questões com características de validade, consistência interna e estabilidade. O instrumento foi enviado usando o software Survey Monkey. A análise dos dados foi realizada por meio do teste Qui quadrado com significância de 5%.
Resultado:
Os profissionais não apresentaram diferenças de percepção e atitude em relação ao tratamento (p> 0,05). Houve diferença quanto ao nível de conhecimento sobre aspectos específicos do tratamento interceptativo (p <0,05).
Conclusões:
Os profissionais tiveram percepções e atitudes semelhantes em relação ao tratamento interceptativo. No entanto, houve diferença significativa quanto ao nível de conhecimento entre odontopediatras, ortodontistas e cirurgiões-dentistas.
Palavras-chave: ortodontia interceptiva; ortodontistas; odontopediatras; dentistas
Introduction and background
Evidence shows that treating malocclusion early has fewer unfavorable effects and that they may even be eliminated.1 However, not much is known about the true benefits of interceptive orthodontics at the highest desired level of evidence, so some gaps remain.2
Malocclusion has a vast etiology, but its results are quite common: unaesthetic appearance, patient discomfort, periodontal problems, chewing difficulty, and speech problems. These require a multidisciplinary approach led by dental surgeons and specialists, who should base their decisions on orthodontic principles and practices.3 It is estimated that 65.1% of all orthodontic cases are treated by orthodontic specialists, 3.7% by pediatric dentists, and 31% are treated by general practitioners.4 However, there is much controversy regarding the skills of practitioners providing orthodontic treatment.5,6
Assessing the need for orthodontic treatment depends on the practitioner's experience and training. In most countries, specialists attend advanced education programs for 2-3 years after dental school to train in the diagnosis and treatment of malocclusions. Training in diagnosing and/or treating patients with interceptive orthodontics may be insufficient given the time constraints of undergraduate plans of studies.4,6
Studies have reported that pediatric dentists, dental surgeons, and orthodontists performing early diagnosis and interceptive treatment of malocclusion have clinical management discrepancies.3,5,7 Treatments vary according to malocclusion type. For instance, some orthodontists would use headgear to treat an anterior open bite, whereas pediatric dentists and dental surgeons prefer a functional or removable dentoalveolar appliance.5 The same applies to crowding, where the treatment approach may range from using a functional appliance to serial extraction.5,8
Pediatric dentists and dental surgeons also have differences in their treatment of choice. They usually treat any type of malocclusion, mainly in primary and early mixed dentition, and they have a different referral rate.4,5,9 Some studies report a significant percentage of general dentists who decide not to refer patients to a specialist and provide some type of interceptive treatment but with a more general approach.4,10
Given the potential differences in the professionals who provide interceptive orthodontic care, it is essential to understand that their perception and attitudes towards diagnosing, preventing, and treating malocclusions may vary. This can have a direct or indirect impact on the success of interceptive orthodontic treatment. This study aims to compare the perception, knowledge, and attitude towards interceptive orthodontics among pediatric dentists, dental surgeons, and orthodontists.
Methods
This study was approved and independently reviewed by the Research Ethics Committee of Universidad Católica Santo Toribio de Mogrovejo under resolution number 410-2020-USAT-FMED. All participants received an oral and written explanation of the study and gave their consent voluntarily.
This study is observational, and the population was made up of professionals who provide preventive orthodontic treatment to children or adolescents. These were both men and women registered with the Peruvian Dental Association and who agreed to participate in the survey. Participants with an inactive e-mail, no cellular phone data, and those who did not send the survey through the link provided were excluded.
Study sample
The sample was determined with this formula for studies using the nonparametric chi-square test with ? = 0.05, ? = 0.10, and with ratios obtained from a pilot study.


This resulted in a minimum sample size of 108 professionals, with a 0.90 power for the study.
The sample was proportionally divided into 36 professionals per group, and the sample was selected through non-probability convenience sampling.
Technique and survey
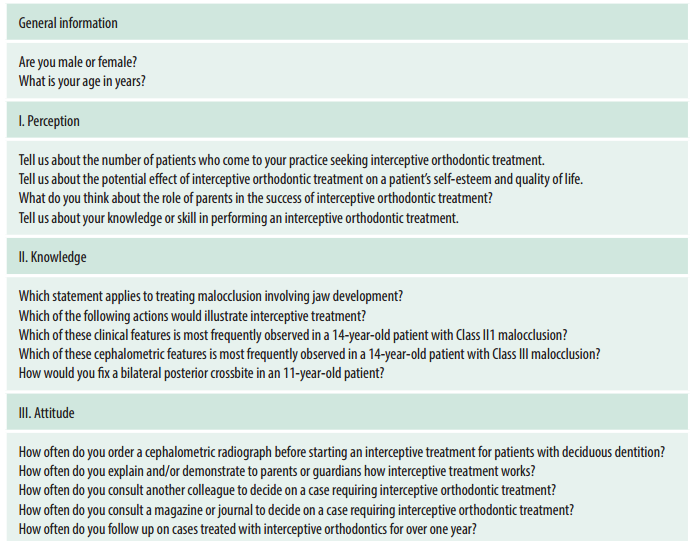
This study was conducted through a self-administered online survey. The questionnaire or survey was divided into two sections: general information about the professional, and interceptive orthodontics. The second section had two subsections: perception (4 questions), knowledge (5 questions), and attitude (5 questions). Dichotomous questions were used to assess knowledge: correct (1 point) and incorrect (0 points). The questions to evaluate perception and attitude were asked on a 5-point Likert scale: always (5 points), often (4 points), regularly (3 points), sometimes (2 points), and never (1 point). Table 1 shows the survey's sections and questions included in the study.
The content of the sections was validated with the participation and evaluation of three reviewers or experts (MCH, MAT, AAN) who applied a previously developed validation matrix. The test-retest based stability results for perception, knowledge, and attitude were 0.644 (p = 0.002 < 0.01), 0.795 (p = 0.000 < 0.001) and 0.912 (p = 0.000<0.001). This shows that the scales used were stable. Internal consistency was adequate; the coefficients were 0.723, 0.699, and 0.685 for perception, knowledge, and attitude.
Procedure
The research staff entered the survey's questions and answers into the Survey Monkey online platform and default fields. Microsoft Excel was used to create a database including specific information on the study variables and information about the respondent: full name, phone number, and/or e-mail. These were initially provided to the research staff. The information was tabulated for each participant. Then, practitioners were classified according to the type of professional: pediatric dentist, orthodontist, or general dental surgeon. The professionals were classified using information from the website of the National Registry of Degrees and Diplomas of the National Superintendence of University Higher Education (SUNEDU), which is free and publicly accessible.
Before collecting the data, each participant was given a data sheet with information on the research objectives, the head researcher, and the confidentiality of the information provided. The participants' data was entered into the survey software. Then, the platform automatically sent the participants a link to access the survey. The software sends automatic recurring messages according to the participants' response rate. The information obtained from the completed surveys was assigned identification codes for each participant.
Statistical analysis
All the data was processed using SPSS 25.0 statistical software. Univariate statistical analysis was performed for the study variables using absolute and relative frequencies to present the data. A bivariate analysis was also performed using the chi-square test to compare the perception, knowledge, and attitude towards interceptive treatment among the three groups of professionals, with a 5% significance level.
Results
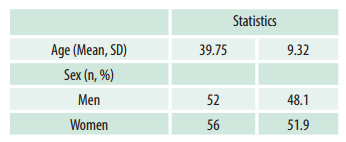
Of the 113 people selected for the sample, a total of 108 professionals, both men, and women, agreed to participate in the study, which amounts to a 95.3% response rate. Table 2 shows the characteristics of the study participants.
Regardless of the type of professional, the perception of interceptive treatment was generally favorable: 91.7% in orthodontists, 88.9% in pediatric dentists, and 83.3% in dental surgeons. Table 3 shows that the overall high perception does not provide evidence of any significant difference between the perception reported by the various professionals (p=0.542).
Table 3: Perception of interceptive treatment by dental surgeons, pediatric dentists, and orthodontists

(*) Chi-square statistical test.
Regarding the level of knowledge of specific aspects of interceptive treatment, the most frequent level of knowledge was fair: 83.4% in dental surgeons, 61.1% in pediatric dentists, and 52.8% in orthodontists. Table 4 shows that a significant percentage of orthodontists (38.9%) and pediatric dentists (33.3%) replied that the level was good, which shows a statistically significant difference (p=0.039).
Table 4: Knowledge of interceptive treatment of dental surgeons, pediatric dentists, and orthodontists
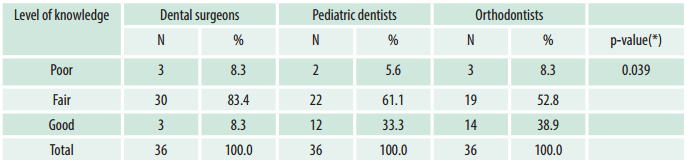
(*) Chi-square statistical test.
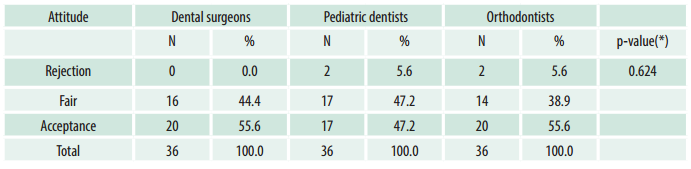
Regarding attitude towards interceptive treatment, there was a shared perspective. Generally, there was an attitude of acceptance and of uncertainty (fair). Dental surgeons and orthodontists (55.6%) and pediatric dentists (47.2%) had a similar acceptance level. As for uncertainty, the percentages were 47.2% for pediatric dentists, 44.4% for dental surgeons, and 38.9% for orthodontists. Table 5 shows no statistical differences between the groups for acceptance.
Discussion
The benefits of interceptive treatment versus no treatment or delayed treatment remain controversial.11 Thus, for example, functional appliances may effectively correct long-term skeletal Class II malocclusion. However, the quality of the evidence is still low and the clinical significance is limited.12 Similarly, there is evidence supporting the use of facemasks to treat skeletal Class III malocclusion, but with limited long-term results.13 The lack of adequate clinical trials and the failure to evaluate other factors such as patient satisfaction, pain experience, and cost14 contribute to the practitioners' idea that this procedure is debatable.
Interceptive orthodontics has adopted a multidisciplinary approach where general dentists and other specialists such as pediatric dentists can play a significant role in diagnosis and treatment. However, possible variations in education and perceptions of orthodontic treatment may create differences if the dentists have a specialization degree.15,16 The results of this study show differences in education and training among the professionals who provide interceptive orthodontic treatment. However, some aspects regarding perception and attitude towards certain situations are similar.
No differences were found regarding the perception of the demand of patients seeking interceptive treatment, the benefit of treatment on the patient's self-esteem and quality of life, the role of parents, and the professionals' perception of their own skills. Hunt et al.17 compared the perception of orthodontists and general dental practitioners. They agree that this treatment improves self-esteem and quality of life; orthodontists obtained a higher score. This study also showed a higher percentage of orthodontists who had a favorable perception of the treatment, and no statistical difference was found. Heath et al.6 evaluated the perception among the same professionals regarding their orthodontic treatment skills. They found a considerable difference in favor of the specialists, which contrasts with this study, where most professionals believed they had adequate skills to provide interceptive treatment.
We found significant differences in the professionals' level of knowledge on how to treat these cases. Most professionals with a good level of knowledge were orthodontists. Among the respondents with poor knowledge, the minority were pediatric dentists. General dental surgeons were the largest group in the fair knowledge category. These results coincide with Barzilay et al.10, who evaluated knowledge of interceptive orthodontics among dental surgeons and pediatric dentists. They assigned a significantly higher score to pediatric dentists. However, the results of this study differ from those of Aldrees et al.,5 who found no differences in diagnostic skills regarding most malocclusions assessed through clinical cases. The difference between the studies above may be due to the different formats used to assess diagnostic skills. According to Ghafari18 and You et al.,19 it may also be due to the diversity of orthodontic skills offered and how they are acquired in each undergraduate and graduate program, despite the globalization of orthodontic education. This study presented specific situations, which demanded accurate clinical responses. This may have made structured decision-making difficult when professionals with less training had to diagnose and treat patients in specific clinical scenarios.
Once the level of knowledge has been identified, it is necessary to evaluate attitudes to interpret the impact on our clinical treatment decisions. This is a tool that allows professionals to improve constantly. In this study, most dental surgeons, pediatric dentists, and orthodontists had a similar attitude of accepting the situations presented to the point that no general dental surgeon rejected the topics evaluated regarding interceptive orthodontic treatment. Currell et al.20 found that general dental surgeons' attitude towards interceptive orthodontic treatment depended on factors such as selfconfidence and doubts about the benefits of the treatment, results that differ from those of this study. This could be explained by dental surgeons' predisposition to be more efficient in relation to interceptive treatment, regardless of their training compared to that of specialists.
In most countries such as Peru, interceptive orthodontic treatment is often provided by pediatric dentists, orthodontists, and general dental surgeons. Therefore, it is interesting to see no differences in perception and attitude towards the treatment despite possible differences in training in undergraduate and specialty programs. This can be seen as a starting point for common ground for general and specialized care.
This study had the limitation that the knowledge of specialists and non-specialists was evaluated according to theoretical background only and not necessarily according to clinical experience, which could change the professionals' opinion about orthodontic treatment. In this sense, the answers provided may not represent the respondents' actual clinical practice. Therefore, these findings should be treated with caution.
Conclusions
General dental surgeons, pediatric dentists, and orthodontists who provide interceptive orthodontic treatment in Peru were mostly similar in their favorable perception of interceptive treatment and acceptance in clinical situations. In general, there was a significant difference in the level of knowledge when comparing the three types of professionals, although most of them had a fair performance in the topics evaluated.
REFERENCES
1. Keski-Nisula K, Keski-Nisula L, Varrela J. Class II treatment in early mixed dentition with the eruption guidance appliance: effects and long-term stability. Eur J Orthod. 2020; 42(2):151-156. [ Links ]
2. Artese F. A broader look at Interceptive Orthodontics: What can we offer?. Dental Press J. Orthod. 2019; 24(5):7-8. [ Links ]
3. Kapoor D, Bhatia S, Garg D. Assessment of the attitude and knowledge of the principles and practices of orthodontic treatment among the non-orthodontic specialists and general practitioner dentists. J. Nepal Med. Assoc. 2018; 56(1):766-9. [ Links ]
4. Batarse AP, English JD, Frey GN, Piazza JM, Akyalcin S. Referral patterns of pediatric dentists and general practitioners to orthodontists based on case complexity. Am. J. Orthod. Dentofacial Orthop. 2019;156(1): 61-6. [ Links ]
5. Aldrees AM, Tashkandi NE, Al-Wanis AA, Al-Sanouni MS, Al-Hamlan NH. Orthodontic treatment and referral patterns: A survey of pediatric dentists, general practitioners and orthodontists. Saudi Dent. J. 2015; 27(1):30-9. [ Links ]
6. Heath EM, English JD, Johnson CD, Swearingen EB, Akyalcin S. Perceptions of orthodontic case complexity among orthodontists, general practitioners, orthodontic residents, and dental students. Am J Orthodont Dentofac Orthop 2017; 151(2): 335-41. [ Links ]
7. Quinzi V, Ferro R, Rizzo FA, Marranzini EM, Federici-Canova F, Mummolo S, Mattei A, Marzo G. The Two by Four appliance: a nationwide cross-sectional survey. Eur. J. Paediatr. Dent. 2018;19(2):145-50. [ Links ]
8. Caplin J, Han MD, Miloro M, Allareddy V, Markiewicz MR. Interceptive Dentofacial Orthopedics (Growth Modification). Oral Maxillofac. Surg. Clin. North Am. 2020; 32(1): 39-5. [ Links ]
9. Mahmood R, Dayar J, Ahmed Z. Evaluation of awareness among general dentists for referral of patients needing orthodontic treatment. Pak J. Med. Health Sci. 2019; 4(1): 326. [ Links ]
10. Barzilay V, Ratson T, Sadan N, Dagon N, Shpack N. Orthodontic knowledge and referral patterns: a survey of paediatric specialists and general dental practitioners. Aust. Orthod. J. 2020;36(1): 55. [ Links ]
11. Sunnak R, Johal A, Fleming PS. Is orthodontics prior to 11 years of age evidence-based? A systematic review and meta-analysis. J. Dent. 2015; 43(5):477-86. [ Links ]
12. Cacciatore G, Ugolini A, Sforza C, Gbinigie O, Plüddemann A. Long-term effects of functional appliances in treated versus untreated patients with Class II malocclusion: A systematic review and metaanalysis. PLoS One. 2019; 14(9): e0221624. Disponible en: https://doi.org/10.1371/journal.pone.0221624 [ Links ]
13. Woon SC, Thiruvenkatachari B. Early orthodontic treatment for Class III malocclusion: A systematic review and meta-analysis. Am J Orthod Dentofacial Orthop. 2017;151(1):28-52. [ Links ]
14. Elangovan B, Pottipalli Sathyanarayana H, Padmanabhan S. Effectiveness of various interceptive treatments on palatally displaced canine-a systematic review. Int Orthod. 2019;17(4):634-642. [ Links ]
15. Acharya A, Mishra P, Shrestha RM, Shah P. Orthodontic treatment knowledge among general dentists and non-orthodontic specialists. Orthod. J. Nepal. 2019; 9(1): 39-43. [ Links ]
16. Imran ML, Abdurazaq MR, Kumar KN. Attitude and knowledge of orthodontics among general dentists and non-orthodontic specialists: a questionnaire based survey. Int. J. Dent. Oral Sci. 2020; 7(9): 815-20. [ Links ]
17. Hunt O, Hepper P, Johnston C, Stevenson M, Burden D. Professional perceptions of the benefits of orthodontic treatment. Eur. J. Orthod. 2001; 23: 315-23. [ Links ]
18. Ghafari JG. Ways and pathways of global orthodontic postgraduate education. Seminars in Orthodontics. 2020; 26(4): 188-98. [ Links ]
19. You QL, Qian YF, Shen G. Study on the teaching mode and quality management of orthodontic education in undergraduates. Shanghai Kou Qiang Yi Xue. 2011; 20(3):324-7. [ Links ]
20. Currell SD, Matthew V, Craig WD. Interceptive Orthodontic Practices in General Dentistry: A Cross-Sectional Study. Australasian Orthodontic Journal. 2019 35(2): 152-7. [ Links ]
1Authorship contribution 1. Conception and design of study 2. Acquisition of data 3. Data analysis 4. Discussion of results 5. Drafting of the manuscript 6. Approval of the final version of the manuscript. MOrtiz has contributed in: 1, 3, 5, and 6. Rpachas has contributed in: 1, 2, 4, and 6.
Conflict of interest: The authors declare no conflict of interest regarding the conception, execution, and information of this study. This research was not funded by any particular company or individual.
Received: June 20, 2021; Accepted: July 30, 2021
 Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
