










Servicios Personalizados
Revista

Articulo
 texto en
texto en  Español (pdf)
Español (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Curriculum ScienTI
Curriculum ScienTILinks relacionados
Compartir

 Permalink
PermalinkOdontoestomatología
versión impresa ISSN 0797-0374versión On-line ISSN 1688-9339
Odontoestomatología vol.23 no.37 Montevideo 2021 Epub 30-Mayo-2021
https://doi.org/10.22592/ode2021n37a11
Case report
Large dentigerous mandibular cyst treated in two surgical steps. A case report
1
 http://orcid.org/0000-0002-0251-1475
http://orcid.org/0000-0002-0251-1475
2
http://orcid.org/0000-0002-1966-6385
2
http://orcid.org/0000-0003-1429-6351
1Cirugía Bucomaxilofacial. Facultad de Odontología de Recife, FOR, FOPCB, Recife, Brasil
2Facultad de Odontología de Recife, FOR, FOPCB, Recife, Brasil
3Odontología Hospitalaria, Instituto de Ciencias Biológicas, Universidad de Pernambuco, Brasil
A dentigerous cyst is a benign lesion arising from the odontogenic epithelium associated with the crown of an impacted tooth. They are radiolucent and unilocular, usually asymptomatic and diagnosed in clinical routine or radiographic examinations. The lower third molars and upper canines are the most affected teeth, and the lesion is also associated with odontomas and supernumerary teeth. The cyst is slow-growing but can reach considerable dimensions, causing facial deformity, impaction, and displacement of teeth or adjacent structures. This study aims to report the clinical case of a large mandibular dentigerous cyst treated in two stages: biopsying and decompressing the lesion and enucleating the cyst capsule. It was thus possible to accurately diagnose the lesion, reduce its size to allow for total enucleation with minimal damage to the surrounding anatomical structures, and preserve sensitive function. A five-year follow-up was performed, with full lesion healing.
Keywords: oral surgery; dentigerous cyst; odontogenic cysts; oral pathology
El quiste dentígero es una lesión benigna que se origina en el epitelio odontogénico asociado a la corona de un diente incluido. Son radiolúcidos y uniloculares, generalmente asintomáticos y diagnosticados en exámenes de rutina o exámenes radiográficos. Los terceros molares inferiores y los caninos superiores son los dientes más afectados, y esta lesión también ocurre en dientes supernumerarios o asociados a odontomas. De crecimiento lento puede alcanzar dimensiones considerables, provocando deformidad facial, impactación y desplazamiento de dientes y/o estructuras adyacentes. El objetivo de este trabajo es informar un caso clínico de un voluminoso quiste dentígero mandibular, que se trató quirúrgicamente en dos etapas: la primera intervención con fines de biopsia y descompresión de la lesión y la segunda con el objetivo de enuclear la cápsula remanente. De esta forma, fue posible realizar un diagnóstico preciso de la lesión, reducir su tamaño para permitir una enucleación total con un daño mínimo a las estructuras anatómicas circundantes y la preservación de la función neurosensorial. Se realizó el seguimiento del paciente durante un período de 5 años en el posoperatorio, y el caso evolucionó hasta la curación total.
Palabras clave: Cirugía bucal; Quiste dentígero; Quistes odontogénicos; Patología bucal
O cisto dentígero é uma lesão benigna oriunda do epitélio odontogênico associado à coroa de um dente incluso. São radiolúcidos e uniloculares, normalmente assintomáticos e diagnosticados em exames de rotina ou exame radiográfico. Os terceiros molares inferiores e os caninos superiores são os dentes mais acometidos, tendo também ocorrência desta lesão em dentes supranumerários ou associados a odontomas. De crescimento lento pode atingir dimensões consideráveis, causando deformidade facial, impactação e deslocamento de dentes e/ou estruturas adjacentes. O objetivo deste trabalho é relatar um caso clínico de volumoso cisto dentígero mandibular, tratado cirurgicamente em duas etapas: a primeira intervenção com fins de biópsia e descompressão da lesão e uma segunda com intuito de enuclear a capsula rôta. Desta forma pôde-se realizar o diagnostico preciso da lesão, diminuir seu tamanho de forma a permitir a enucleação total com o mínimo de dano as estruturas anatômicas circunvizinhas e a preservação da função neurossensorial. O paciente foi acompanhado por um período de 05 anos no pós operatório, tendo o caso evoluído para a cura total.
Palavras-Chaves: Cirurgia Bucal; Cisto Dentígero; Cistos Odontogênicos; Patologia Bucal
Introduction
A dentigerous cyst is one of the most frequent benign intraosseous lesions among developmental odontogenic cysts. It is associated primarily with impacted third molars and upper canines. It tends to appear in individuals in the second to fourth decades of life1,2,3,4. They are usually asymptomatic, slow-growing, and are discovered incidentally during routine radiographic evaluation3,5. X-ray imaging shows a unilocular radiolucent lesion with well-defined scleral edges on the crown of the impacted tooth6. Cortical expansion and root resorption are commonly found. Differential diagnoses may include cystic lesions, such as keratocyst and primary cyst, and odontogenic tumors such as ameloblastoma, unilocular ameloblastoma, ameloblastic fibroma, and adenomatoid odontogenic tumors7. Histologically, most dentigerous cysts are a pathological cavity lined by layered flat epithelium5,9. Some cases also have an organized loose fibrous connective tissue capsule, islands or strands of odontogenic epithelium, dystrophic calcifications, and an inflammatory infiltrate of varying intensity9. Most frequent treatments include careful cyst enucleation and removal of the impacted tooth4,10,11. Larger cysts can be treated with marsupialization-facilitating decompression and enucleation-following a conservative elective surgical procedure4,5. Prognosis is excellent in most cases, and cyst recurrence is rare3,8,12.
Case report
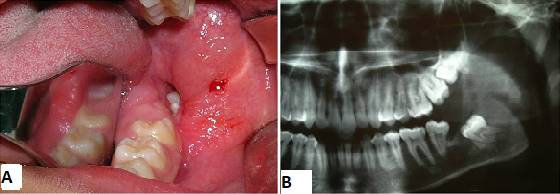
Male patient of African descent aged 17, a student born in Fortaleza, state of Ceará, Brazil, sought care in a private dental clinic with complaints of mouth suppuration. The patient’s mother informed us that he had felt a bad taste in his mouth for about a month. A clinical dental surgeon ordered a panoramic x-ray of the jaws, detected the lesion, and referred him to an oral and maxillofacial surgeon. His medical history did not include any complaints of pain: he had only reported a bad taste in the mouth and bad breath. The extraoral physical examination showed symmetrical facies and absence of facial deformities. Nodal chains of the cervicofacial complex presented no alterations. On intraoral examination, a suppuration was visible in the lingual and distal gingival sulcus in the region of tooth 37. There was a discrete elevation in the region of the left retromolar trigone with fluctuation point and liquid consistency. The panoramic radiograph showed an extensive osteolytic lesion in the left mandibular angle and ascending branch region, of expansive appearance, associated to and including tooth 38, displaced towards the basilar bone (Fig. 1).

A cone-beam volumetric tomography was ordered to better assess the extent of the lesion, which showed the lesion's anatomical boundaries and relationships (Fig. 2).

The diagnostic hypothesis was dentigerous cyst, ameloblastoma, or odontogenic keratocyst after assessing the medical history, physical examination, and complementary examinations. The treatment was accepted by the responsible adults, who read, agreed to, and signed the free and informed consent form. The treatment entailed performing a marsupialization biopsy under general anesthesia to diagnose and decompress the lesion (as delayed therapy). The surgery was scheduled after ordering routine preoperative exams, which were within the normal standards.
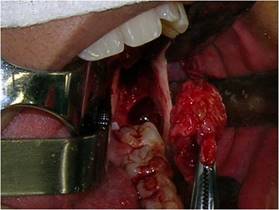
Nasotracheal intubation was done under general anesthesia after extra and intraoral antisepsis with 2 and 0.12% chlorhexidine. The operative field was placed, and the oropharynx cross-section was packed. Subperiosteal infiltration was performed at the retromolar trigone region-where there was cortical erosion due to fluctuation-with 0.5% bupivacaine hydrochloride solution with 1:200,000 epinephrine hemitartrate to promote hydrodissection of the periosteum and hemostasis. Next, aspiration was performed with a 10 cm³ Luer syringe with a 40X12 needle, and abundant seropurulent liquid was collected (Fig. 3).

In sequence, a circumferential incision was made with a #3 scalpel handle equipped with a 15 blade, deep enough to penetrate the lesion. This tissue was removed, and a fragment of the lesion capsule was also removed separately to obtain a more specific lesion sample (Fig. 4).

All the extracted material was immediately fixed in a 10% formalin solution. Isolated stitch sutures were performed throughout the resected area, encompassing the lesion capsule and surrounding mucosa (Fig. 5). After cleansing the cavity with saline solution, the remaining cavity was packed with medicated dressing impregnated with 5 mg/g neomycin sulfate and bacitracin zinc 250 IU ointment.

A week later, the medicated dressing and suture were removed. The cavity was left open, and the patient and his parents were instructed on the need for rigorous hygiene with constant irrigation with water and antiseptic substances (mouthwash) during the regression waiting period.
The histopathological examination was compatible with a dentigerous cyst. Given this result, the clinicians decided to wait for the lesion regression to minimize the likelihood of surgical damage of noble anatomical structures in the perilesional region (inferior alveolar neurovascular bundle and adjacent teeth).
A year after the first intervention, there was a clinically and radiographically significant reduction of the lesion (Figs. 6 A and 6 B). The next step was to enucleate the remaining cyst capsule and teeth 38, 18, 28, and 48 under general anesthesia.
Teeth 18, 28, and 48 were initially extracted by applying traditional surgical techniques. The remaining cyst was then addressed through an elliptical incision of approximately 0.5 cm from the opening of the decompression area. After total enucleation of the remaining cystic capsule and tooth 38 (Fig.7), the cavity was packed with medicated dressing as in the first intervention (Fig.8).

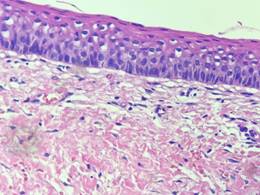
Histopathological examination of the surgical specimen confirmed the initial diagnosis of dentigerous cyst (Figure 9).
The stitches were removed seven days after surgery without any complications. Unlike the first intervention, where no bone structure was exposed, in this surgery, the dressing was replaced after irrigation with saline solution. Then, the surgical cavity was aspirated weekly until full epithelialization of the surgical cavity. This took place four weeks after surgery.
The patient was followed up clinically and radiographically every three months for one year and then annually for five years. Figs 20 A and 10 B show the final clinical and radiographic appearance five years after surgery, where complete bone neoformation is observed.
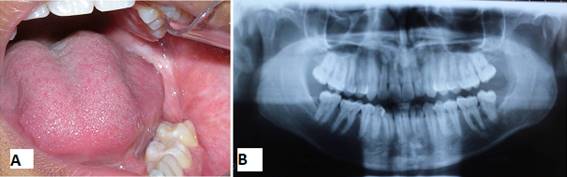
After this follow-up period, the patient was discharged as there was no clinical-radiographic evidence of recurrence.
Discussion
As described in the literature, a dentigerous cyst is a benign intraosseous lesion more frequent than odontogenic cysts1,2,3,4. They are usually asymptomatic and slow-growing, generally discovered incidentally during routine clinical and radiographic evaluation3,5. X-ray imaging shows these lesions as unilocular radiolucent injuries with well-defined scleral edges on the crown of the impacted tooth6. However, they can also be symptomatic, as in this case report, with an associated secondary infection causing suppuration as the patient’s main complaint. Frequently found cortical expansion and root resorption were not clinically visible because of the size of this lesion.
Histologically, dentigerous cysts are characterized in most cases as a pathological cavity, lined by layered flat epithelium5,9. In some cases, there is a loose fibrous connective tissue capsule, islands or strands of odontogenic epithelium, dystrophic calcifications, and an inflammatory infiltrate of varying intensity9. This is compatible with the histopathological range of this case report.
We agree that the proper treatment in most cases is careful cyst enucleation and removal of the impacted tooth4,10,11 when the tooth is not viable. This allows professionals to entirely remove the affected tissue, preventing the tissue from becoming a tumor cell provider. Larger cysts can be treated with decompression (marsupialization)4,5, allowing for an accurate diagnosis and decompression. Then, the remaining capsule can be enucleated without risking surrounding noble anatomical structures such as the inferior alveolar neurovascular bundle and adjacent vital teeth. This was the procedure in this case.
Prognosis is excellent in most cases, and cyst recurrence is rare3,8,12 as seen in this case: evolution until complete lesion healing.
Conclusion
In view of the above, we can conclude that two-stage intervention is extremely valuable in large cystic lesions of the maxillomandibular complex because it allows for an accurate diagnosis of the type of lesion and minimizes surgical sequelae. It also preserves vital adjacent teeth and noble anatomical structures, such as the inferior alveolar neurovascular bundle.
REFERENCES
1. Pulido Valladares Y, Torres Rodríguez LE, Gounelas Amat S. Quiste dentígero en la atención pediátrica multidisciplinaria. Rev Ciencias Médicas (Internet). 2019 Jun (citado 2020 Oct 17) ; 23( 3 ): 473-479 [ Links ]
2. vasconcelos, MG et al. Localização incomum de cisto dentígero relato de caso. Scientific-Clinical Odontology 2017; 16(4): 200 [ Links ]
3. Lacerda EPM, Martorelli SBF, Martorlelli FO. Dentigerous cyst in the maxillary posterior region associated with an impacted deciduous molar. RGO, Rev. Gaúch. Odontol. (Internet). 2018 June (cited 2020 Oct 15) ; 66( 2 ): 194-198. Disponible en: Disponible en: http://www.scielo.br/scielo.php?script=sci_arttext&pid=S1981-86372018000200194&lng=en [ Links ]
4. lacerda SHT. Aproveitamento de dentes retidos e associados com cisto dentígero após marsupialização: série de casos. 2015. Revista Intercâmbio 2017; 12: 165 [ Links ]
5. Bertolo-Domingues N, Girotto-Bussaneli D, Jeremias Fabiano A, Giro EM, Aguiar-Pansani C. Diagnóstico y tratamiento conservador de quiste dentígero: seguimiento a 3 años. CES odontol. (Internet). 2018 June (cited 2020 Oct 15) ; 31( 1 ): 57-65. Available from: http://www.scielo.org.co/scielo.php?script=sci_arttext&pid=S0120-971X2018000100057&lng=en. [ Links ]
6. Morais HHA et al. Bilateral mandibular dentigerous cysts: a case report. RGO, Rev. Gaúch. Odontol. (Internet). 2014 Sep (cited 2020 Oct 15) ; 62( 3 ): 299-304. Available from: Available from: http://www.scielo.br/scielo.php?script=sci_arttext&pid=S1981-86372014000300299&lng=en [ Links ]
7. Patil AS, Jathar PN, Panse AM, Bahutule SR, Patil RU, Patil M. Infected Dentigerous Cyst and its Conservative Management: A Report of Two Cases. Int J Clin Pediatr Dent. 2019 Jan-Feb;12(1):68-72. doi: 10.5005/jp-journals-10005-1578. [ Links ]
8. Spini RG, Bordino L, Cruz D, Fitz Maurice Mde L, Martins A, Michalski J. Quiste dentígero: reporte de un caso (Dentigerous cyst: a case report). Arch Argent Pediatr. 2016 Oct 1;114(5):e338-42. doi: 10.5546/aap.2016.e338. Epub 2016 Oct 1. [ Links ]
9. Morales ND, Díaz Ramos AG. Quiste dentígero en tercer molar mandibular en posición invertida. Rev Cubana Estomatol (Internet). 2018 Sep (citado 2020 Oct 17) ; 55( 3 ): 1-8 [ Links ]
10. Lee JY. Dentigerous Cyst Associated With a Supernumerary Tooth. Ear Nose Throat J. 2020 Jan;99(1):32-33. doi: 10.1177/0145561318823638. Epub 2019 Jan 28. [ Links ]
11. Sardana D, Goyal A, Gauba K. Manejo de um cisto dentígero inflamado em um paciente com mordida cruzada anterior, usando um obturador modificado. S. Afr. dente. j. (Internet). 2016 (citado 18 de octubre de 2020); 71 (6): 266-269. Disponible en: Disponible en: http://www.scielo.org.za/scielo.php?script=sci_arttext [ Links ]
12. Jain N, Gaur G, Chaturvedy V, Verma A. Cisto dentígero associado com pré-molar maxilar impactado: uma ocorrência de local raro e uma coincidência rara. Int J Clin Pediatr Dent. 2018 de janeiro a fevereiro; 11 (1): 50-52. doi: 10.5005 / jp-journals-10005-1483. Epub 1 de fevereiro de 2017. [ Links ]
Authorship contribution: 1) Conception and design of study 2) Acquisition of data 3) Data analysis 4) Discussion of results 5) Drafting of the manuscript 6) Approval of the final version of the manuscript SBFM has contributed in 1,2,3,4,5,6. CLCDL has contributed in 1,2,5. DSGL has contributed in 1,2,5. MRB has contributed in 1,2,5. LALH has contributed in 1,2,5,6.
Received: November 03, 2020; Accepted: February 19, 2021
 Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
