










Servicios Personalizados
Revista

Articulo
 texto en
texto en  Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
Links relacionados
Compartir

 Permalink
PermalinkOdontoestomatología
versión impresa ISSN 0797-0374versión On-line ISSN 1688-9339
Odontoestomatología vol.22 no.36 Montevideo 2020 Epub 01-Dic-2020
https://doi.org/10.22592/ode2020n36a2
Research
Oral health-related quality of life in Perúvian children with severe early childhood caries

1Facultad de Odontología. Universidad Nacional Mayor de San Marcos. Lima, Perú.
2Facultad de Medicina. Universidad Nacional Mayor de San Marcos. Lima, Perú.
3Instituto Nacional de Salud del Niño. Lima, Perú
Objective:
To evaluate parental perception of the quality of life related to the oral health of children with severe early childhood caries from a Perúvian health institute.
Method:
An observational, analytical, and cross-sectional study was carried out in 200 children aged 3 to 5, without caries and children with severe early childhood caries (S-ECC) selected randomly. A calibrated examiner applied the Perúvian version of the ECOHIS questionnaire (P-ECOHIS) and the dmfs index. The normal distribution was determined with the Kolmogorov-Smirnov test; the Mann-Whitney U statistical test was also applied.
Results:
The total ECOHIS score is higher in children with S-ECC than in caries-free children, with a statistically significant difference (p<0.05).
Conclusion:
Parental perception of oral health-related quality of life was negatively affected by severe early childhood caries in children at a Perúvian health institute.
Keywords: dental caries; quality of life; pediatric dentistry; child; preschool
Objetivo:
Evaluar la percepción parental sobre la calidad de vida relacionada a la salud bucal en niños con caries de infancia temprana severa de un instituto de salud Perúano.
Método:
Se realizó un estudio observacional, analítico y transversal, en 200 niños de 3 a 5 años de edad, sin caries y con caries de infancia temprana severa (CIT-S) escogidos aleatoriamente. El instrumento aplicado por un encuestador calibrado fue la versión Perúana del cuestionario ECOHIS (P-ECOHIS) y el índice ceo-s. La distribución normal fue determinada con Kolmogorov - Smirnov, también se aplicó la prueba estadística U de Mann-Whitney.
Resultados:
El puntaje total del ECOHIS es mayor en los niños con CIT-S comparado con los niños sin caries, con una diferencia estadísticamente significativa (p<0.05).
Conclusión:
La percepción parental sobre la calidad de vida relacionada a la salud bucal fue negativamente afectada por la caries de infancia temprana severa de los niños de un instituto de salud Perúano.
Palabras claves: Caries dental; calidad de vida; odontología pediátrica; niño; preescolar.
Objetivo:
Avaliar a percepção dos pais sobre a qualidade de vida relacionada à saúde bucal em crianças com cárie grave na primeira infância de um instituto de saúde Perúano.
Método:
Foi realizado um estudo observacional, analítico e transversal em 200 crianças de 3 a 5 anos de idade, sem cárie e com cárie precoce da infância severa (CIT-S). O instrumento aplicado por um pesquisador calibrado foi a versão Perúana do questionário ECOHIS (P-ECOHIS) e o índice ceo-s. A distribuição normal foi determinada com Kolmogorov - Smirnov, o teste estatístico Mann-Whitney U também foi aplicado.
Resultados:
O escore total do ECOHIS é maior em crianças com CIT-S em comparação com crianças sem cárie, com diferença estatisticamente significante (p <0,05).
Conclusão:
A percepção dos pais sobre a qualidade de vida relacionada à saúde bucal foi afetada negativamente por cáries graves na primeira infância em crianças de um instituto de saúde Perúano.
Palavras-chave: Cárie dentária; qualidade de vida; odontopediatría; criança; pré-escolar
Introduction and background
Oral health-related quality of life (OHRQL) is a multidimensional (functional, psychosocial, and economic) complex of interrelated domains1 that represents the patients’ subjective perspective on their symptoms and experiences2. It is a socio-dental indicator, defined as the extent to which oral conditions influence normal social functioning and lead to significant changes in daily activities such as inability to work or attend school, etc.(3 These indicators are considered to complement clinical indicators significantly4.
Severe early childhood caries (S-ECC) is defined as any sign of smooth-surface caries in a child younger than three years of age. From ages 3 through 5, it typically has one or more cavitated, missing (due to caries), or filled smooth surfaces in primary maxillary anterior teeth or a dmfs index ≥4 (age 3), ≥5 (age 4), or ≥6 (age 5) 5. The etiology is complex and multifactorial, as in early childhood caries (ECC) 6.
ECC prevalence is 21% to 41.2% 7-9 in different parts of the world. ECC prevalence in Perú has already been studied10, but S-ECC prevalence in Perúvian children is unknown. It must be studied because children with S-ECC are at high risk of permanent tooth decay11 and other clinical consequences, which can be prevented if detected in time.
The link between dental caries and parental perception of OHRQL has already been studied internationally12-13, in Latin America14-15, and Perú16. It was found that dental caries reduces the quality of life. It impacts the child as it causes pain, infections, increased risk of hospitalization due to complications; it impacts parents because of high treatment costs, sleepless nights, lost work days, and distress17. This connection strengthens as the disease becomes more severe 18, and few studies analyze this connection in children with S ECC19.
In Perú, dental caries is the disease that most affects children’s oral health. Its prevalence is 59.1% in deciduous teeth and 85.6% in mixed dentition20. Children are at greater risk of tooth decay because Perúvian public health policies have not prioritized oral health10. It is vital to work with them more comprehensively, combining the social and clinical components, evaluating the quality of life, and addressing the issue as a whole to improve the likelihood of preventing tooth decay effectively. This study evaluates the parental perception of oral health-related quality of life in children with severe early childhood caries at a Perúvian health institute.
Materials and methods
Study population
The study was observational, analytical, and cross-sectional. It was conducted at Instituto Nacional de Salud del Niño (National Institute of Children’s Health - INSN), located in Lima, Perú. This institute specializes in health care for children and adolescents. It is the first pediatric institution of reference nationwide. Most users are from the capital (83.24%), including the urban population (75%). The children that seek the care services the most are under nine years of age, and only 49% are subsidized by free public insurance21.
Calibration of examiners
The calibration was performed in two stages: the theoretical stage involved discussing the dmfs index criteria by analyzing 30 photographs taken by a pediatric dentistry specialist (gold standard). The clinical stage was conducted at a preschool by performing the clinical examination of 30 children, aged 3 to 5, randomly chosen by the gold standard. The children were evaluated twice at a seven-day interval. Good intra- and inter-examiner reliability were determined (Cohen’s Kappa = 0.8 and 0.9). A pilot study was then conducted to assess the caregivers’ understanding of the ECOHIS questionnaire; everything was clear. The children from the pilot study and the calibration process were not included in the main sample.
Sample selection
The sample size was determined by convenience and randomly (every third child from the attendees’ list). It included 200 children (100 caries free and 100 with S-ECC), aged three to five, and treated at the pediatric dentistry department, accompanied by their caregiver, in October 2019. They were invited to participate in the study as per these inclusion criteria: the caregiver must be their father or mother, the child must not suffer from any systemic disease, and must have their dental clinical history in the institute.
Collection of non-clinical data
Structured interviews were conducted in the waiting room of the institute. The demographic data of the children and their caregivers were collected, as well as information on whether they had health insurance.
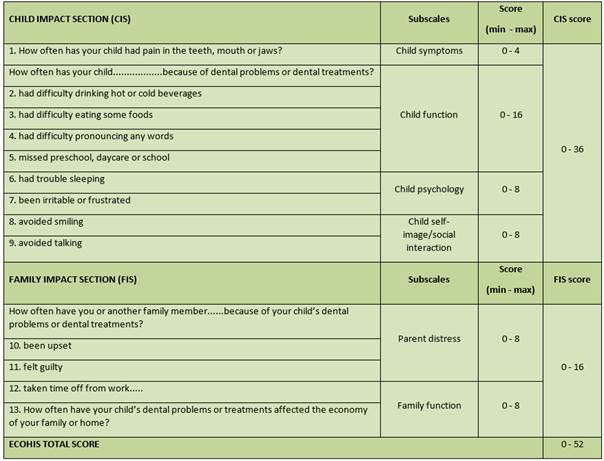
The instrument applied was the Perúvian version of the Early Childhood Oral Health Impact Scale (P-ECOHIS) validated by López Ramos et al. 22 This scale assesses the impact or influence of oral health problems related to the quality of life on children aged three to five, taking parental perception as a reference23. It includes 13 questions (items) divided into two main parts: the child impact section (first part) and the family impact section (second part). The child impact section (CIS) includes four subscales: child symptoms, child function, child psychology, and child self-image and social interaction. The family impact section (FIS) includes two subscales: parental distress and family function. The questionnaire includes a Likert scale of five responses ranging from “never” to “very often” (equivalent to a score of 0 to 4) 24. These responses record how often an event occurred during the child’s life. Each subscale element was classified as having no impact (0 or 1) and impacting (2-4). “Never” and “hardly ever” were considered to have no impact on the OHRQL, and “occasionally,” “often” and “very often” to have an impact25. The sixth response (“I don’t know”) was not considered in the study.
The total score ranges from 0 to 52 calculated as the addition of the answers. A higher score reflects a worse parental perception about OHRQL, an adverse effect or influence 23 Sections and scores are summarized in table 1. This stage lasted approximately ten minutes.
Collection of clinical data
Immediately after the interview, clinical data were collected. Patients were examined using an oral mirror, a WHO-recommended periodontal probe (Hu Friedy® PCP 11.5B), and artificial light. The dmfs index was used to distinguish caries-free children (dmfs = 0) from those with S-ECC (dmfs≥4, in children aged 3; dmfs≥5, in children aged 4, and dmfs≥6, in children aged 5). Cavitated carious lesions were considered caries, regardless of location. If the child had bacterial plaque or food debris, the caregiver was instructed to wash the child’s teeth before the evaluation. This stage lasted approximately five minutes.
Statistical analysis
The collected data were organized in an Excel spreadsheet (Microsoft Excel 2010). R package version 3.6.1 was used (R Core Development Team, 2019). The caries-free and S ECC samples were analyzed using a descriptive statistical method and a frequency distribution of ECOHIS demographics, components, subscales, and items. The caregiver’s age was cut-off at the median. Normal distribution was determined with the Kolmogorov-Smirnov test. As no normal distribution was found, a non parametric test was applied. The Mann Whitney U statistical test with a 95% confidence level determined the statistical difference between the two samples regarding the ECOHIS subscales and the total score (Table 1).
Results
The mean age of children and caregivers in the caries-free and S-ECC samples was 4.39 ± 0.85; 32.83 ± 6.82 and 4.1 ± 0.72; 31.4 ± 5.81, respectively. Most participants with S-ECC were male (55%), and they were mostly accompanied by their mothers (89%). Of the children, 65% had health insurance. The mean dmfs values in children aged 3, 4, and 5 were 6.4 ± 2.79, 7.12 ± 3.48, and 9.05 ± 3.56. Table 2 shows the demographic data of caries-free children.
Table 3 shows how the child and family sections of caries-free children had a higher frequency of “never” and “hardly never” responses. These children obtained 98%, 99%, and 100%, in the child’s section, as the “never” response in the items “difficulty pronouncing words,” “has avoided smiling,” “has avoided talking,” “difficulty drinking” and “felt upset or frustrated.” In the family section, they have low scores in the “never” response for items “has been upset or worried,” “has felt guilty,” and “has taken time off of work.” Additionally, caries-free children scored 0 in the “often” response for all the child’s section items.
Table 4 shows that the total ECOHIS score was higher in children with S-ECC compared to caries-free children. The family section had the highest values, with the items “has been upset or worried,” “has felt guilty” and “has taken time off from work” being the most impacted. The items least impacted by S-ECC were “avoided smiling” and “avoided talking,” with 7% and 6%respectively.
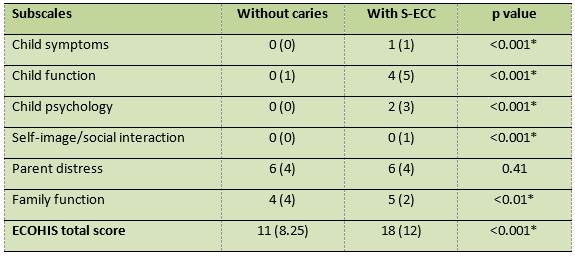
Table 5 shows the statistically significant difference (p<0.05) between the subscales’ impact and the total ECOHIS score among caries-free children and children with S-ECC, except on the parent distress subscale.
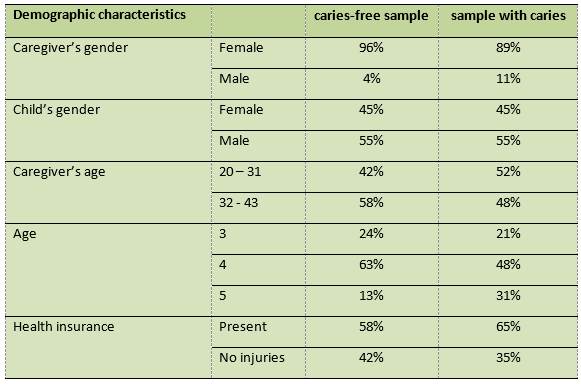
Table 3: Distribution of ECOHIS responses according to subscales and items in Perúvian children without caries and with S-ECC (n=200)
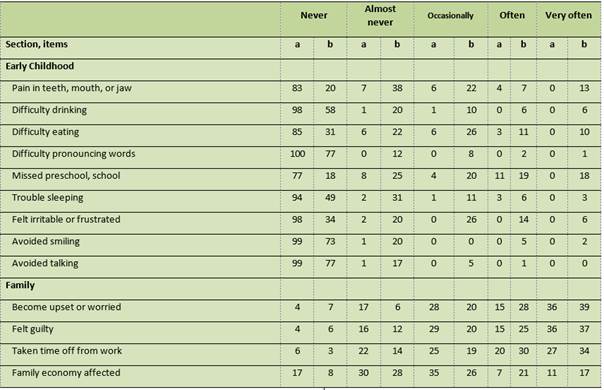
a= caries-free children, b= children with S-ECC (values in percentages)
Table 4: Distribution of ECOHIS scores according to child and family impact in Perúvian children without caries and with S-ECC (n=200)
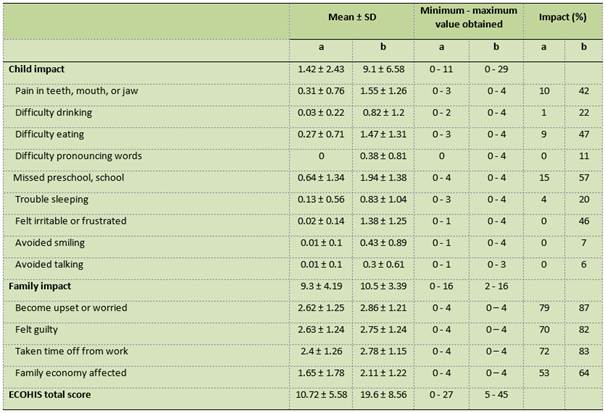
SD= standard deviation, a = caries-free children, b= children with S-ECC
Discussion
The main reason for caries prevention and treatment in primary dentition is to avoid pain and infection, as this has a considerable impact on children’s psychosocial well-being and can affect their daily activities26. Children’s health affects all family members economically and emotionally, making dental caries a family and social problem. Moreover, Perú is one of the countries with the highest prevalence of untreated caries in the region10, so this is a national public health problem.
Early childhood caries (ECC) has negatively impacted parental perception on the OHRQL of children and their parents/caregivers27-30. In contrast, in the study published by Ramos Jorge et al.(31, 52.8% of parents/caregivers consider that caries does not impact the quality of life, where 60.6% of children have severe caries. In this study, caregivers reported that S ECC negatively impacted the parental perception of OHRQL (all ECOHIS items have high percentages except for “avoided smiling” and “avoided talking”). A similar result was found in Asia19,6. It follows that the S-ECC has the most significant impact on children and families. Still, most of the research we consulted on caries in preschoolers focuses on ECC, which is one of the limitations of this study.
The mean ECOHIS score for children with S-ECC was 19.6 ± 8.56, which was higher compared to caries-free children, a result that matches what Lai et al. found19 (14.3 ± 7.9). These values are close, although the compared populations belong to different continents. It should be noted that the ECC scores are lower (9.21; 3.1 ± 5.1; 2.95) according to Abanto et al. 32, Li MY et al.33 and Martins-Junior et al.(30, respectively, compared to those obtained in this study. It is essential to determine the total ECOHIS score since the higher the score, the more affected the OHRQL. In this study, both ECOHIS components are affected by S-ECC; the family component is affected the most, a similar result to that found by Lai et al., 19 as opposed to Scarpelli et al.(27, Gomes et al.(29, and Martins-Júnior et al.(30, where the child component is the most impacted by ECC.
The most notable feature of the child’s component is the missed school days (57%), a topic studied by Ruff et al.(34),who showed that children with unmet dental needs might be absent longer because they have to go to the dentist for treatment. Also, pain makes it difficult for them to attend classes, which affects their school performance. Issues related to pain and difficulty eating have been reported more frequently27,30, although over half the parents in this study responded that it did not impact parental perception on OHRQL. Even so, the pain caused by ECC could affect nutrition since several studies have found that, for each unit of increase in the frequency of dental pain, children are more likely to be underweight35, which is linked to malnutrition36.
Regarding the family component, the results are similar to those of Lai et al.(19; the parents’ guilt is evident (82%), as previously studied by Carvalho et al.(37-38, and Gomes et al.(39 These researchers found that one third of parents feel guilty, leading to a decrease in the parental perception of OHRQL of families. This is associated with the perception that the child has tooth problems and that this could have been avoided. The parent distress subscale showed no difference in scores for children with S-ECC and caries-free children; the scores on this subscale are higher than those published by Li et al. in 201533.
Another important item in the family component is the time spent by parents accompanying their children to dental appointments (83%), studied by Ribeiro et al.(40 as missing work days. These researchers conclude that it is associated with dental pain, which affects family function. Regarding the economy (64%), Ribeiro et al.(41 state that parents had financial difficulties when they sought treatment too late, mainly due to the presence of pain and clinical complications.
All the negative effects on OHRQL for S-ECC compared to caries-free children found in this study should be taken into account to implement better public policies focusing on measures to prevent the appearance of caries. This would strengthen primary health care strategies in the first level of care and establish them as a priority within Perúvian public health measures. The current ones have not been effective, so far, in controlling the disease. It is recommended that future research on the subject include a larger sample so that the results can be extrapolated to the general population.
Conclusion
The parental perception of oral health-related quality of life in children was negatively affected by severe early childhood caries among children treated at a Perúvian health institute.
Referencias
1. Gift HC, Atchison KA, Dayton CM. Conceptualizing oral health and oral health-related quality of life. Soc Sci Med. 1997; 44 (5): 601-608. [ Links ]
2. Sischo L, Broder HL. Oral health-related quality of life: what, why, how, and future implications. J Dent Res. 2011; 90 (11): 1264-1270. [ Links ]
3. Locker D, Allen PF. Developing short-form measures of oral health-related quality of life. J Public Health Dent. 2002 Winter; 62 (1): 13-20. [ Links ]
4. Maizels J, Maizels A, Sheiham A. Dental disease and health behaviour: the development of an interactional model. Community Dent Health. 1991; 8 (4): 311-21. [ Links ]
5. AAPD. Definition of early childhood caries (ECC): Classifications, consequences, and preventive strategies. Pediatr Dent Ref Man, 2012-13; 34:12-3. [ Links ]
6. Mansoori S, Mehta A, Ansari MI. Factors associated with Oral Health Related Quality of Life of children with severe -Early Childhood Caries. J Oral Biol Craniofac Res. 2019; 9 (3): 222-225. [ Links ]
7. Li Y, Wulaerhan J, Liu Y, Abudureyimu A, Zhao J. Prevalence of severe early childhood caries and associated socioeconomic and behavioral factors in Xinjiang, China: a cross-sectional study. BMC Oral Health. 2017; 17 (1): 144. [ Links ]
8. G Mangla R, Kapur R, Dhindsa A, Madan M. Prevalence and associated Risk Factors of Severe Early Childhood Caries in 12- to 36-month-old Children of Sirmaur District, Himachal Pradesh, India. Int J Clin Pediatr Dent. 2017; 10 (2):183-187. [ Links ]
9. Schroth RJ, Halchuk S, Star L. Prevalence and risk factors of caregiver reported Severe Early Childhood Caries in Manitoba First Nations children: results from the RHS Phase 2 (2008-2010). Int J Circumpolar Health. 2013; 72. [ Links ]
10. Castillo JL, Palma C, Cabrera-Matta A. Early Childhood Caries in Perú. Front Public Health. 2019; 7: 337. [ Links ]
11. Xie YY, Cheng ML, Xu MR, Si Y, Xu T. Cost-effectiveness Analysis of Comprehensive Oral Health Care for Severe Early Childhood Caries in Urban Beijing, China. Chin J Dent Res. 2019; 22 (1):45-50. [ Links ]
12. Duangthip D, Gao SS, Chen KJ, Lo ECM, Chu CH. Oral health-related quality of life and caries experience of Hong Kong preschool children. Int Dent J. 2019; 70 (2): 100-107 [ Links ]
13. Sakaryali D, Bani M, Cinar C, Alacam A. Evaluation of the impact of early childhood caries, traumatic dental injury, and malocclusion on oral health-Related quality of life for Turkish preschool children and families. Niger J Clin Pract. 2019;22 (6):817-823. [ Links ]
14. Nóbrega AVD, Moura LFAD, Andrade NS, Lima CCB, Dourado DG, Lima MDM. Impact of dental caries on the quality of life of preschoolers measured by PedsQL questionnaire. Cien Saude Colet. 2019; 24 (11): 4031-4042. [ Links ]
15. Díaz S, Mondol M, Peñate A, Puerta G, Boneckér M, Martins Paiva S, et al. Parental perceptions of impact of oral disorders on Colombian preschoolers' oral health-related quality of life. Acta Odontol Latinoam. 2018; 31 (1): 23-31. [ Links ]
16. Pesaressi E, Villena RS, Frencken JE. Dental caries and oral health-related quality of life of 3-year-olds living in Lima, Perú. Int J Paediatr Dent. 2020; 30 (1): 57-65. [ Links ]
17. BaniHani A, Deery C, Toumba J, Munyombwe T, Duggal M. The impact of dental caries and its treatment by conventional or biological approaches on the oral health-related quality of life of children and carers. Int J Paediatr Dent. 2018; 28 (2): 266-276. [ Links ]
18. Nora ÂD, da Silva Rodrigues C, de Oliveira Rocha R, Soares FZM, Minatel Braga M, Lenzi TL. Is Caries Associated with Negative Impact on Oral Health-Related Quality of Life of Pre-school Children? A Systematic Review and Meta-Analysis. Pediatr Dent. 2018; 40 (7): 403-411. [ Links ]
19. Lai SHF, Wong MLW, Wong HM, McGrath CPJ, Yiu CKY. Factors influencing the oral health-related quality of life among children with severe early childhood caries in Hong Kong. Int J Dent Hyg. 2019; 17 (4):350-358. [ Links ]
20. Perú.Ministerio de salud [Internet]. Guía de práctica clínica para la prevención, diagnóstico y tratamiento de la caries dental en niñas y niños: Guía técnica ,citado el 14 de noviembre del 2019. Disponible en: http://bvs.minsa.gob.pe/local/MINSA/4195.pdf. [ Links ]
21. Perú. Instituto Nacional de Salud del Niño. Análisis Situacional de los Servicios de Salud del Instituto Nacional de salud del Niño - 2018 citado el 20 de diciembre del 2019. Disponible en: Disponible en: http://www.insn.gob.pe/publica-ciones/asis [ Links ]
22. López Ramos RP, García Rupaya CR, Villena-Sarmiento R, Bordoni NE. Cross cultural adaptation and validation of the Early Childhood Health Impact Scale (ECOHIS) in Perúvian preschoolers. Acta Odontol Latinoam. 2013; 26 (2): 60-7. [ Links ]
23. Pahel BT, Rozier RG, Slade GD.Parental perceptions of children's oral health: the Early Childhood Oral Health Impact Scale (ECOHIS). Health Qual Life Outcomes. 2007; 5:6. [ Links ]
24. Martins-Júnior PA, Ramos-Jorge J, Paiva SM, Marques LS, Ramos-Jorge ML. Validations of the Brazilian version of the Early Childhood Oral Health Impact Scale (ECOHIS). Cad Saude Pública. 2012;28 (2): 367-74. [ Links ]
25. Arrow P, Klobas E. Evaluation of the Early Childhood Oral Health Impact Scale in an Australian preschool child population. Aust Dent J. 2015; 60 (3): 375-81. [ Links ]
26. Ferraz NK, Nogueira LC, Pinheiro ML, Marques LS, Ramos-Jorge ML, Ramos-Jorge J. Clinical consequences of untreated dental caries and toothache in preschool children. Pediatr Dent. 2014; 36 (5): 389-92. [ Links ]
27. Scarpelli AC, Paiva SM, Viegas CM, Carvalho AC, Ferreira FM, Pordeus IA. Oral health-related quality of life among Brazilian preschool children. Community Dent Oral Epidemiol. 2013; 41(4): 336-44. [ Links ]
28. Abanto J, Paiva SM, Raggio DP, Celiberti P, Aldrigui JM, Bönecker M. The impact of dental caries and trauma in children on family quality of life. Community Dent Oral Epidemiol. 2012; 40 (4): 323-31. [ Links ]
29. Gomes MC, Pinto-Sarmento TC, Costa EM, Martins CC, Granville-Garcia AF, Paiva SM. Impact of oral health conditions on the quality of life of preschool children and their families: a cross-sectional study. Health Qual Life Outcomes. 2014; 12:55. [ Links ]
30. Martins-Júnior PA, Vieira-Andrade RG, Corrêa-Faria P, Oliveira-Ferreira F, Marques LS, Ramos-Jorge ML. Impact of early childhood caries on the oral health-related quality of life of preschool children and their parents. Caries Res. 2013; 47 (3): 211-8. [ Links ]
31. Ramos-Jorge J, Pordeus IA, Ramos-Jorge ML, Marques LS, Paiva SM. Impact of untreated dental caries on quality of life of preschool children: different stages and activity. Community Dent Oral Epidemiol. 2014; 42 (4): 311-22. [ Links ]
32. Abanto J, Carvalho TS, Mendes FM, Wanderley MT, Bönecker M, Raggio DP. Impact of oral diseases and disorders on oral health-related quality of life of preschool children. Community Dent Oral Epidemiol. 2011; 39 (2): 105-114. [ Links ]
33. Li MY, Zhi QH, Zhou Y, Qiu RM, Lin HC. Impact of early childhood caries on oral health-related quality of life of preschool children. Eur J Paediatr Dent. 2015; 16 (1): 65-72. [ Links ]
34. Ruff RR, Senthi S, Susser SR, Tsutsui A. Oral health, academic performance, and school absenteeism in children and adolescents: A systematic review and meta-analysis. J Am Dent Assoc. 2019; 150 (2): 111-121. [ Links ]
35. So M, Ellenikiotis YA, Husby HM, Paz CL, Seymour B, Sokal-Gutierrez K. Early Childhood Dental Caries, Mouth Pain, and Malnutrition in the Ecuadorian Amazon Region. Int J Environ Res Public Health. 2017; 14 (5). [ Links ]
36. Janakiram C, Antony B, Joseph J. Association of Undernutrition and Early Childhood Dental Caries. Indian Pediatr. 2018; 55 (8): 683-685. [ Links ]
37. Carvalho TS, Abanto J, Pinheiro ECM, Lussi A, Bönecker M. Early childhood caries and psychological perceptions on child's oral health increase the feeling of guilt in parents: an epidemiological survey. Int J Paediatr Dent. 2018; 28 (1): 23-32. [ Links ]
38. Carvalho TS, Abanto J, Mendes FM, Raggio DP, Bonecker M. Association between parental guilt and oral health problems in preschool children. Braz Oral Res 2012; 26: 557-563. [ Links ]
39. Gomes MC, Clementino MA, Pinto-Sarmento TC, Martins CC, Granville-Garcia AF, Paiva SM. Association between parental guilt and oral health problems in preschool children: a hierarchical approach. BMC Public Health 2014; 14: 854. [ Links ]
40. Ribeiro GL, Gomes MC, de Lima KC, Martins CC, Paiva SM, Granville-Garcia AF. Work absenteeism by parents because of oral conditions in preschool children. Int Dent J. 2015;65 (6): 331-7. [ Links ]
41. Ribeiro GL, Gomes MC, de Lima KC, Martins CC, Paiva SM, Granville-Garcia AF. The potential financial impact of oral health problems in the families of preschool children. Cien Saude Colet. 2016;21 (4): 1217-26. [ Links ]
Received: April 06, 2020; Accepted: June 12, 2020
 Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
