










Serviços Personalizados
Journal

Artigo
 texto em
texto em  Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
Links relacionados
Compartilhar

 Permalink
PermalinkOdontoestomatología
versão impressa ISSN 0797-0374versão On-line ISSN 1688-9339
Odontoestomatología vol.22 no.35 Montevideo 2020 Epub 01-Jun-2020
https://doi.org/10.22592/ode2020n35a6
Research
In vitro study of the relationship between bond strength to dental enamel and microleakage in photopolymerizable composite resins
1
 http://orcid.org/0000-0002-3780-1034
http://orcid.org/0000-0002-3780-1034
2
http://orcid.org/0000-0002-1561-2283
3
http://orcid.org/0000-0002-2759-8984
1Cátedra de Materiales Dentales, Facultad de Odontología, Universidad de la República, Uruguay
2Cátedra de Materiales Dentales, Facultad de Odontología, Universidad de la República, Uruguay. matiasmederos@odon.edu.uy
3Laboratorio de Materiales Dentales. Área Académica de Odontología, Universidad Autónoma del Estado de Hidalgo, México
4Cátedra de Operatoria Dental II, Facultad de Odontología, Universidad de la Republica, Uruguay
5Cátedra de Materiales Dentales, Facultad de Odontología, Universidad de la Republica, Uruguay
Objectives:
To evaluate and compare the relationship between enamel bond strength and microleakage of two composite based restorative systems.
Methods:
40 third molars were randomly divided into two groups: 20 molars restored with the Adper Single bond 2 + Filtek Z250 XT (3M ESPE; ST PAUL, MN, USA) system and 20 with the Tetric N Bond + Tetric N Ceram (Ivoclar Vivadent; Schaan, Liechtenstein) system. Half of the teeth in each group were used for a bond strength test, while the other half were used for the microleakage test.
Results:
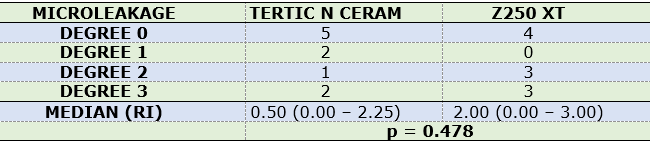
The means and standard deviation of the bond strength resistance were 27.93 (± 9.55) MPa for Adper Single bond 2 + Filtek Z250 XT system and 33.12 (± 8.18) MPa for Tetric N Bond + Tetric N Ceram system (p = 0.049). Regarding the microleakage values, there were no statistically significant differences between the groups (p = 0.478). No significant correlation was observed between Microtensile bond strength and microleakage (R2 = 0.0909, p = 0.196).
Conclusions:
It was not found a relationship between adhesive bond values and the degree of microleakage.
Key words: Bond strength; Microleakage; Composite Resins
Objetivos:
Evaluar y comparar la relación entre la resistencia de unión inmediata a esmalte y microfiltración de dos sistemas restauradores a base de resina compuesta.
Métodos:
40 terceros molares se dividieron aleatoriamente en dos grupos: 20 molares restaurados utilizando el sistema Adper Single bond 2 + Filtek Z250 XT (3M ESPE; ST PAUL, MN, USA); y 20 molares restaurados con el sistema Tetric N Bond + Tetric N Ceram (Ivoclar Vivadent; Schaan, Liechtenstein). La mitad de los dientes de cada grupo se utilizaron para un ensayo de microtracción, mientras que la otra mitad fueron utilizados para un ensayo de microfiltración (n = 10).
Resultados: Las medias y el desvío padrón de la resistencia de unión a microtracción fueron de 27.93 (±9.55) para Adper Single bond 2 + Filtek Z250 XT MPa y 33.12 (±8.18) MPa para Tetric N Bond + Tetric N Ceram (p = 0,049). En cuanto a los valores de microfiltración, no hubo diferencias estadísticamente significativas entre los grupos (p = 0,478). No fue observada una correlación significativa entre la resistencia de unión a la microtracción y la microfiltración (R2= 0.0909; p = 0.196).
Conclusiones:
No se encontró una relación entre los valores de resistencia de unión y el grado de microtracción.
Palabras claves: Microtracción; Microfiltración; Resinas Compuestas
Objetivos:
Avaliar e comparar a relação entre a resistência de união imediata ao esmalte e a microfiltração de dois sistemas restauradores baseados em resina composta.
Métodos:
40 terceiros molares foram divididos aleatoriamente em dois grupos: 20 molares restaurados usando o sistema Adper Single bond 2 + Filtek Z250 XT (3M ESPE; ST PAUL, MN, EUA); e 20 molares restaurados com o sistema Tetric N Bond + Tetric N Ceram (Ivoclar Vivadent; Schaan, Liechtenstein). Metade dos dentes de cada grupo foi utilizada para um teste de resistência de união à microtração, enquanto a outra metade foi utilizada para um teste de microfiltração (n = 10).
Resultados:
As mídias e o padrão de resistência de união à microtração foram 27,93 (± 9,55) para Adper Single bond 2 + Filtek Z250 XT MPa e 33,12 (± 8,18) MPa
para Tetric N Bond + Tetric N Ceram (p = 0,049). Em relação aos valores de microfiltração, não houve diferença estatisticamente significativas entre os grupos (p = 0,478). Não houve correlação significativa observada entre a resistência de união à microtração e a microfiltração (R2= 0,0909; p = 0,196).
Conclusões:
Não foi encontrada relação entre os valores de resistência de união e o grau de microfiltração.
Palavras-chave: microtração; microfiltração; resinas compostas
Introduction
Since their introduction in the 1960s, composite resins have been increasingly used. Currently, they are considered materials for universal use and are the first option for direct restorations in anterior and posterior teeth1. The aesthetic characteristics they provide, matching the natural tooth color, their ability to adhere to the hard tissues through micromechanical retention adhesive systems, and their low cost compared to indirect restorative materials are some of the reasons that justify their use2.
However, a large number failures are still reported for this type of restoration in the short and medium term2. This is related to problems regarding the changes the resin undergoes once polymerized (polymerization contraction, thermal expansion coefficient), and regarding the oral cavity (superficial abrasion, chemical degradation, etc.)3-4. These problems explain restoration failures, with failures in the tooth-restoration interface, microleakage and subsequent caries recurrence5-8.
To counteract these problems, manufacturers have modified resin composition, for example, monomers with higher molecular weight (producing less polymerization shrinkage), or improving inorganic charge particles (higher load, smaller size and different morphologies), which has led to significant improvements in material properties9-10.
Using accelerated aging techniques under standardized laboratory conditions is an effective alternative to study long-term restorative material behavior, as it is possible to simulate the clinical use of a material in a short period. Some methods have been proposed to this end, including immersion in water, ethanol or artificial saliva, as well as thermal cycling and UV aging11.
Thermal cycling involves subjecting samples to extreme temperatures to simulate intraoral changing temperature conditions12. The effect of thermal cycling induces the degradation of the tooth/restoration interface because of the difference in the thermal expansion coefficient13. This methodology is proposed by the International Organization for Standardization in its ISO 11405 standard as a method to accelerate material aging, simulating its survival in the mouth14.
The simplicity and effectiveness of the enamel adhesion process is well known15. Of the available adhesive strategies, the three-step etch-and-rinse techniques and the two-step self-etch techniques are considered as the gold standard16-17. However, the two-step etch-and-rinse technique is the most widely used one in our country, also yielding satisfactory results18-19.
Objective
To evaluate and compare the relationship between immediate enamel bond strength and the microleakage of two composite resin-based restorative systems through microtensile and microleakage tests.
The hypothesis raised is that the greater the bond strength value, the lower degree of microleakage.
Materials and methods
Obtaining samples
The sample included 40 third molars with a healthy crown regardless of root development status. They were obtained in the surgical block service of the School of Dentistry, having been removed for reasons unrelated to this research. The teeth were collected after the patients signed a written informed consent and upon approval of the project by the Ethics Committee of the School of Dentistry - UDELAR (File no. 215/14). Once extracted, the molars were cleaned with periodontal curettes and prophylaxis with pumice stone and water was implemented. They were then stored in 0.5% Chloramine-T for 7 days and subsequently in distilled water at 3°C to 5°C for no more than 3 months. This procedure is protocolized by the Human Tooth Bank of the School of Dentistry (File no. 091100-000933-11, Council of the School of Dentistry).
All restorations were made in the same batch and samples for each trial were randomly distributed (generated through www.randomizer.org) into two groups of twenty molars each, depending on the restorative system used:
-Group “Z”: 20 molars restored with Adper Single bond 2+ Filtek Z250 XT (3M SPEC; ST PAUL, MN, USA).
-Group “T”: 20 molars restored with Tetric N Bond + Tetric N Ceram (Ivoclar Vivadent; Schaan, Liechtenstein, Germany).
All the materials were handled in compliance with the manufacturer’s instructions. Both adhesive systems were applied after conditioning the enamel with 37% phosphoric acid for 15 seconds (Dentsply; Petropolis, RJ, Brazil). The same color (A2) was selected for both restorative systems to avoid having polymerization variables induced by pigments. Both composite resins have nanohybrid filler so this variable was also controlled to avoid biases. Table 1 includes information regarding composition, manufacturer's indications and batch.
Microtensile test
Half the teeth assigned to each group were used for the microtensile test (n=10). The buccal faces of the molars were worn down with sandpaper with 600 grit size by making eight-shaped movements to achieve a flat, smooth enamel surface. This surface was used to apply the adhesive treatment. It had been conditioned with 37% phosphoric acid for 15 seconds. After that time, the surface was washed vigorously with pressurized water for 15 seconds followed by pressurized air, drying in a direction oblique to the surface. The adhesive system was then applied according to the corresponding group and following the manufacturer’s instructions. The adhesive layer was light-cured with an Optilight Max halogen unit (Gnatus; Ribeirao Preto, Brazil) and previously analyzed with a Bluephase Meter radiometer (Ivoclar Vivadent; Schaan, Liechtenstein, Germany) at 980mw/cm2.
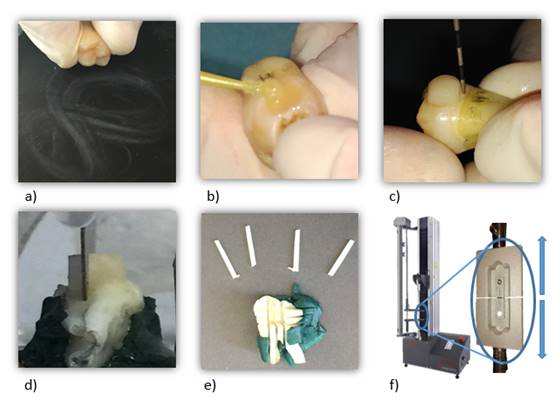
A 4 mm high and 5 mm wide resin block was then made on the buccal face, incrementally adding 2 mm layers and light-curing each increment according to the manufacturer’s instructions. The specimens were stored 24 hours in distilled water at 37oC to allow time for polymerization reactions to end and release the stresses induced by it. Then, using a Gellings-Hamco microtome (Hamco Machines INC.; Rochester, NY, USA) 1 mm2 specimens were sectioned (rods), which were half enamel and half composite resin (Fig. 1).
The microtensile test was performed using an MTS SANS CMT 2000 5KN universal testing machine (MTS Systems Corporation; Shanghai China) at a speed of 1mm/min and a 100 N charge cell.
Bond strength (MPa) was calculated using the following formula:
μTBS (MPa) = F(N)/A(mm 2 )
Where μTBS is the microtensile bond strength in MPa, F is the maximum force measured by the universal test machine in Newton, and A is the cross-sectional area of the specimen calculated according to width multiplied by depth.
The specimens were subjected to microtensile tests according to the ISO 11405 standard14. The failure mode was analyzed in each of the samples with a stereoscope (10x) and classified into failures:
Microleakage test
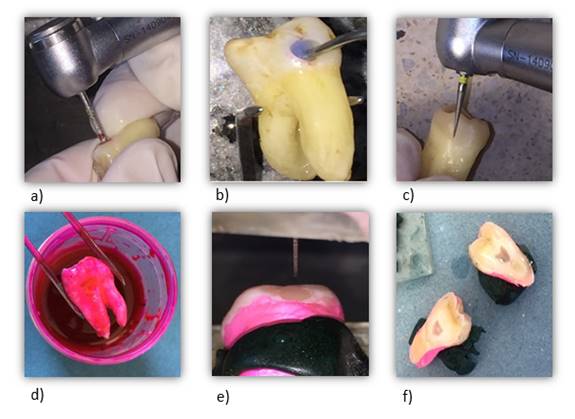
A total of 10 teeth per group were used (n=10) for the microleakage test. A cavity was made in enamel and dentin at the middle third of the buccal face using Kavo EXTRAtorque 505C high-speed rotary instruments with spray (Kavo Dental; Schwaben, Germany) and a 100-110 micron/1.6 mm diameter medium-grain diamond cylindrical bur (Microdont Dental Products; Monsei, NY, USA). We obtained a dentin cavity measuring 3 mm in diameter and 1 mm deep. The bur was changed every three cavities. The cavities were standardized using an American Eagle periodontal probe (American Eagle Instruments Inc.; Missoula, Montana, USA), and if the measurements were not the same, the specimen was discarded. The adhesive treatment of the corresponding group was implemented following the manufacturer’s instructions. The composite resin was placed by adding consecutive 2 mm thick layers until the entire cavity was filled. The adhesive and resin were light-cured with a GNATUS Optilight Max unit. Once completed, the restoration was finished with a 30 micron/0.16 diameter extra-fine diamond stone (Microdont Dental Products; Monsei, NY, USA) and polished with medium and extra-fine grain discs (Microdont Dental Products; Monsei, NY, USA) until a smooth surface was obtained. The restored specimens were stored for 24 hours in distilled water at 37oC. Finally, the samples were sealed with transparent Colorama synthetic polish (L’Oréal Brasil; São Paulo, Brazil), applying two layers that covered the root up to the cementoenamel junction (except 1 mm around the cavo surface angle) in order to avoid possible root or apical filtrations.
For the microleakage test, the samples were subjected to 500 thermal cycles in a thermal cycler (Termocycle; Biopdi, São Paulo, Brazil) at between 5°and 55° C, each bath lasting 20 seconds, with intervals between baths of 10 seconds, following the ISO/TS 11405 standard14. According to some studies, 500 cycles are sufficient to observe a microleakage effect on the interface, and the increase in the number of cycles is not associated with increased microleakage20-21. Finally, the samples were immersed in basic fuchsin in 0.5% propylene glycol solution for 24 hours, following previously established protocols22-23, and sagittally cut with a Gellings-Hamco microtome (Hamco Machines INC.; Rochester, NY, USA) to be evaluated (Fig. 2).
The samples were analyzed with a ROSSBACH YZ-6 stereoscope (Rossbach de Mexico; Mexico City, Mexico), and classified according to the degree of dye penetration:
0 - No dye penetration
1 - Dye penetrated the enamel walls
2 - Dye penetrated the walls, reaching the dentin
3 - Dye reached the floor of the cavity
All the observations were made by the same researcher (See Fig. 3).
Statistical analysis
Statistical analysis was performed using SigmaPlot Version 12.0. Data obtained about microtensile bond strength were analyzed using Student’s t-test. In addition, microleakage values were analyzed using the Mann-Whitney U (non-parametric) test. A Pearson correlation analysis was used to determine the degree of association of the dependent variables studied. A significance level of = 0.05 was chosen for all the analyses.
Results
Microtensile bond strength values are presented in Fig. 4. The results of this study showed a statistically significant difference between the groups (p = 0.049); Tetric N Ceram (Ivoclar Vivadent ®) had a higher bond strength value compared to Filtek Z250XT (3M ESPE®).
Additionally, no statistically significant differences were found in the degree of microleakage (P=0.478) between the two restorative materials (Table 2).
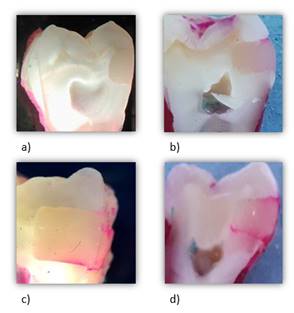
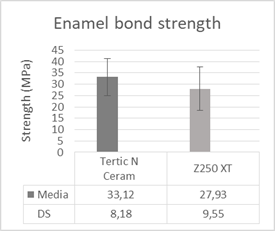
Fig. 4: Mean bond strength values and corresponding standard deviations (SD) obtained after the microtensile test
The correlation analysis showed no statistically significant correlation (p = 0.196) between microtensile bond strength and microleakage, and the correlation coefficient was 0.09.
Discussion
Based on the results of this study, it was not possible to accept our hypothesis, since statistically significant differences were found in the bond strength values (p = 0.049). This was not the case in the microleakage test, as both resins had a similar degree of microleakage (p = 0.478).
We know that adhesive dentistry aims to develop materials that can replace dental structure. Sealing capacity (nanoleakage and microleakage) and adhesive bond strength are two of the main types of laboratory tests used to evaluate the performance of restoration systems24.
Regarding bond strength, the data obtained in this study are consistent with the literature: between 28.57 and 29 MPa for Tetric N Bond25,26, and 24.8 to 29.7 MPa for Adper Single Bond 227.
It is important to mention that this study found no direct relationship between bond strength and microleakage, as have other works in the literature28-31.
We must also note that the aim of the microleakage test is not to determine material survival, because there is evidence in the literature that penetration tests to evaluate microleakage do not correlate with the clinical success parameters of the restoration (postoperative sensitivity, retention, marginal coloration)32. The aim of thermal cycling is to simulate the aging of the material while the microleakage test aims to analyze the failure mode of the adhesive interface33. This is why studies are still conducted aiming to predict the behavior of polymeric restoration systems using this type of test28-31.
Having discussed the results and after analyzing other scientific studies, we can conclude that bond strength is not the only determining factor when testing the performance of an adhesive system. In addition, multiple other variables inherent to the material must be considered (filler type and percentage, degree of volumetric contraction, hydrolytic stability, thermal expansion coefficient, etc.)34-35, the technique (stratified technique, monolayer, C factor, light-curing times and intensity, etc.) 35-36) the substrate (depth, tissues involved, type of dentition, smear layer removal, etc.)37, and the medium (pH variability, mechanical loads received, etc.)36,38-41.
Currently, we can say that restorative systems satisfactorily meet the requirements set out in the standards, achieving good clinical performance. This is why selecting a restorative system has become a minor problem today2,9. Additionally, the “operator factor”, which is rarely studied, is likely to play a major role throughout the longevity process42-44.
Therefore, it is essential that professionals know the material and its correct handling (respecting the established protocols) in order to create an effective and long-lasting bond with the tooth structure.
More studies considering these variables must be conducted in order to support our conclusions and consolidate the role of other factors in the performance of adhesive systems, such as long-term clinical trials, which can record real conditions more closely.
Conclusions
The restorative systems used were unable to prevent microleakage, although Tetric N Ceram obtained higher bond strength values.
No connection was found between bond strength values and degree of microleakage. Bond strength is not the only determining factor for predicting the performance of an adhesive system, so other multiple variables inherent to the material, substrate, technique, and environment should be taken into account.
Acknowledgments
This study was funded by the Student Research Support Program (PAIE) of the Sectoral Commission for Scientific Research (CSIC).
REFERENCES
1. Correa MB, Peres MA, Peres KG, Horta BL, Barros AD, Demarco FF. Amalgam or composite resin? Factors influencing the choice of restorative material. J Dent. 2012; [ Links ]
2. Demarco FF, Corrêa MB, Cenci MS, Moraes RR, Opdam NJM. Longevity of posterior composite restorations: not only a matter of materials. Dent Mater. 2012; 28 (1): 87-101. [ Links ]
3. Chang C-H, Fang C-L, Hsu J-T, Chen. Chang-Pen. Cavity Dimension Effect on MOD Dental Restoration Filled with Resin Composite - A Finite Element Interface Stress Evaluation. J Med Biol Eng. 2004; 24 (4). [ Links ]
4. Ishikiriama SK, De Oliveira GU, Maenosono RM, Wang L, Duarte MAH, Mondelli RFL. Wear and surface roughness of silorane composites after pH cycling and toothbrushing abrasion. Am J Dent. 2014; 27 (4): 195-8. [ Links ]
5. Mjör IA. Problems and benefits associated with restorative materials: side-effects and long-term cost. Adv Dent Res. 1992; 6 (1): 7-16. [ Links ]
6. Mjör IA, Jokstad A. Five-year study of Class II restorations in permanent teeth using amalgam, glass polyalkenoate (ionomer) cerment and resin-based composite materials. J Dent. 1993;21 (6): 338-43. [ Links ]
7. Mjör IA. The reasons for replacement and the age of failed restorations in general dental practice. Acta Odontol Scand. 1997;55 (1): 58-63. [ Links ]
8. Braga SRM, Vasconcelos BT, Macedo MR de P, Martins VRG, Sobral MAP. Reasons for placement and replacement of direct restorative materials in Brazil. Quintessence Int. 2007; 38 (4): e189-94. [ Links ]
9. Opdam NJ, van de Sande FH, Bronkhorst E, Cenci MS, Bottenberg P, Pallesen U, Gaengler P, Lindberg A, Huysmans MC, van Dijken JW. Longevity of Posterior Composite Restorations. J Dent Res. 2014; 93 (10): 943-9. [ Links ]
10. Matos AB, Trevelin LT, Silva BTF da, Francisconi-dos-rios LF, Siriani LK, CArdoso MV. Bonding efficiency and durability: current possibilities. Braz Oral Res. 2017; 31(suppl 1). [ Links ]
11. Hahnel S, Henrich A, Bürgers R, Handel G, Rosentritt M. Investigation of mechanical properties of modern dental composites after artificial aging for one year. Oper Dent. 2010; 35 (4): 412-9. [ Links ]
12. Amano S, Yamamoto A, Tsubota K, Rikuta A, Miyazaki M, Platt JA, Moore BK. Effect of Thermal Cycling on Enamel Bond Strength of Single-step Self-etch Systems. Oper Dent. 2006; 31(5): 616-22. [ Links ]
13. Rossomando KJ, Wendt SL. Thermocycling and dwell times in microleakage evaluation for bonded restorations. Dent Mater. 1995;11 (1): 47-51. [ Links ]
14. ISO/TS 11405:2015(en), Dentistry - Testing of adhesion to tooth structure. [ Links ]
15. Van Meerbeek B, De Munck J, Yoshida Y, Inoue S, Vargas M, Vijay P, Van Landuyt K, Lambrechts P, Vanherle G. Adhesion to enamel and dentin: current status and future challenges. Oper Dent. 2003; [ Links ]
16. Mahn E, Rousson V, Heintze S. Meta-Analysis of the Influence of Bonding Parameters on the Clinical Outcome of Tooth-colored Cervical Restorations. J Adhes Dent. 2015;17 (5): 391-403. [ Links ]
17. van Dijken JW V, Pallesen U. Long-term dentin retention of etch-and-rinse and self-etch adhesives and a resin-modified glass ionomer cement in non-carious cervical lesions. Dent Mater. 2008;24 (7): 915-22. [ Links ]
18. Perdigão J. New Developments in Dental Adhesion. Dent Clin North Am. 2007;51 (2): 333-57. [ Links ]
19. Cardoso MV, de Almeida Neves A, Mine A, Coutinho E, Van Landuyt K, De Munck J, Van Meerbeek B.Current aspects on bonding effectiveness and stability in adhesive dentistry. Aust Dent J. 2011;56 Suppl 1:31-44. [ Links ]
20. Wahab FK, Shaini FJ, Morgano SM. The effect of thermocycling on microleakage of several commercially available composite Class V restorations in vitro. J Prosthet Dent 2003; 90 (2): 168-74. Available from: http://www.ncbi.nlm.nih.gov/pubmed/12886210 [ Links ]
21. Pazinatto FB, Campos BB, Costa LC, Atta MT. Effect of the number of thermocycles on microleakage of resin composite restorations. Pesqui Odontol Bras. 2003; 17 (4): 337-41. [ Links ]
22. Güçlü ZA, Dönmez N, Hurt AP, Coleman NJ. Characterisation and microleakage of a new hydrophilic fissure sealant-ultraseal XT(r)hydroTM. J Appl Oral Sci. 2016;24 (4): 344-51. [ Links ]
23. Okida RC, Martins TM, Briso ALF. In vitro evaluation of marginal leakage in bonded restorations, with mechanical or chemical-mechanical (Carisolv) removal of carious tissue. Braz Oral Res. 2007; 21 (2): 176-81. [ Links ]
24. Bedran-de-Castro AKB, Pereira PNR, Pimenta LAF, Thompson JY. Effect of thermal and mechanical load cycling on microtensile bond strength of a total-etch adhesive system. Oper Dent 2004; 29 (2): 150-6 [ Links ]
25. Shadman N, Farzin Ebrahimi S, Abrishami A, Sattari H. Shear bond strength of three adhesive systems to enamel and dentin of permanent teeth. J Dent Med. 2012; 25 (3): 202-10. [ Links ]
26. Ivoclar-Vivadent. Tetric(r) N-Collection Un completo sistema restaurativo nano-optimizado. [ Links ]
27. De Nordenflycht D, Kaplan M, Montecinos V, Báez A. Resistencia microtraccional de capa de adhesivo contaminada con sangre. Rev Clínica Periodoncia, Implantol y Rehabil Oral. 2013; 6 (3): 118-22. [ Links ]
28. Ateyah NZ, Elhejazi AA. Shear bond strengths and microleakage of four types of dentin adhesive materials. J Contemp Dent Pract. 2004; 5 (1): 63-73. [ Links ]
29. Fortin D, Swift EJ, Denehy GE, Reinhardt JW. Bond strength and microleakage of current dentin adhesives. Dent Mater. 1994;10 (4): 253-8. [ Links ]
30. Abdelrahman M, Abdelrahman MH, Mahmoud EM, Ghoneim MM, Kammar AA. Comparative study of microleakage and shear bond strength between bulk fill and self adhesive flowable composite resins. Alexandria Dent J. 2016; 41 (3): 322-7. [ Links ]
31. Chowdary Mandava R, Gurunathan D, Ramakrishnan M, Subramanian E. Comparison of Microleakage and Shear Bond Strength (SBS) of Dyad Flow and Tetric Flow in Primary Molars: An In-vitro Study. J Clin Diagnostic Res. 2018; 12 (10). [ Links ]
32. Heintze SD. Clinical relevance of tests on bond strength, microleakage and marginal adaptation. Dent Mater. 2013; 29 (1): 59-84. [ Links ]
33. Gale MS, Darvell BW. Thermal cycling procedures for laboratory testing of dental restorations. J Dent. 1999; 27 (2): 89-99. [ Links ]
34. Ilie N, Hilton TJ, Heintze SD, Hickel R, Watts DC, Silikas N, Stansbury JW, Cadenaro M, Ferracane JL.Academy of Dental Materials guidance-Resin composites: Part I-Mechanical properties. Dent Mater. 2017; 33 (8): 880-94. [ Links ]
35. Nedeljkovic I, Teughels W, De Munck J, Van Meerbeek B, Van Landuyt KL. Is secondary caries with composites a material-based problem? Dent Mater. 2015; 31 (11):e247-77. [ Links ]
36. Demarco FF, Collares K, Correa MB, Cenci MS, Moraes RR de, Opdam NJ. Should my composite restorations last forever? Why are they failing? Braz Oral Res. 2017;31 (suppl 1). [ Links ]
37. van de Sande FH, Opdam NJ, Rodolpho PADR, Correa MB, Demarco FF, Cenci MS. Patient risk factors' influence on survival of posterior composites. J Dent Res. 2013; 92 (7 Suppl): 78S-83S. [ Links ]
38. Hamburger JT, Opdam NJM, Bronkhorst EM, Huysmans MCDNJM. Indirect restorations for severe tooth wear: fracture risk and layer thickness. J Dent. 2014; 42 (4): 413-8. [ Links ]
39. Leloup G, D'Hoore W, Bouter D, Degrange M, Vreven J. Meta-analytical review of factors involved in dentin adherence. J Dent Res. 2001; 80 (7): 1605-14. [ Links ]
40. De Munck J, Mine A, Poitevin A, Van Ende A, Cardoso MV, Van Landuyt KL, Peumans M, Van Meerbeek B. Meta-analytical Review of Parameters Involved in Dentin Bonding. J Dent Res. 2012; 91 (4): 351-7. [ Links ]
41. Van Meerbeek B, Peumans M, Poitevin A, Mine A, Van Ende A, Neves A, De Munck J. Relationship between bond-strength tests and clinical outcomes. Dent Mater. 2010; 26 (2): e100-21. [ Links ]
42. Laske M, Opdam NJM, Bronkhorst EM, Braspenning JCC, Huysmans MCDNJM. Longevity of direct restorations in Dutch dental practices. Descriptive study out of a practice based research network. J Dent. 2016; 46: 12-7. [ Links ]
43. Heaven TJ, Gordan VV, Litaker MS, Fellows JL, Brad Rindal D, Firestone AR, Gilbert GH; National Dental PBRN Collaborative Group. Agreement among dentists' restorative treatment planning thresholds for primary occlusal caries, primary proximal caries, and existing restorations: Findings from The National Dental Practice-Based Research Network. J Dent. 2013;41 (8): 718-25. [ Links ]
44. Lucarotti PSK, Holder RL, Burke FJT. Outcome of direct restorations placed within the general dental services in England and Wales (Part 1): variation by type of restoration and re-intervention. J Dent. 2005;33 (10): 805-15. [ Links ]
Conflict of interests The authors declare that they have no conflict of interest regarding companies mentioned in the study.
Authorship contribution MELC has contributed in, 1, 2, 3, 4, 5. MMG has contributed in, 1, 2, 3, 4, 5. CECS has contributed in, 3, 4, 6. FMG has contributed in, 1, 4, 6. GSGP has contributed in, 1, 3, 4, 5, 6.
Received: April 13, 2019; Accepted: January 28, 2020
 Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
