










Services on Demand
Journal

Article
 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Related links
Share

 Permalink
PermalinkOdontoestomatología
Print version ISSN 0797-0374On-line version ISSN 1688-9339
Odontoestomatología vol.21 no.33 Montevideo June 2019 Epub June 01, 2019
https://doi.org/10.22592/ode2019n33a6
Actualización
Interdental brushes, from theory to practice: literature review and clinical indications
1
 http://orcid.org/0000-0002-3381-3732
http://orcid.org/0000-0002-3381-3732
2
, Práctica privada exclusiva Ortopedia, Ortodoncia y Orto-periohttp://orcid.org/0000-0002-0950-346X
1Cátedra de Periodoncia, Facultad de Odontología, Universidad de la República. Uruguay. natalia.asquino@gmail.com
2Práctica privada exclusiva Ortopedia, Ortodoncia y Orto-perio
Interproximal brushes are an interdental hygiene tool with diverse indications that have multiple benefits. Among other uses, they are indicated in patients with periodontal disease, with papillae that do not fill the interdental space, patients with orthodontic appliances, fixed prosthesis or implant.supported prosthesis. The aim of this article is to provide guidance on their clinical use based on the available evidence. The results support their use in combination with dental floss for preventing and treating the most prevalent oral diseases, with a significant effect on biofilm control and gingival inflammation.
Keywords: interproximal brush; inderdental brush; interdental device; interdental hygiene; periodontal diseases; dental caries
Los cepillos interproximales son una herramienta de higiene interdental que tiene variadas indicaciones y múltiples beneficios. Pacientes con enfermedad periodontal, con papilas que no llenan el espacio interdentario, portadores de aparatología ortodóncica, prótesis fija o de implantes entre otros casos, pueden beneficiarse con su utilización. El presente artículo tiene como objetivo dar una orientación de su uso clínico basado en la evidencia científica disponible. Los resultados apoyan su utilización en combinación con el hilo dental para la prevención y tratamiento de las enfermedades bucales más prevalentes, con un efecto marcado sobre el control del biofilm y la inflamación gingival.
Palabras clave: cepillo interproximal; cepillo interdental; higiene interdental; enfermedades periodontales; caries dental.
Introduction
The aim of this article is to highlight the relevance and importance of the use of interproximal brushes to maintain oral health in terms of preventing dental caries and periodontal diseases. This aim has been achieved by compiling the scientific evidence available.
Method
We searched the literature covering papers published between 1965 and 2018 on the Pubmed, Scielo, and Medline databases, using the following descriptors: interproximal brush, interdental brush, interdental hygiene, periodontal disease, dental caries, as well as information provided by product manufacturers.
Development
Effective oral hygiene is essential to maintain good oral health, which is associated to a good general health status and a good quality of life1. Oral biofilm, also known as dental plaque, is a complex bacterial community that develops naturally on the surface of teeth2. However, if it is not disorganized, the bacterial flora changes from Gram.positive to anaerobic Gram.negative bacteria, which are associated with periodontal disease(3.4).
Gingivitis is the reversible, initial stage of periodontal disease(3-5 ), regardless of the fact that not all areas affected by gingivitis evolve to develop periodontitis. Health professionals are not able to predict the degree or the speed of disease progression3.4,6, thus making it necessary to prevent and treat gingivitis3-4. The daily mechanical disorganization of oral biofilm by means of tooth brushing remains the primary self.care method to reach and sustain oral health; according to some studies, the bacteria in biofilms have a natural protection against oral antimicrobial agents7.9.
Primary prevention of periodontal disease comprises educational interventions about it and its related risk factors, together with the disorganization of biofilm by the patient and mechanical removal of biofilm and calculus by the professional. As such, optimum dental hygiene requires patients to have the necessary motivation, adequate tools, and professional oral hygiene instruction10.
Brushing twice a day with fluoride paste is an essential part of the oral hygiene routine of most people in the western world. However, clinical studies show that most individuals cannot achieve total control of their biofilm every time they brush10.
Brushing alone is not enough to reach the interproximal areas, which results in these areas remaining uncleaned6,10.12,14.
As per the ISO 16409 standard, interdental or interproximal brushes are manually activated devices consisting of a wired stem with inserted filaments, designed to clean interdental surfaces.
Good interdental hygiene requires a device that can penetrate between adjacent teeth, as gingivitis usually begins in interdental spaces6,10.12,14.
The conditions in the interdental area, which is exposed to the initial inflammation of the papilla, are ideal for the onset and development of oral biofilm, which favors the development of periodontal disease15.
As periodontal disease and dental caries are more prevalent in the interproximal area, the additional use of interdental hygiene devices should be highly recommended16.
Dental floss has been used for many years together with brushing to remove dental biofilm between teeth. However, many people find interdental brushes easier to use than dental floss, provided that there is enough space between teeth1,17.18,24.25.
Interdental brushes have become an invaluable self.care tool for periodontal patients (who present a high prevalence in the loss of papilla), those with dental implants, with fixed prostheses, and patients undergoing orthodontic treatment. Not only are they indicated for the initial stages of treatment but they also play a relevant role in maintaining oral health in the long term.
Studies have shown their effectiveness in reducing biofilm and inflammation in interproximal spaces and underneath orthodontic devices, as compared to brushing and flossing18.23. They have also been proven to remove biofilm up to 2.2.5 mm beneath the gingival margin22.
It is necessary to stress that cooperation is important for the use of this kind of device, as is its adequate indication by the treating practitioner.
There are so many different kinds of interproximal brushes that choosing one can be an overwhelming task for the patient. It is therefore advisable that oral health professionals recommend a specific one for each particular case, and that they insist on its use during maintenance appointments, in order to motivate patients to re.focus on their hygiene.
The market offer is wide; there are I.shaped or L.shaped brushes, with rigid or flexible handles, small or with interchangeable handles, with triangular, conical or cylindrical heads, or diabolo shaped brushes. A crossover clinical trial by Larsen et al. conducted in 2017 compared the effectiveness of conical and cylindrical interdental brushes in the removal of interproximal biofilm and concluded that in terms of the proximal.lingual surfaces, conically shaped brushes were less effective. There was no significant difference for the rest of the surfaces (proximal and proximal.vestibular)26.
Patients with limited manual dexterity might benefit from using a brush with a wider or an adapted handle. For patients who need to clean interdental spaces in the posterior area, a flexible or L.shaped brush could be the best option.
In terms of size, the brush should fit tightly around the interproximal space, and it should not be necessary to apply force to use it. Patients may need different sizes for different areas, and despite this being tedious or confusing at the beginning, it does not take too long until using them becomes a healthy habit and is done with ease. It is therefore very important to guide the patient in the selection of the right interproximal brush.
The international market offers a wide variety of brands with diameters ranging from 0.4 mm to 2.2 mm GUM®; TePe®; Interprox® ; Pico Jenner®; etc).
Figures 1 - 3 ) show examples of models available in the Uruguayan market.



The size of the brush must be chosen bearing in mind that it needs to touch the interproximal surfaces of the adjacent teeth. The patient may need to increase the diameter of the brush as periodontal tissues recede in response to treatment.
If used correctly, interdental brushes should have a limited lifetime of a week, depending on the quality of the brush and on the technique used. When the bristles deteriorate or the wire feels weaker or bends, the brush must be discarded and replaced.
Interdental brushes must be inserted gently in order to avoid injuring the tissue when brushing, and to increase their lifespan. The brush is first inserted from the vestibular area in the interdental space using circular movements until the other side, either lingual or palatal, is reached. Once there, it is moved horizontally. The brush must be rinsed before it is inserted in a new interdental space. In posterior areas where the vestibular and palatal/lingual tissues are at different levels, the brushes can be curved slightly to prevent the tip from impacting against the tissue on the other side and accidentally hurting the soft tissue (Figures 4 and 5A ).




Fig. 5: B . Use of interdental brush in interradicular area of lower molar, after a tunneling procedure to treat a degree.2 furcation.
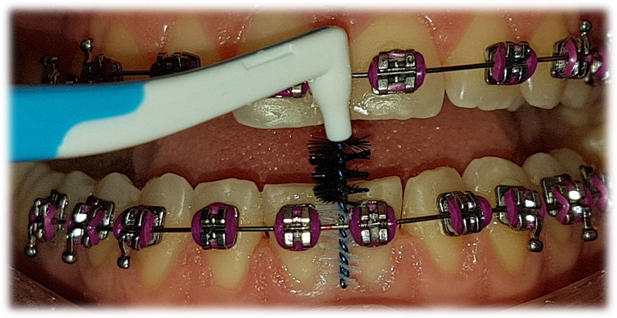
The use of interdental brushes in orthodontic treatments (Fig. 6) has major benefits since orthodontics devices retain large amounts of biofilm. Their use is recommended on all four sides of the brackets (Fig. 6) and with special care under buccal tubes (Fig. 7) and hooks (Fig. 8 and Fig. 9



After its use, the brush must be washed thoroughly with running water, and it must be left to dry in a clean place.
Discussion
In their systematic review, Slot et al.27 evaluated the effectiveness of interproximal brushes based on gingival inflammation parameters, and they concluded that interdental brushes remove more biofilm than regular brushing alone, or brushing and flossing, or using interdental toothpicks; reduction in probing depth was greater with the interdental brush, but there was no difference in the gingival inflammation indexes when compared with flossing.
To this date, two systematic reviews conducted by Hennequin.Hoenderdos et al. in 201728 and Abouassi et al. in 201429 compared the effectiveness of interdental brushes and rubber interdental cleaning devices, and they concluded that there were no statistically significant differences in the reduction of gingival inflammation and of interdental plaque indexes.
A systematic review conducted by Bock et al.(30 did not find significant differences between the use of interdental brushes and single tuft brushes in patients undergoing orthodontic treatment, but did so in terms of preference, since patients preferred to use interdental brushes.
Conclusions
The best care for the patient is not only in the clinician’s judgment or in the scientific evidence, but in the art of combining both through the interaction with the patient, in order to find the best option for each individual11.
There is currently a wide range of treatments available to restore the aesthetics and the function lost by our patients. The results achieved in recent years in the area of orthodontics, implants, and rehabilitation are extraordinary. However, we must not lose sight of the importance of the prevention of caries and gingival diseases, preventing new diseases and the relapse of diseases that have already been treated.
Most prevalent oral diseases, such as caries and periodontal disease, can be effectively prevented with an adequate program that involves oral health and general education, and with a strict maintenance program.
A good selection and use of oral hygiene devices is part of this process.
The responsibility of educating current and future generations on the importance of oral health care, and how it can have affect the individual’s general health, lies with the dental professional.
If it is necessary to implement any kind of sophisticated treatment, it must be accompanied by the right post.treatment maintenance
Referencias
1. Poklepovic T, Worthington HV, Johnson TM, Sambunjak D, Imai P, Clarkson JE, Tugwell P.Interdental brushing for the prevention and control of periodontal diseases and dental caries in adults. The Cochrane Database Syst Rev. 2013; 18 (12): CD009857.doi: 10.1002/14651858.CD009857.pub2. [ Links ]
2. Marsh PD. Plaque as a biofilm: pharmacological principles of drug delivery and action in the sub. and supragingival environment. Oral Dis. 2003; 9 (Suppl.1): 16-22. [ Links ]
3. Rosen PS. American Academy of Periodontology. Research, science, and therapy committee. Treatment of plaque.induced gingivitis, chronic periodontitis, and clinical conditions. Pediatr Dent. 2008.2009; 30 (7 Suppl): 253-262. [ Links ]
4. Haffajee AD, Socransky SS. Introduction to microbial aspects of periodontal biofilm communities, development, and treatment. Periodontol 2000. 2006; 42:7-12. [ Links ]
5. Mariotti A. Dental Plaque.induced Gingival Diseases. Annals of Periodontology 1999; 4(1): 7-19. [ Links ]
6. Loe H, Theilade E, Jensen SB. Experimental gingivitis in man. J Periodontol 1965 ;36: 177-187. [ Links ]
7. Costerton JW, Stewart PS, Greenberg EP. Bacterial biofilms: a common cause of persistent infections. Science. 1999; 284 (5418): 1318-1322. [ Links ]
8. Schaudinn C, Gorur A, Keller D, Sedghizadeh PP, Costerton JW. Periodontitis: an archetypical biofilm disease. J Am Dent Assoc. 2009; 140 (8): 978-986. [ Links ]
9. Kuramitsu HK, He X, Lux R, Anderson MH, Shi W. Interspecies interactions within oral microbial communities. Microbiol Mol Biol Rev. 2007; 71 (14): 653-670 [ Links ]
10. Van der Weijden F, Slot DE. Oral hygiene in the prevention of periodontal diseases: the evidence. Periodontol 2000.2011; 55 (1): 104-123. [ Links ]
11. Van der Weijden GA, Slot DE. Interdental oral hygiene: the evidence. En: Bartold PM, Jin LJ (eds). Multi.disciplinary management of periodontal disease. Proceedings of the 9th Asian Pacific Society of Periodontology Meeting; 9.10 September, 2011. Hong Kong: Asian Pacific Society of Periodontology; 2011. [ Links ]
12. Nayak RP, Wade AB.The relative effectiveness of plaque removal by the Proxabrush and rubber cone stimulator. J Clin Periodontol. 1977; 4 (2): 128-133. [ Links ]
13. Hansen F, Gjermo P. The plaque.removing effect of four toothbrushing methods. Scand J Dent Res. 1971; 79 (7): 502-506. [ Links ]
14. Loe H. Oral hygiene in the prevention of caries and periodontal disease. Int Dent J. 2000; 50 (3):129-139. [ Links ]
15. Sicilia A, Arregui I, Gallego M, Cabezas B, Cuesta S. A systematic review of powered vs manual toothbrushes in periodontal cause.related therapy. J Clin Periodontol . 2000; 29 (Suppl. 3): 39-54. [ Links ]
16. Imai PH, Yu X, Macdonald D. Comparison of interdental brush to dental floss forreduction of clinical parameters of periodontal disease: A systematic review. Can J Dent Hyg. 2012; 1: 63-78. [ Links ]
17. Bergenholts A, Olsson A. Efficacy of plaque.removal using interdental brushes and waxed dental floss. Scand J Dent Res . 1984; 92 (3): 198-203. [ Links ]
18. Christou V, Timmerman MF, Van der Velden U, Van der Weijden FA. Comparison of different approaches of interdental oral hygiene: interdental brushes versus dental floss. J Periodontol . 1998; 69 (7): 759-764. [ Links ]
19. Imai PH, Hatzimanolakis PC. Interdental brush in type I embrasures: Examiner blinded randomized clinical trial of bleeding and plaque efficacy. Can J Dent Hyg 2011; 45 (1):13-20. [ Links ]
20. Jackson MA, Kellett M, Worthington HV, Clerehugh V. Comparison of interdental cleaning methods: a randomized controlled trial. J Periodontol . 2006; 77: 1421-1429. [ Links ]
21. Kiger RD, Nylund K, Feller RP. A comparison of proximal plaque removal using floss and interdental brushes. J Clin Periodontol . 1991; 18: 681-684. [ Links ]
22. Waerhaug J.The interdental brush and its place in operative and crown and bridge dentistry. J Oral Rehabil. 1976; 3 (2): 107-13. [ Links ]
23. Salzer S, Slot DE, Van der Weijden FA, D€orfer CE. Efficacy of inter.dental mechanical plaque control in managing gingivitis . a meta.review. J Clin Periodontol . 2015; 42 (Suppl. 16): 92-105. [ Links ]
24. Imai PH, Hatzimanolakis PC. Encouraging client compliance for interdental care with the interdental brush: The client’s perspective. Can J Dent Hyg . 2010; 44 (2):71-75. [ Links ]
25. Ishak N, Watts TLP.A comparison of the efficacy and ease of use of dental floss and interproximal brushes in a randomised split mouth trial incorporating an assessment of subgingival plaque. Oral Health Prev Dent. 2007; 5: 13-18. [ Links ]
26. Larsen HC, Slot DE, Van Zoelen C, Barendregt DS, Van der Weijden GA. The effectiveness of conically shaped compared with cylindrically shaped interdental brushes. a randomized controlled clinical trial. Int J Dent Hyg. 2017;15 (3): 211-218. [ Links ]
27. Slot DE, Dorfer CE, Van der Weijden GA. The efficacy of interdental brushes on plaque and parameter of periodontal inflammation: a systematic review. Int J Dent Hyg. 2008; 6:253-264. [ Links ]
28. Hennequin.Hoenderdos NL, Van der Sluijs E, Van der Weijden F, Slot DE. Efficacy of a rubber bristles interdental cleaner compared to an interdental brush on dental plaque, gingival bleeding and gingival abrasion: A randomized clinical trial. Int J Dent Hygiene. 2018; 16 (3): 380-383. [ Links ]
29. Abouassi T, Woelber JP, Holst K, Stampf S, Doerfer CE, Hellwig E, Ratka.Kruger P. Clinical efficacy and patients’ acceptance of a rubber interdental bristle. A randomized controlled trial. Clin Oral Investig. 2014;18 (7): 1873-80 [ Links ]
30. Bock NC, Von Bremen J, Kraft M, Ruf S. Plaque control effectiveness and handling of interdental brushes during multibracket treatment. a randomized clinical trial. Eur J Orthod; 2010; 32 (4): 408-13. [ Links ]
Received: December 18, 2018; Accepted: April 02, 2019
 Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
