










Services on Demand
Journal

Article
 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Related links
Share

 Permalink
PermalinkOdontoestomatología
Print version ISSN 0797-0374On-line version ISSN 1688-9339
Odontoestomatología vol.20 no.32 Montevideo Dec. 2018
https://doi.org/10.22592/ode2018n32a7
Investigación
Satisfaction with the use of fixed orthodontic appliances in patients from Valdivia and Paillaco, 2017. Observational study
1
 http://orcid.org/0000-0003-2098-3369
http://orcid.org/0000-0003-2098-3369
2
http://orcid.org/0000-0002-1306-3735
1 Escuela de Odontología, Facultad de Medicina, Valdivia, Universidad Austral de Chile. fgallegosdelgado@gmail.com
2 Escuela de Odontología, Facultad de Medicina, Valdivia, Universidad Austral de Chile.
3 Instituto de Odontoestomatología, Facultad de Medicina, Valdivia, Universidad Austral de Chile
4 Instituto de Odontoestomatología, Facultad de Medicina, Valdivia, Universidad Austral de Chile
Objective:
To determine user satisfaction with fixed orthodontic appliances during the first three checkups after installation.
Materials and methods:
A cross-sectional observational study was conducted with patients who started fixed orthodontic treatment in health centers in Paillaco and Valdivia. For this, a survey instrument validated in Spanish by Gacitúa et al. (2016) was used. To establish differences, the Friedman test was performed with a p<0.05 significance level.
Results:
Thirty-four patients participated (14.1 (SD ± 3.5) years old). The total satisfaction score was 37.94 (SD ± 7.13) points for the first month, 40.56 (SD ± 6.35) points for the second and 41.09 (SD ± 6.92) points for the third.
Conclusion:
General satisfaction levels with orthodontic appliances increase as the orthodontic treatment extends over time.
Keywords: orthodontic appliances; orthodontics; personal satisfaction
Objetivo:
Determinar satisfacción usuaria en el uso de aparatos de ortodoncia fija post instalación.
Material y métodos:
Estudio observacional de corte transversal, en pacientes con tratamiento de ortodoncia fija en centros de salud de la ciudad de Valdivia y Paillaco. El nivel de satisfacción fue medido mediante una encuesta validada al español de Gacitúa et al., (2016). Para establecer diferencias, se realizó la prueba de Friedman con un nivel de significancia p<0,05.
Resultados:
Participaron 34 pacientes. La edad promedio fue de 14,1 DE ± 3,5 años. El puntaje total de satisfacción para el primer control fue 37,94 (DE ± 7,13) puntos, 40,56 (DE ± 6,35) puntos para el segundo y 41,09 (DE ± 6,92) puntos para el tercero.
Conclusión:
El nivel de satisfacción en el uso de aparatos de ortodoncia fija, aumenta a medida que transcurre el tratamiento de ortodoncia
Palabras clave: aparatos ortodónticos; ortodoncia; satisfacción personal
Introduction
In Chile, the prevalence of caries and periodontal diseases has declined in people under the age of 201. However, dento-maxillary anomalies, affecting 38.29% of children aged 6 and 53% of children aged 12, have not significantly decreased over time2.
Therefore, corrective orthodontic treatment with brackets is an option to address these anomalies, because it improves aesthetics and therefore patients’ quality of life3. However, the use of these appliances in an area as sensitive as the oral cavity may cause discomfort4, and there often appear oral ulcers5-6 and pain, especially in the first few months7.
The information on the first three months of orthodontic treatment is essential for the clinical trial, and as mentioned above, the appearance of pain and functional limitations in this period may disappoint certain patients, affecting their motivation, cooperation spirit, and it may even lead them to abandon the treatment7-8.
Marques et al.9 show that approximately 16% of patients experience a degree of discomfort when using fixed orthodontic appliances, which has a negative impact on their quality of life. However, in the study conducted by Gacitúa et al.10 in Santiago de Chile, there was a significant difference in level of satisfaction between the first and second evaluations, the latter yielding the best result. However, there was no follow-up after the first month.
Given this background, the aim of this study is to assess the level of satisfaction with the use of fixed orthodontic appliances in users attending health centers in Valdivia and Paillaco in 2017.
Materials and methods
An observational cross-sectional study was conducted between May and October of 2017. The target population were patients who had started treatment with fixed orthodontic appliances in public and private health centers in Paillaco and Valdivia.
The sample size was designed considering the results of Gacitúa et al.10, who found an average overall satisfaction score before the orthodontic treatment of 27.2 points (SD ± 4.48); our hypothesis posits a difference between the first and third checkups in the scale average: 31.2 points (SD ± 4.48). Considering a power level of 0.9 and an alpha error of 0.05, and 25% of additional observations in case there is no follow-up, a sample size of 34 users was estimated. This was calculated using Stata software, version 10.0 (StataCorp USA).
The study included patients over 9 and under 25 of both sexes, who could read and write in Spanish, and who voluntarily accepted to participate in the study, following the required protocols in the case of minors.
The users included in this study had fixed appliances, with MBT or Roth prescription metal brackets11, and were diagnosed with moderate or severe negative dento-maxillary discrepancy12. Users with additional orthodontic appliances like transpalatal arches, lingual arches, mini implants and Quad Helix were also included.
Users excluded from the study; users who needed conventional orthodontic treatment and also surgical treatment, presence of mild negative dentomaxillary discrepancy, users of removable and/or fixed dentures, presence of periodontal disease, chronic diseases, those undergoing analgesic therapy, presence of some type of temporomandibular disorder13, oral pathology causing pain, speech disorder and those with some type of condition that might prevent them from completing the survey autonomously.
To measure satisfaction, the questionnaire developed by Gacitúa et al.10) was used. It included ten statements, which were grouped in three areas: oral hygiene (OH), comfort (CF) and aesthetic self-perception (ASP); each with a certain number of questions, three for OH, four for CF and three for ASP. According to the literature, these are essential elements in orthodontic treatment9,14. Each question has a value between 0 and 5 in alternatives with Likert format (5: very satisfied, 4: satisfied, 3: acceptable, 2: dissatisfied, and 1: very dissatisfied). Non-answers were awarded a 0 value. The total score of the questionnaire ranges between 0 and 50 points, where a higher score indicated greater satisfaction.
The invitation to participate in the study was made to patients in the centers described, which was approved by the Ethics Committee of the Valdivia Health Service. In the case of users under 18, their permission was requested and their representatives had to sign an informed consent.
The surveys were administered by two researchers (G.F. and S.A.) who were calibrated by administering it to ten patients who had already completed their treatment with fixed orthodontic appliances. The first survey was administered one month after the installation of the fixed appliances, which was the first checkup. The following surveys were administered in the two subsequent checkups, corresponding to the second and third months. At the time of installation, all the patients were instructed on the necessary care regarding hygiene, eating and potential discomfort.
The variables studied were sex, total score of the questionnaire and score of each area (OH, CF, ASP). The data were organized in a Google spreadsheet (Google Inc. USA.).
A descriptive statistics analysis using central tendency and dispersion measures was conducted. The Shapiro Wilk test was performed to determine the normality of the data. To establish differences between scores and the different health centers, the Friedman test was performed with a p<0.05 significance level, for which free-access statistical software R, version 3.4.1, was used.
Results
Thirty-six patients fulfilled the selection criteria. Follow-up could not be conducted with two of them, so the survey was correctly administered to 34 users. Twenty-one were women (61.8%) and 13 were men (38.2%). The average age was 14.1 (SD ± 3.5).
The total satisfaction score was 37.94 (SD ± 7.13) points for the first checkup, 40.56 (SD ± 6.35) for the second and 41.09 (SD ± 6.92) for the third. Table 1 shows the total satisfaction scores obtained per checkup in the health centers studied.
Table 1: Total overall satisfaction score according to checkup and health center
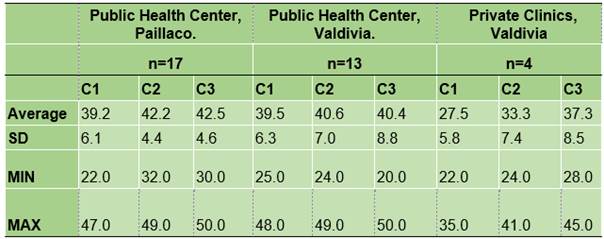
C1: Checkup 1 C2: Checkup 2 C3: Checkup 3 SD: Standard Deviation MIN: Minimum value MAX: Maximum value
In oral hygiene, the mean obtained for women was 11 (SD ± 2.3) points for the first checkup, 11 (SD ± 2.5) points for the second, and 11 (SD ± 2.2) points for the third. Among men, the mean obtained was 11 (SD ± 2.5) points for the first checkup, 11 (SD ± 2.5) for the second and 12 (SD ± 3.0) for the third (Fig. 1).
Fig. 1: Scores obtained for oral hygiene (checkups 1, 2 and 3) after the application of the satisfaction questionnaire
The scores obtained for comfort are seen in Fig. 2. The mean for women in the first checkup was 15 (SD ± 3.4) points, 16 (SD ± 2.8) points for the second, and 16 (SD ± 2.9) for the third. For men, the mean result was 14 (SD ± 3.8) points for the first checkup, 17 (SD ± 3.5) points for the second and 17 (SD ± 4.1) for the third.
Fig. 2: Scores obtained for comfort, (checkups 1, 2 and 3) after the application of the satisfaction questionnaire
For aesthetic self-perception, the scores obtained are shown in Fig. 3. The mean for women in the first checkup was 13 (SD ± 2.7) points, 13 (SD ± 2.0) points for the second, and 14 (SD ± 1.5) for the third. The mean for men in the first checkup was 11 (SD ± 3.4) points, 13 (SD ± 2.5) points for the second, and 13 (SD ± 2.9) for the third.
Fig. 3: Scores obtained for aesthetic self-perception (checkups 1, 2 and 3) after the application of the satisfaction questionnaire
There were no statistically significant differences (p>0.05) when comparing the total score of the surveys in the various checkups per health center, nor when assessing these results regarding satisfaction.
Discussion
Despite using different methods to assess satisfaction with the use of fixed appliances, the studies conclude that there is an impact on the user’s quality of life right after installation. Therefore, the aim of this study was to assess the level of satisfaction with the use of fixed orthodontic appliances in users attending health centers in Valdivia and Paillaco.
Regarding our results, an increase was found in the average total satisfaction score in all health centers after the checkups. In Paillaco, this increase was 3.3 points, 0.9 points for the public health center in Valdivia and 9.8 points in the private health center in Valdivia. These results suggest that satisfaction with the use of brackets is steady during the treatment or that it increases slightly during this period.
By contrasting these results with those obtained by Gacitúa et al. 10, who administered the same survey a week and a month after installation and reported a significant increase in satisfaction, greater than 10 points between these two instances, such values cannot be compared with those of this study since the surveys were administered for the first, second and third month after installation. This study showed an increase of 3.15 points between the first and third checkups, which is considerably lower. However, both results show an increase in average satisfaction with the use of fixed appliances.
Regarding oral hygiene, in this study there was no significant increase in the scores, which can be attributed to the fact that clinicians were good motivators and educators, and also because patients understood the instructions given. With fixed orthodontic appliances, maintaining good hygiene and proper plaque removal become more difficult and require more time and frequency of brushing15, especially at the beginning of the treatment given the malocclusion present. As biofilm elimination is deficient, the prevalence of caries lesions increases as the treatment progresses16,17, which could lead to a long-term negative effect regarding the degree of satisfaction of users of orthodontic appliances.
A similar trend was found for comfort, with a slight increase in the average score between the first and second checkup, which remained steady for the third, without significant differences between the groups. This means that patients better adapt to and feel more comfortable with the appliance over time. Wu et al.,18 had similar results, reporting an improvement in this area over time. Although both groups reached a level of satisfaction similar to that of the third checkup, men showed a slight increase in the score for this area, which is consistent with what Krishnan7 reports, who states that men might achieve higher levels of satisfaction than women.
The comfort dimension includes topics such as eating, pain, and phonation. Regarding eating, the potential changes experienced by users of fixed orthodontic appliances are widely documented: difficulty when eating and chewing certain types of harder foods5, which leads to eating smaller amounts and softer foods 6. One of the reasons for this change is the fact that certain foods adhere to the metal brackets, which makes it more difficult to preserve good oral hygiene15. Despite these difficulties, Johal et al.6 describe that as the treatment progresses, patients can adapt and resume their normal eating habits.
Regarding communication, as reported by Villanueva et al.19, phonation problems decrease considerably on the seventh day after installing the orthodontic appliance. In turn, Khattab et al.20 note that phonation is negatively affected from the time of installation. However, in the following months, the patients did not experience any difficulty speaking or pronouncing words. Additionally, Martínez et al.21 indicate that 29.15% of phoneme production and perception is affected a month after installation.
Regarding pain, it increases between 4 and 24 hours after adjusting the fixed appliances, decreasing gradually and returning to normal on the seventh day9. These results are similar to those mentioned by Salmassian et al.4 regarding the reduction of pain over time.
Marques et al.9 state that younger patients have better tolerance to pain and are more adaptable to discomfort with the use of fixed appliances. Krishnan7 reached different results: adolescents reported the most pain, unlike preadolescents and adults. In this same study, regarding difference according to sex, women have greater levels of discomfort, ulcers and related pain than men do, while others find no significant differences.
When analyzing aesthetic self-perception, Feldens et al.22 say that one of the reasons to start orthodontic treatment is to improve aesthetics, which was more prevalent among women. This was also observed by Pachêco-Pereira et al.23, who state that women have higher expectations than men regarding the treatment. This could explain the results of this study, where women’s level of satisfaction does not increase in the first three checkups, compared with men, who do show a slight increase in satisfaction after the second checkup.
This area remains controversial: on the one hand, patients find that using fixed appliances is not aesthetic24, and on the other hand, the presence of brackets has not shown a negative impact on the aesthetic evaluation of the smile in patients with this type of appliance25.
Within the limitations of our study, although the survey used10 provides a satisfaction questionnaire validated for the use of metal brackets, it has been used in few studies. It is also important to consider that this questionnaire has no cut-off value to determine patient dissatisfaction or satisfaction. Although we took all the necessary measures to avoid information biases, they might still be present.
Future studies could assess satisfaction over longer periods of treatment, in a more heterogeneous population, and consider more variables that differentiate each orthodontic treatment.
In conclusion, the level of satisfaction of users of brackets improves as orthodontic treatment progresses, both in the overall experience and for each area analyzed: oral hygiene, comfort and aesthetic self-perception.
Referencias
1. Cartes-Velásquez R, Araya E, Valdés C. Maloclusiones y su Impacto Psicosocial en Estudiantes de un Liceo Intercultural. Int J Odon. 2010; 4 (1): 65-70. [ Links ]
2. Chile. Ministerio de Salud, Gobierno de Chile. Diagnóstico Nacional de Salud Bucal del Adolescente de 12 años y Evaluación del Grado de Cumplimiento de los Objetivos Sanitarios de Salud Bucal 2000-2010. Chile. 2007: 1-15. [ Links ]
3. Silvola AS, Varimo M, Tolvanen M, Rusanen J, Lahti S, Pirttiniemi P. Dental esthetics and quality of life in adults with severe malocclusion before and after treatment. Angle Orthod. 2014; 84 (4): 594-99. [ Links ]
4. Salmassian R, Oesterle LJ, Shellhart WC, Newman SM. Comparison of the efficacy of ibuprofen and acetaminophen in controlling pain after orthodontic tooth movement. Am J Orthod Dentofacial Orthop.2009; 135 (4): 516-21. [ Links ]
5. Abed Al Jawad F, Cunningham S, Croft N, Johal A. A qualitative study of the early effects of fixed orthodontic treatment on dietary intake and behaviour in adolescent patients. Eur J Orthod. 2012;34 (4): 432-36. [ Links ]
6. Johal A, Abed Al Jawad F, Marcenes W, Croft N. Does orthodontic treatment harm children's diets? J Dent. 2013; 41 (11): 949-54. [ Links ]
7. Krishnan V. Orthodontic pain: from causes to management - a review. Eur J Orthod. 2007; 29 (2): 170-79. [ Links ]
8. Abreu L, Melgaço C, Abreu M, Lages E, Paiva S. Agreement between adolescents and parents or caregivers in rating adolescents' quality of life during orthodontic treatment. Am J Orthod Dentofacial Orthop.2015; 148 (6): 1036-42. [ Links ]
9. Marques L, Paiva S, Vieira-Andrade R, Pereira L, Ramos-Jorge M. Discomfort associated with fixed orthodontic appliances: determinant factors and influence on quality of life. Dental Press J. Orthod. 2014; 19 (3): 102-7. [ Links ]
10. Gacitúa P, Werlinger F, Ríos M, Alvarez E. Satisfacción del uso de brackets metálicos en relación a higiene oral, confort y autopercepción estética. Rev Cubana Estomatol. 2016; 53 (1): 21-7. [ Links ]
11. Ventureira C. Prescripción variable en ortodoncia: lo que todo ortodoncista debería conocer. Rev Esp Ortodon. 2010; 40: 9-24. [ Links ]
12. Comas R, De la Cruz J, Díaz E, Carreras C, Ricardo M. Relación entre los métodos clínicos y de Moyers-Jenkins para la evaluación del apiñamiento dentario. MEDISAN. 2015; 19 (11): 1309-16. [ Links ]
13. American Academy of Orofacial Pain & Okeson J. Orofacial Pain: guidelines for assessment, diagnosis, and management. Chicago: Quintessence Pub.Co., Inc; 1996. [ Links ]
14. Zhou Y, Wang Y, Wang X, Volière G, Hu R. The impact of orthodontic treatment on the quality of life a systematic review. BMC Oral Health. 2014; 14 (1): 1-7. [ Links ]
15. Azaripour A, Weusmann J, Mahmoodi B, Peppas D, Gerhold-Ay A, Van Noorden C, Willershausen B. Braces versus Invisalign(r): gingival parameters and patients' satisfaction during treatment: a cross-sectional study. BMC Oral Health. 2015; 15 (1): 1-5. [ Links ]
16. Ahmed I, Haque S, Nazir R. Carious lesions in patients undergoing orthodontic treatment. J Pak Med Assoc. 2011; 61 (12): 1176-9. [ Links ]
17. Shrestha S, Shrestha L, Shrestha N, Shrestha R. Effect of Orthodontic Treatment in Occurrence of Dental Caries. Orthodontic Journal of Nepal. 2013; 3 (1): 31-6. [ Links ]
18. Wu A, McGrath C, Wong RW, Wiechmann D, Rabie AB. Comparison of oral impacts experienced by patients treated with labial or customized lingual fixed orthodontic appliances. Am J Orthod Dentofacial Orthop. 2011;139 (6): 784-90. [ Links ]
19. Villanueva P, Lizana ML, Huber H, Morán D, Fernández MA, Palomino H. Modificaciones en la articulación de fones en pacientes con aparato ortodóncico fijo lingual. Rev CEFAC. 2007; 9 (4): 483-89. [ Links ]
20. Khattab TZ, Farah H, Al-Sabbagh R, Hajeer MY, Haj-Hamed Y. Speech performance and oral impairments with lingual and labial orthodontic appliances in the first stage of fixed treatment. Angle Orthod. 2013; 83 (3): 519-26. [ Links ]
21. Martínez H, Mora E, Prato R. Influencia de los aparatos dentales ortodónticos en la producción y percepción del habla: estudio de cinco casos. Rev CEFAC. 2006; 8 (4): 467-76. [ Links ]
22. Feldens C, Nakamura E, Tessarollo F, Closs L. Desire for orthodontic treatment and associated factors among adolescents in southern Brazil. Angle Orthod. 2015; 85 (2): 224-32. [ Links ]
23. Pachêco-Pereira C, Abreu L, Dick B, De Luca Canto G, Paiva S, Flores-Mir C. Patient satisfaction after orthodontic treatment combined with orthognathic surgery: A systematic review. Angle Orthod. 2016; 86 (3): 495-08. [ Links ]
24. Fonseca L, Araújo T, Santos A, Faber J. Impact of metal and ceramic fixed orthodontic appliances on judgments of beauty and other face-related attributes. Am J Orthod Dentofacial Orthop. 2014;145 (2): 203-06. [ Links ]
25. Berto P, Lima C, Lenza M, Faber J. Esthetic effect of orthodontic appliances on a smiling face with and without a missing maxillary first premolar. Am J Orthod Dentofacial Orthop. 2009;135 (4): 55-60. [ Links ]
Received: May 14, 2018; Accepted: July 30, 2018
 Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
