










Servicios Personalizados
Revista

Articulo
 texto en
texto en  Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
Links relacionados
Compartir

 Permalink
PermalinkOdontoestomatología
versión impresa ISSN 0797-0374versión On-line ISSN 1688-9339
Odontoestomatología vol.20 no.32 Montevideo dic. 2018
https://doi.org/10.22592/ode2018n32a6
Research
Validation of a new placebo acupuncture method with potential for double blinding. Phase II: practitioner blinding
1
 http://orcid.org/0000-0002-7942-9189
http://orcid.org/0000-0002-7942-9189
2
http://orcid.org/0000-0001-6463-1280
11-Cátedra de Fisiología, Facultad Odontología, Universidad de la República. Uruguay. ale-fp@hotmail.com
22-Cátedra de Fisiología, Facultad Odontología, Universidad de la República. Uruguay
33-Cátedra de Fisiología, Facultad Odontología, Universidad de la República. Uruguay
44-Instituto de Estadística, Facultad de Ciencias Sociales y Administración. Universidad de la República. Uruguay
Methodology:
We conducted two experimental studies using the acupuncture point of the Large Intestine 4 (LI 4) as reference. In the first study (I), three practitioners used the device on the same patient. In the second experiment (II), a single acupuncturist used this device on 12 healthy volunteers.
Results:
In I, out of 30 needles used by the practitioners, they were able to correctly identify 7 needles (23%) (practitioner #1, 2/10; practitioner #2, 4/10; and practitioner #3, 1/10). In experiment II, success rates were around 50%, so there is not enough evidence to state that the acupuncturist recognizes the type of needle used.
Conclusions
The new device showed high potential for practitioner blinding, suggesting that it is useful to blind even experienced acupuncturists.
Keywords: acupuncture; placebo; double blind; LI 4; Chinese medicine
Se presenta un nuevo método de acupuntura placebo, evaluándose en esta fase el cegamiento del operador.
Metodología:
Se implementaron dos estudios experimentales utilizando como referencia el punto acupuntural Intestino Grueso 4 (IG4). En el primero (I) tres operadores utilizaron el dispositivo desarrollado en un mismo paciente. Mientras que en un segundo experimento (II), un único acupunturista utilizó dicho dispositivo en 12 voluntarios sanos.
Resultados:
En I, sobre un total de 30 agujas que utilizaron los operadores, estos pudieron identificar correctamente 7 (23%). Por otra parte, en el experimento II, los porcentajes de acierto encontrados no fueron significativamente diferentes de 50%, por lo cual no hay evidencia suficiente que permita decir que el acupunturista reconoce el tipo de aguja que está utilizando.
Conclusiones:
El nuevo dispositivo evidenció un alto potencial de cegamiento del operador, sugiriendo que es útil para enmascarar incluso a acupunturistas experimentados.
Palabras clave: Acupuntura; placebo; doble ciego; IG4; medicina china
Introduction
Traditional Chinese medicine is a medical system made up of several different diagnostic and therapeutic practices developed over thousands of years. The basis of this philosophy differs in several aspects from Western medical philosophy, essentially considering meridian systems, the concept of energy balance, and other systemic and emotional features 1-4.
Acupuncture is one of the most widespread therapies, even in Western medicine. However, it has met resistance in academic and scientific fields, given the methodological difficulties researchers have had to prove their real therapeutic effect 5. To assess the real therapeutic effect of an intervention, the Gold Standard 6) is set by means of randomized controlled clinical trials (RCTs). Likewise, the use of placebos for control purposes in said research is essential to assess the real effectiveness of an intervention 7. However, given the absence of a proper placebo method in acupuncture to be used as control in clinical studies, researchers have applied diverse comparative methods such as TENS 8, laser 9, superficial acupuncture 10-11, the stimulation of points which are close to acupuncture points 10,12 or a combination of the latter 13-15, thus raising questions regarding the internal and external validity of said studies.
Developing a placebo acupuncture needle as a control mechanism for clinical research purposes has been a historical challenge in this area of knowledge. Over the last few years, efforts have been made to develop and validate several placebo methods, and they have been used in RCTs, but these mechanisms still have several limitations16. One of their weaknesses is that, although they use blunt tip needles, they press on the skin and may stimulate afferent nerve fibers, generating physiological responses which act as confusion variables that are impossible to control 17-19. Therefore, these devices are not inert 20-22.
Some promising devices have emerged in the last few decades 23-27, though only the one developed by Takakura has double blind potential 16,26,28-29 30. However, some of these devices are either difficult to find or to produce/manufacture. This is why developing a placebo system that allows for double blinding, which is trustworthy and easy to build, comes as a challenge to clinical research in this area. In a previous study, our group developed a new reliable placebo acupuncture system, which was cost-effective and single blind; it was validated in a group of healthy volunteers with no previous experience with acupuncture 25.
This pilot study analyzes an adjustment to that system to assess the blinding of the operator and to thus obtain a potential double blind system. The hypothesis proposed that the operator (acupuncturist) would not be capable of telling real needles from placebo needles.
Methodology
Two experimental studies were implemented to test the blinding of the operator under this new system.
The following criteria were used to select the patients:
Inclusion criteria:
-Aged between 18 and 65.
-Willing to take part in a study where an acupuncture needle is inserted and left for 30 seconds.
Exclusion criteria:
-Fear of needles
-Pregnancy
-High blood pressure (≥ 140/90)
-Wounds or alterations in the area of the acupuncture point to be stimulated
-Use of psychotropic drugs
-Chronic painkiller use
Experiment 1
Three operators (acupuncturists with over 10 years’ experience) were tested in their ability to tell the difference between real and placebo needles on the same patient. For this purpose, they received a set of 10 needles in total, which included a random number of real and placebo needles, organized in random order. After applying the acupuncture technique on each volunteer, the operator answered a questionnaire stating what kind of needle they thought they had used. The options were: real, placebo, does not know. At the same time, they were asked to mark the degree of confidence or certainty regarding their answer on a 100-mm visual analogue scale, 0 being not sure at all, and 100 absolutely certain. This experiment was conducted on the same 56-year-old female volunteer.
Experiment 2
One acupuncturist with over 10 years’ experience was tested in his ability to tell real needles from placebo needles on 12 volunteers (2 men and 10 women, aged 20 on average). All the volunteers were healthy students at the School of Dentistry of Universidad de la República, Uruguay. The operator used two needles on each volunteer, a real one and a placebo needle, in random order. After inserting each needle, the operator answered the following question from a questionnaire: What kind of needle do you think you used? The options were real or placebo. After that, they were asked to state the degree of confidence or certainty of their answer on a 100-mm visual analogue scale, 0 being not sure at all, and 100 absolutely certain. The order of the real and placebo needles was randomized using Excel®. Each patient received two needles, meaning that the acupuncturist carried out 24 interventions in total.
Design of the new double blind acupuncture system:
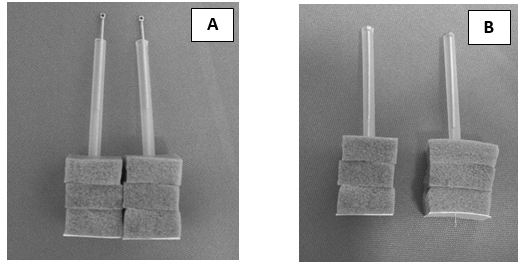
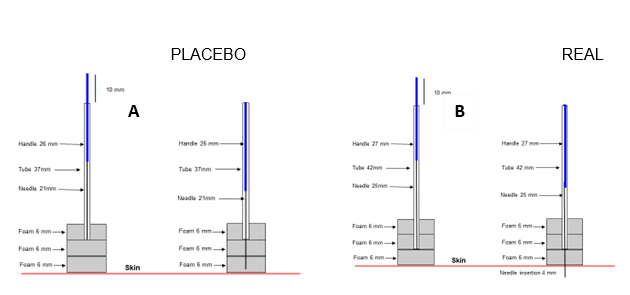
There was no apparent visual difference between the real and the placebo devices. They were made from Wujiang City Cloud and Dragon Medical Device Co. Limited, China 25 x 0.22mm acupuncture needles. The three high-density polyurethane foam pieces used were 13 mm long, 12.7 mm wide, and 6 mm thick (MD brand Georgia, USA), with an adhesive substance on one of their sides, which allowed the acupuncturist to attach the pieces to each other, as well as to adhere the device to the volunteer’s skin in order to apply the acupuncture technique. Both devices were double packed and sterilized using ethylene oxide. The difference between the real and the placebo device is the length of the needle, the length of the tube, and the perforations made on the pieces of foam. The result is two apparently identical devices, as shown in Figure 1A and Figure 2.
Blinding:
All participants were informed that two different acupuncture techniques were being tested. The methods used and the verbal instructions given during the experiment were identical for all the individuals, so as to minimize all possible bias between both methods. The patients were blind to the kind of procedure they were undergoing. To minimize bias, an independent researcher prepared the patients, the needles, and the randomization of the study. The acupuncturist was blind to the kind of device he was using.
Ethical considerations:
The protocol and the consent were approved by the Ethics Committee of the School of Dentistry of Universidad de la República. All participants signed the relevant written consent form.
Real acupuncture technique:
This technique was applied using the device described above. The acupuncture point chosen was the Large Intestine 4 (LI4) bilateral point, one of the most frequently used points in the clinical management of cranial-facial pain. In all cases, the skin was disinfected prior to the procedure with 70% alcohol. The device was inserted into the skin on said acupuncture point by placing the tube in its starting position; the tube served as an insertion guide for the acupuncturist, who then proceeded to insert the needle using the tapping-in method 31. The acupuncturist was instructed to perform all the relevant maneuvers without inserting the needle farther than the initial position. Following this criterion, the tube was removed and the acupuncturist performed the classical acupuncture needle rotation maneuver for 5 seconds. The needle was removed after 30 seconds and the acupuncturist was asked to answer the questionnaire.
Placebo acupuncture technique:
The placebo device was created by removing the tip of a regular needle, which resulted in a shorter, blunt needle. This caused the needle to move only inside the foam pad, which provided a resistance to rotation that was similar to the real resistance without actually coming into contact with the skin. The same technique was used to disinfect the skin, and to insert the device into the volunteer’s skin. The acupuncturist was instructed to use the same stimulation procedure to create the same psychological impact.
All the technical aspects were identical to the real acupuncture technique.
Measurement of variables
Questionnaire:
After withdrawing each needle, the acupuncturists were asked to answer a standard questionnaire with the following questions:
1. What kind of needle do you think you used? Real or placebo.
2. How did you recognize the device?
3. On a 0-100 visual analogue scale, the acupuncturist stated the degree of confidence of their answer to the first question
In the case of Experiment 1, question 1 included the option “I do not know”.
Data analysis
Experiment 1:
The data obtained were subject to statistical analysis using the Fisher Exact Test and the Chi-Squared Test. Statistical significance was accepted for any answer below the 5% level.
Experiment 2:
The data from the 24 interventions were analyzed using the Chi-Squared method. The acupuncturist’s correct identification of the kind of needle was categorized as a correct answer, regardless of the kind of needle. The percentage of successful and unsuccessful answers was calculated for each needle and the confidence interval was calculated for each measurement. The data related to the degree of confidence with which the answers were selected were analyzed using the t-test. The tests were conducted with a 5% significance level.
Results
Experiment 1:
There was no difference between operators in terms of their ability to identify the real needle (p = 0.192). From the 30 needles used, the operators were able to successfully identify 7 (23%). Operator # 1 identified 2/10 successfully, Operator # 2 4/10, and Operator # 3 1/10 (Fig. 3).
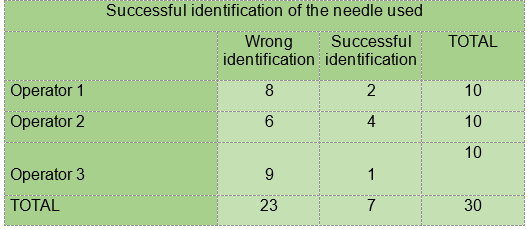
Fig. 3: Results after testing the devices on 3 experienced acupuncturists with 10 interventions each on the same volunteer
Experiment 2:
Table 1: Success rate with the corresponding confidence interval when testing only one acupuncturist with 24 interventions
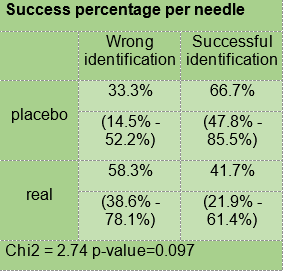
The success percentage according to the kind of needle was higher for the placebo needle (66.7%) than for the real needle (41.7%) with an 18.8 and 19.8 standard deviation, respectively. Additionally, the percentage of wrong answers was 33.3% for the placebo needle, and 58.3% for the real one (Table 1).
Table 2: T-test to analyze the acupuncturist’s degree of confidence in his response to the type of needle
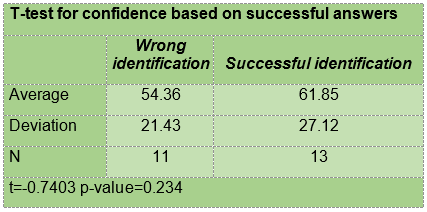
When considering the confidence stated by the operator on the 100 mm visual analogue scale, we found that the average degree of confidence for successful answers was 61.85 (, 27.12 for 13 interventions, while the average for the 11 unsuccessful interventions was 54.36 ( 21.43 (Table 2).
Discussion
Developing a simple, cost-effective, easy-to-produce acupuncture method, with double blinding potential has been a primary objective in this area of knowledge, despite the partial success obtained so far. This study perfected a new placebo acupuncture method initially developed to be used in single blind studies 25, making alterations which make it possible to use it as control in double blind clinical research. The method that was originally presented and the changes assessed in this pilot study sought to improve previously used devices which exhibited several methodological difficulties, mainly because they presented physiological effects that could include biased results. For example, the device developed by Streitberger causes a slight prick on the skin 32-33, and Park’s device is known by acupuncturists, thus making it a single blind device 34 35. Takakura et al. presented a device with double blind potential, which poses the issues of difficult access and high cost, added to the authors’ recommendation to use three different devices for better results, a real one, one which generates pressure on the skin, and one which does not touch the skin 16,28-29.
The first experiment presented here allowed the researchers to assess several acupuncturists and their ability to identify the kind of needle used, thus assessing potential interindividual variability. The results showed that the experienced acupuncturists were not able to tell the real needles from the placebo ones, there being no interindividual differences.
The second experiment sought to assess the degree of success of the same acupuncturist in relation to various patients. The analysis of the success rate based on the kind of needle showed that, despite there being a 66.7% difference for placebo needles and 41.7% for real needles, said percentages do not stray significantly from 50%, which would be the random percentage. Therefore, there is not enough evidence to say that the acupuncturist recognizes the kind of needle used.
Likewise, we found no significant differences when analyzing the degree of confidence on the decision made by the acupuncturist regarding the kind of needle used, the average of said confidence and the deviations in the cases of success and errors. Although the average degree of confidence was higher when the acupuncturist was able to recognize the kind of needle, the sizes of the samples together with the variability observed did not make it possible to assert that the averages were different.
Upon simultaneous consideration of both scenarios, it is not possible to reject the hypothesis that the acupuncturist cannot distinguish between a real needle and a placebo needle.
The device under consideration allows the practitioner to adjust the direction of the insertion of the needle, thus altering the angle from the lower end of the guide tube. Moreover, manipulating the needle with the guide tube makes it possible to establish a safety stop to regulate the depth of insertion of the needle 25. The design also makes it possible to use the device in all acupuncture points, with the sole need to shave the area where the hair may hinder its insertion. This study used a single acupuncture point; it is thus necessary to assess it in other points.
One of the limitations of the device is the fact that the insertion angle and depth are limited by the position of the guide tube. Therefore, it is a useful artificial device for research purposes but it cannot fully reproduce all the conditions of the real practice of acupuncture. Furthermore, it is unclear whether this placebo device presents some kind of activity, for the contact of the adhesive polyurethane foam with the skin and the pressure exerted when activating the device could create some kind of tactile physiological effect, which would be negligible if compared to that of a needle that puts pressure on the skin. Future studies with larger samples and electrophysiological analyses of afferent neuron activity might be able to answer these questions.
Conclusions
The new device here presented showed high potential for blinding the operator, suggesting that it is useful to mask even experienced acupuncturists. These data, together with the previous study that showed an adequate blinding of the patient, confirm the possibility of designing double blind clinical studies.
Acknowledgments
This study was financed by the Sector Committee of Scientific Research and by the School of Dentistry of UdelaR.
Drs. Gustavo Codari and Guillermo Chaibun for their cooperation in experiment I
REFERENCES
1. Ernst E. Acupuncture: A critical analysis. J Intern Med. 2006; 259 (2): 125-137. doi:10.1111/j.1365-2796.2005.01584.x [ Links ]
2. Yang ES, Li PW, Nilius B, Li G. Ancient Chinese medicine and mechanistic evidence of acupuncture physiology. Pflugers Arch Eur J Physiol. 2011; 462 (5): 645-653. doi:10.1007/s00424-011-1017-3 [ Links ]
3. Leung L. Neurophysiological Basis of Acupuncture-induced Analgesia: An Updated Review. JAMS J Acupunct Meridian Stud. 2012; 5 (6): 261-270. doi:10.1016/j.jams.2012.07.017 [ Links ]
4. Cheng KJ. Neurobiological Mechanisms of Acupuncture for Some Common Illnesses: A Clinician's Perspective. JAMS J Acupunct Meridian Stud. 2014;7 (3): 105-114. doi:10.1016/j.jams.2013.07.008 [ Links ]
5. Kaptchuk TJ. Acupuncture?: Theory , Efficacy , and Practice. Ann Intern Med. 2002; 136 (5): 374-83 [ Links ]
6. Schulz K, Douglas AG, Moher D. CONSORT 2010 Statement: Updated Guidelines for Reporting Parallel Group Randomised Trials. Br Med J. 2010; 340:698-702. doi:10.1136/bmj.c332 [ Links ]
7. Lin J-G, Chen C-H, Huang Y-C, Chen Y-H. How to Design the Control Group in Randomized Controlled Trials of Acupuncture? Evidence-Based Complement Altern Med. 2012; 2012: 1-7. doi:10.1155/2012/875284 [ Links ]
8. Vas J, Perea-Milla E, Méndez C, Sánchez Navarro C, León Rubio JM, Brioso M, García Obrero I. Efficacy and safety of acupuncture for chronic uncomplicated neck pain: A randomised controlled study. Pain. 2006; 126(1-3): 245-255. doi:10.1016/j.pain.2006.07.002 [ Links ]
9. Irnich D, Behrens N, Molzen H, König A, Gleditsch J, Krauss M, Natalis M, Senn E, Beyer A, Schöps P. Randomised trial of acupuncture compared with conventional massage and "sham" laser acupuncture for treatment of chronic neck pain. BMJ. 2001; 322 (7302): 1574-1578. doi:10.1055/s-2003-41566 [ Links ]
10. Diraçoglu D, Vural M, Karan A, Aksoy C. Effectiveness of dry needling for the treatment of temporomandibular myofascial pain: A double-blind, randomized, placebo controlled study. J Back Musculoskelet Rehabil. 2012; 25 (4): 285-290. doi:10.3233/BMR-2012-0338 [ Links ]
11. Cho S-Y, Lee D-H, Shin HS, Hwan Lee S, Seok Koh J, Woo-Sang J, Kwan Moon S, Mi Park J, Chang-Nam K, Ho K Park S. The efficacy and safety of acupuncture for cerebral vasospasm after subarachnoid hemorrhage: study protocol for a randomized controlled trial. Trials. 2015; 16 (1): 68. doi:10.1186/s13063-015-0591-7 [ Links ]
12. Liang Z, Zhu X, Yang X, Fu W, Lu A. Assessment of a traditional acupuncture therapy for chronic neck pain: A pilot randomised controlled study. Complement Ther Med. 2011; 19 (SUPPL. 1):S26-S32. doi:10.1016/j.ctim.2010.11.005 [ Links ]
13. Linde K, Streng A, Jürgens S, Hoppe A, Brinkhaus B, Witt C, Wagenpfeil S, Pfaffenrath V, Hammes MG, Weidenhammer W, Willich SN, Melchart D. Acupuncture for patients with migraine: A randomized controlled trial. J Am Med Assoc. 2005; 293 (17): 2118-2125. doi:10.1001/jama.293.17.2118 [ Links ]
14. Kim H-M, Cho S-Y, Park SU, Sohn IS, Jung WS, Moon SK, Park JM, Ko CN, Cho KH. Can Acupuncture Affect the Circadian Rhythm of Blood Pressure? A Randomized, Double-Blind, Controlled Trial. J Altern Complement Med. 2012; 18 (10): 918-923. doi:10.1089/acm.2011.0508 [ Links ]
15. Park J, Kim HS, Lee SM, Yoon K, Kim WS, Woo JS, Lee S, Kim JB, Kim W. Acupuncture antiarrhythmic effects on drug refractory persistent atrial fibrillation: Study protocol for a randomized, controlled trial. Evidence-based Complement Altern Med. 2015;2015. doi:10.1155/2015/613970 [ Links ]
16. Zhang CS, Tan HY, Zhang GS, Zhang AL, Xue CC, Xie YM. Placebo devices as effective control methods in acupuncture clinical trials: A systematic review. PLoS One. 2015; 10 (11): 1-22. doi:10.1371/journal.pone.0140825 [ Links ]
17. Lund I, Näslund J, Lundeberg T. Chinese Medicine. 2009; 9:1-9. doi:10.1186/1749-8546-4-1 [ Links ]
18. Olausson H, Lamarre Y, Backlund H, Morin C, Wallin BG, Starck G, Ekholm S, Strigo I, Worsley K, Vallbo AB, Bushnell MC. Unmyelinated tactile afferents signal touch and project to insular cortex. Nat Neurosci. 2002; 5 (9): 900-904. doi:10.1038/nn896 [ Links ]
19. Olausson H, Wessberg J, Morrison I, McGlone F, Vallbo Å. The neurophysiology of unmyelinated tactile afferents. Neurosci Biobehav Rev. 2010; 34 (2): 185-191. doi:10.1016/j.neubiorev.2008.09.011 [ Links ]
20. Melchart D, Linde K, Streng A, Reitmayr S, Hoppe A, Brinkhaus B, Becker-Witt C, Wagenpfeil S, Pfaffenrath V, Hammes M, Willich SN, Weidenhammer W. Acupuncture Randomized Trials (ART) in patients with migraine or tension-type headache--design and protocols. Forsch Komplementarmed Klass Naturheilkd. 2003; 10 (4): 179-184. doi:73473 [ Links ]
21. Lundeberg T, Lund I, Näslund J, Thomas M. The Emperor's sham - Wrong assumption that sham needling is sham. Acupunct Med. 2008; 26 (4): 239-242. doi:10.1136/aim.26.4.239 [ Links ]
22. Birch S. Sham acupuncture is not a placebo treatment - implications and problems in research. Japanese Acupunct Moxibustion. 2012; 8 (1): 4-8. [ Links ]
23. Park J, White A, Lee H, Ernst E. Development of a new sham needle. Acupunct Med. 1999; 17 (2): 110-112. doi:10.1136/aim.17.2.110 [ Links ]
24. Streitberger K, Kleinhenz J. Introducing a placebo needle into acupuncture research. Lancet. 1998; 352 (9125): 364-365. doi:10.1016/S0140-6736(97)10471-8 [ Links ]
25. Kreiner M, Zaffaroni A, Alvarez R, Clark G. Validation of a simplified sham acupuncture technique for its use in clinical research: A randomised, single blind, crossover study. Acupunct Med. 2010; 28 (1): 33-36. doi:10.1136/aim.2009.001735 [ Links ]
26. Takakura N, Yajima H. A placebo acupuncture needle with potential for double blinding - A validation study. Acupunct Med. 2008; 26 (4): 224-230. doi:10.1136/aim.26.4.224 [ Links ]
27. Kim S. Creating an instrument for a successful double-blind acupuncture placebo. JAMS J Acupunct Meridian Stud. 2008; 1 (1):36-41. doi:10.1016/S2005-2901(09)60005-4 [ Links ]
28. Takakura N, Takayama M, Kawase A, Yajima H. Double blinding with a new placebo needle: A validation study on participant blinding. Acupunct Med. 2011; 29 (3): 203-207. doi:10.1136/aim.2010.002857 [ Links ]
29. Takayama M, Yajima H, Kawase A, Homma I, Izumizaki M, Takakura N. The Potential of Double Blinding with Two Placebo Acupuncture Needles: A Randomized Controlled Pilot-Trial. Medicines. 2014; 2 (1): 11-27. doi:10.3390/medicines2010011 [ Links ]
30. Zhu D, Gao Y, Chang J, Kong J. Placebo acupuncture devices: Considerations for acupuncture research. Evidence-based Complement Altern Med. 2013; 2013. doi:10.1155/2013/628907 [ Links ]
31. Takakura N, Takayama M, Kawase A, Yajima H, Streitberger K. Tapping-in method (Skin Penetration Technique) with a placebo needle for double-blind acupuncture trials. Dtsch Zeitschrift fur Akupunkt. 2013;56 (3): 25-26. doi:10.1016/j.dza.2013.09.008 [ Links ]
32. McManus C a, Schnyer RN, Kong J, Nguyen LT, Hyun Nam B, Goldman R, Stason WB, Kaptchuk TJ. Sham acupuncture devices--practical advice for researchers. Acupunct Med. 2007; 25 (1-2): 36-40. doi:10.1136/AIM.25.1-2.36 [ Links ]
33. Rebhorn C, Breimhorst M, Buniatyan D, Vogel C, Birklein F, Eberle T. The efficacy of acupuncture in human pain models: A randomized, controlled, double-blinded study. Pain. 2012; 153 (9): 1852-1862. doi:10.1016/j.pain.2012.05.026 [ Links ]
34. Park J, White A, Stevinson C, Ernst E, James M. Validating a new sham (placebo) acupuncture device: two randomized controlled trials. Acupunct Med. 2002;20 (2-3): 123-123. doi:10.1136/aim.20.2-3.123 [ Links ]
35. To M, Alexander C. The effects of Park sham needles: a pilot study. J Integr Med. 2015; 13 (1): 20-24. doi:10.1016/S2095-4964(15)60153-4 [ Links ]
Received: July 16, 2018; Accepted: September 03, 2018
 Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
