










Services on Demand
Journal

Article
 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Related links
Share

 Permalink
PermalinkOdontoestomatología
Print version ISSN 0797-0374On-line version ISSN 1688-9339
Odontoestomatología vol.20 no.32 Montevideo Dec. 2018
https://doi.org/10.22592/ode2018n32a5
Investigación
Oral and maxillofacial manifestations in patients with drug addiction
1
 http://orcid.org/0000-0001-8230-1074
http://orcid.org/0000-0001-8230-1074
2
http://orcid.org/0000-0003-1621-4516
3
http://orcid.org/0000-0001-8511-1954
4
http://orcid.org/0000-0003-0538-5096
1Área de Clínica y Patología. Instituto de Investigaciones. Facultad de Odontología. Universidad del Zulia. Maracaibo. Venezuela. neirach@yahoo.com
2Área de Epidemiología y Práctica Odontológica. Instituto de Investigaciones. Facultad de Odontología. Universidad del Zulia. Maracaibo. Venezuela
3Instituto de Investigaciones. Facultad de Odontología. Universidad del Zulia. Maracaibo. Venezuela
4Instituto de Investigaciones. Facultad de Odontología. Universidad del Zulia. Maracaibo. Venezuela
5Instituto de Investigaciones. Facultad de Odontología. Universidad del Zulia. Maracaibo. Venezuela
6Instituto de Investigaciones. Facultad de Odontología. Universidad del Zulia. Maracaibo. Venezuela
Abstract: The aim of this research was to characterize oral and maxillofacial manifestations in patients addicted to drugs. A descriptive field study was conducted. Thirty-two individuals attending voluntarily a rehabilitation center located in Zulia State, Venezuela, were selected. A survey and a clinical examination were conducted to determine the oral and maxillofacial manifestations. The average age of the subjects was 37.7, most of them being male. The most commonly used drugs were crack, followed by cocaine and marijuana. Regarding oral manifestations, the predominance of caries (87.5%) was observed, followed by the presence of signs of periodontal disease. These findings point to the poor oral care of the drug-dependent subjects, which increases the risk of infectious processes, loss of dental organs, decrease of all functions and therefore leads to the deterioration in quality of life.
Keywords: street drugs; oral manifestations
Palabras clave: Drogas ilícitas; manifestaciones bucales
Introduction
The World Health Organization (WHO) has defined the term drug of abuse as a substance used for non-medical purposes with psychoactive effects, capable of being self-administered, which can result in changes in perception, mood, consciousness and behavior1. The short-term sensations or effects associated with drug abuse in connection with health in general are well known and include tiredness, nausea, hallucinations, chills, sweating, increased body temperature, tremors, muscle cramps, blurred vision and anxiety, among others. In combination with this, chronic use of these substances can also have indirect consequences on family life and society as a whole, such as lower self-esteem, lack of motivation, reduced productive working time, and increased violence and crime rates 2.
Drug abuse is one of the most devastating health problems in the world3. According to the United Nations Office on Drugs and Crime, globally, it is estimated that 243 million people aged 15 to 64 have used an illicit drug4, with Iran being the country with the highest numbers of drug use, followed by China, the United States and Russia2; and approximately 5,000 drug-related deaths are reported every year in Latin America and the Caribbean alone4.
Drugs of abuse cause physical and mental problems such as cardiac crisis, respiratory depression, liver cirrhosis, nephropathy, infectious diseases such as hepatitis, AIDS, and tuberculosis, and can also cause disability and mental disorders such as depression. These conditions can progress to advanced stages and can cause significant complications because addicted patients delay seeking medical care and do so when they experience severe symptoms2.
Moreover, these substances can also directly affect dental tissue and oral mucosa, and can also cause xerostomia, alterations in salivary flow, enamel erosion and abrasion, atypical caries, tooth loss 2) and periodontal disease 5; alterations which have been mainly associated with the type of drug and duration of use 6. It has been reported that patients who suffer from addiction to these substances can have a higher caries incidence, possibly due to the combination of multiple factors such as increased consumption of refined carbohydrates7, especially sugar, which they tend to consume periodically while administering the drug3. Recent studies describe the presence of a greater amount of biofilm and, consequently, of dental caries in cervical areas as a pathognomonic sign of abuse of certain drugs8.
It has also been reported that regular use of some substances such as cocaine may have severe orofacial effects, such as perforation of the nasal septum and palate, gingival lesion and erosion of the tooth surface, and it is also associated with changes in the sense of smell and chronic sinusitis 5. Moreover, smoking crack and cocaine produces burns and sores on the lips, face, and inside the oral cavity2.
The existing information on oral and maxillofacial alterations in patients addicted to drugs is not very extensive. In Venezuela, and especially in Zulia state, the available data are scarce, which is why there is no oral profile of the patients affected by this disorder and, therefore, no health policies on this social reality. Thus, the purpose of this research was to characterize oral and maxillofacial manifestations in patients addicted to drugs attending rehabilitation centers.
Methodology
An observational, descriptive, field study was conducted on a population comprising all the patients attending a rehabilitation center for drug-addicts, located in Zulia State, Venezuela. The sample was selected using the intentional, non-probabilistic sampling technique, according to the following inclusion and exclusion criteria:
Inclusion criteria:
Individuals of both sexes, of legal age, who voluntarily agreed to participate in the study and were attending the rehabilitation center for using one or several types of drugs for a period longer than one month, using any administration route, combined or not with tobacco and alcohol use.
Exclusion criteria:
Patients with behavioral problems or a state of immunosuppression, and pregnant women were excluded.
Thus, the sample was finally formed by 32 individuals.
To comply with bioethics rules and the agreements set forth in the Helsinki Declaration, all the participants considered were instructed on the purposes and scope of the research, asking each of them for their written consent to be included in the study. An anonymity agreement was also established, according to bioethics criteria, both for the identity of each participant and for the rehabilitation center.
The data were collected with the survey method, using an information collection instrument designed for this purpose administered by the research team. The data collected included personal details, medical and dental history, and information connected to their drug habits: substance(s) used, duration of use and most frequently used administration route(s).
The direct observation method was used to determine the oral and maxillofacial manifestations present in the patients addicted to drugs considered, through an extraoral and intraoral clinical examination conducted by a single, previously-calibrated (Kappa coefficient 0.9) examiner, specialized in Oral Medicine and experienced in the diagnosis of oral and maxillofacial lesions, following the parameters established in the World Health Organization Oral Health Surveys 9.
In this way, we recorded clinical alterations in soft and/or hard tissue, major salivary glands, cervical lymph node chains, temporomandibular joint disorders, alterations in the skin of the face and neck, malformations and facial asymmetries, and consequences of conditions in the maxillofacial area. Changes in color, shape, size and structure of dental organs, and changes in color, size, consistency or function of the soft tissues that form the oral cavity were also observed, the presence of dental caries and clinical signs of periodontal disease, as well as harmful oral habits, were recorded.
The SPSS statistical analysis computerized system version 22.0 was used for statistical processing. Elements of descriptive statistics, measures of central tendency and dispersion were used to analyze the information. Pearson’s correlation test (given a 95% confidence level) was used to determine whether there is a relationship between the number of missing teeth and the duration of drug use.
Results
Once the data on oral and maxillofacial alterations in patients addicted to drugs attending the study center were collected, it was found that the average of the subjects considered was 37.7 ± 10.0 years old, with a difference of 46 years between the youngest and the oldest individuals in the sample. However, the largest proportion of patients was found in the 25-35 age group and the 36-45 age group (34.4%, respectively), followed by the 46-55 age group (18.8%); most of them being male (81.3%), in a 1:4.3 relation.
Chart 1: Characteristics of drug use in the studied population. Zulia State. 2015
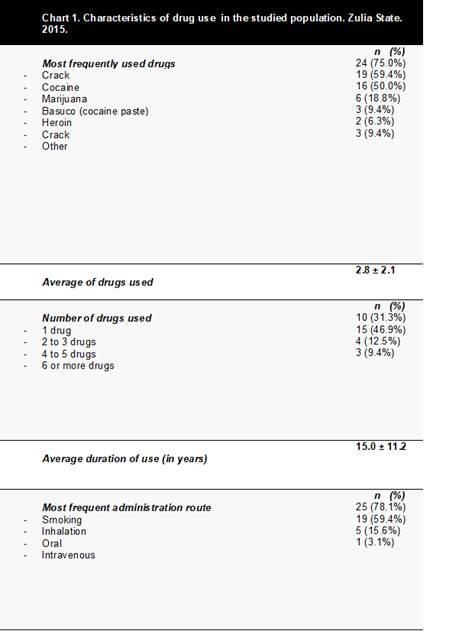
Source: data collection instrument.
As for the characteristics of the drug use (Chart 1), it was found that the most frequently used drugs were crack, followed by cocaine and marijuana, and the average duration of use reported by patients was 15.0 ± 11.2 years. The mean number of drugs used was 2.8 ± 2.1 substances, since almost half of the individuals considered reported using 2 to 3 different drugs simultaneously. The most frequent administration route was smoking, followed by inhalation. The largest proportion of the sample reported using tobacco and alcohol along with drugs.
Regarding maxillofacial manifestations, adenopathies were found in the cervical lymph node chains in 4 of the patients examined (12.5%), increases in parotid gland volume in 2 subjects (6.3%), absence of salivary secretion during gland stimulation at the time of examination in 7 individuals (21.9%) and facial asymmetry in 6 patients (18.8%).
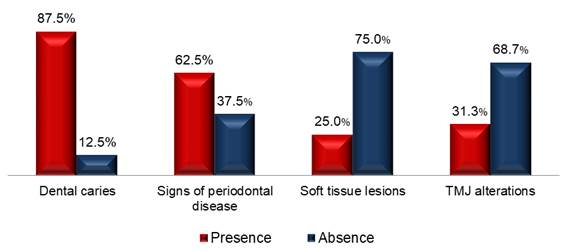
Regarding oral manifestations detected in the intraoral examination (Graph 1), the most frequently found alteration was dental caries, followed by signs of periodontal disease. To analyze the extent of the impact of dental caries, the average number of decaying teeth, teeth missing as a result of caries and filled teeth was determined (Graph 2), and a predominance of missing teeth was found. Pearson’s correlation test (given a 95% confidence level) was also used to determine whether there is a relationship between the number of missing teeth and the duration of drug use, a moderate, statistically significant (p= 0.005), positive correlation was found (r = 0.581).

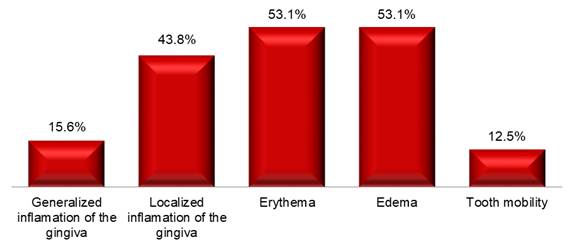
Finally, when discriminating the signs of periodontal disease found most frequently (Graph 3), a predominance of erythema and edema was found. An assessment of the presence of harmful oral habits in the sample analyzed showed that 59.4% had bruxism, and the second most common one was nail biting (37.5%).
Discussion
As shown by the previously reported results, the deterioration of oral health is one of the most frequently found problems in drug-abusing patients. This deterioration could be explained by multiple factors, for example, direct exposure of oral tissue to these substances, the interaction of drugs with the normal physiology of the oral cavity, an increase in the consumption of refined carbohydrates which are usually consumed periodically while taking the drug and associated smoking in addicts 2,7.
As for the distribution of patients with drug addiction by sex and age, numerous publications have reported that users of illegal drugs are most frequently male, aged 15 to 64, with a mean age of 34 years 4,10-12. However, groups of methamphetamine and heroin users under 30 years of age have been found10. This research showed consistency with the studies mentioned regarding the sex and mean age (37.7 years); however, the lower boundary of the age range was 18 because individuals younger than 18 were excluded from this study because there was no authorization from their legal representatives when the information was collected. Nevertheless, it was not possible to compare the results regarding age and heroin or methamphetamine use, since the latter was not found among the drugs used by the group studied.
A comparison of the results obtained from findings reported in the literature in connection to the most commonly used drugs showed significant differences, since crack was the most frequently used substance in the sample analyzed, whereas methamphetamine and marijuana are in the first positions in other studies. This finding could be explained by the fact that the effects of inhaling crack are practically immediate, since it enters the bloodstream quickly, giving users a feeling of euphoria, panic, insomnia and the need to take crack again, which makes it a popular drug among addicts. Moreover, processing and acquiring this substance is less expensive, which means it is easier to use4,10.
Drug addicts may only use one type of drug or a combination of different substances4,10. More than half the subjects included in this research stated that they use two or more drugs. Although the reasons for combining them are varied, users mostly do this to counter the effects caused by one of them, as well as to complement, improve or extend its effects and achieve new ones. For example, the combination of alcohol and cocaine produces cocaethylene in the bloodstream, which is more toxic than the original substances, has additional euphoric effects and is metabolized more slowly than cocaine alone13. According to the scientific literature, most drug users are also smokers and smoke at least one pack of cigarettes a day10. Almost all the addicted patients in this study were also smokers who smoked an average of 28.7 cigarettes a day.
As for the most frequent administration route, it was found that the preferred form of use was smoking, which is consistent with the most used type of substance in this study. These findings differ from studies conducted in Switzerland where the most frequent administration route were injection, followed by inhalation, which is consistent with the drugs most commonly used in that geographical location10,12.There might be a relationship both between administration route and type of drug used with the socioeconomic status of consumers since, even though this variable was not studied, individuals reported having a preference for the least expensive substance.
In the analysis of the findings obtained regarding oral manifestations in drug-addicted patients, the results of most frequent conditions in oral hard tissues, in which dental caries prevailed, are consistent with those reported by Basov et al., who also found a high prevalence of caries in drug-dependent individuals (similar to the prevalence reported in this study). The susceptibility of drug addicts to having caries has been intensively described in the scientific literature by different authors, who have linked its etiology with several of these people’s lifestyle factors 4,10,14,15, among which the most relevant are a marked tendency to consume refined carbohydrates7 combined with poor oral hygiene and salivary hypofunction typical of these patients, aside from limited access to health services, all of which creates a favorable environment for the formation of plaque and possibly dental caries16.
Likewise, the average number of teeth affected by dental caries (decayed, missing as a result of caries and filled) was consistent with the results reported in a study on the dental profile of a community of recovering drug addicts 7 conducted in Spain; both studies found a predominance of missing teeth as a consequence of dental caries in this population. Additionally, this study found a statistically significant correlation between the number of teeth missing and the duration of drug use, which shows that, logically, as the duration of drug use increases, the number of teeth missing increases.
Although the literature describes a pattern of atypical caries in the cervical region of the tooth caused by the abuse of some drugs, which is even described as a pathognomonic sign of the abuse of certain drugs3,7, only 21.8% of patients in this study had caries in the cervical third, which could be due to the fact that the main drug that causes this pattern of caries is methamphetamine5,10, and this drug was not used by the population studied.
Regarding the signs of periodontal disease (second most frequently found oral manifestation in the population considered), previous publications have indicated that gingival bleeding, periodontal attachment loss and the deposit of cervical plaque in or more teeth, are common findings in drug addicts5, which makes periodontal disorders, such as supporting tissue disease, the most prevalent in these patients2, which is consistent with the findings of this study. In addition, Brand et al. reported that oral administration of cocaine in particular can cause gingival lesions in the application site, gum retraction, sores, edema and erythema, as well as pain and inflammation symptoms. However, no lesions of this kind caused by the application of cocaine on gums were found in this study; although gingival edema and erythema were found in association with the sites where the crack pipe is placed17.
Finally, the literature reports that users of drugs such as cocaine, methamphetamine and opiates suffer from bruxism, which results in a higher frequency of temporomandibular joint (TMJ) disorders, cuspal inclinations and dental wear. Winocur et al. claim that the abuse of drugs makes the oral motor parafunction worse, and prior clinical reports showed severe bruxism, myofascial pain, chewing motions and friction of the tongue among drug users2,3,10. Therefore, the findings reported in this study regarding harmful oral habits are consistent with the presence of bruxism, though the assessment of the TMJ showed no alterations in the joint.
Conclusion
These findings point to the poor oral care of drug-dependent subjects since, even though no significant maxillofacial alterations were observed, a high prevalence of dental caries followed by periodontal disease was found. This increases the risk of infectious processes, loss of dental organs, decrease of all functions and therefore leads to the deterioration in quality of life
Referencias
1. World Health Organization. WHO Expert Committee on Drug Dependence - WHO Technical Report Series, No. 915 - Thirty-third Report. Geneva: ONU. 2003. [ Links ]
2. Shekarchizadeh H, Khami MR, Mohebbi SZ, Ekhtiari H, Virtanen JI. Oral Health of Drug Abusers: A Review of Health Effects and Care. Iran J Public Health. 2013; 42 (9): 929-940. [ Links ]
3. Rees T. Oral Effects of Drug Abuse. Crit Rev Oral Biol Med. (1992); 3 (3):163-184. [ Links ]
4. Marques TC, Sarracini KL, Cortellazzi KL, Mialhe FL, de Castro Meneghim M, Pereira AC, Ambrosano GM. The impact of oral health conditions, socioeconomic status and use of specific substances on quality of life of addicted persons. BMC Oral Health. 2015; 15: 38. [ Links ]
5. Saini GK, Gupta ND, Prabhat KC. Drug addiction and periodontal diseases. J Indian Soc Periodontol. 2013; 17 (5): 587-591. [ Links ]
6. Hadzic S, Dedic A, Gojkov-Vukelic M, Mehic-Basara N, Hukic M, Babic M, Beslagic E. The effect of psychoactive substances (drugs) on the presence and frequency of oral Candida species and Candida dubliniensis. Mater Sociomed. 2013; 25 (4): 223-225. [ Links ]
7. Mateos-Moreno MV, Del-Río-Highsmith J, Riobóo-García R, Solá-Ruiz MF, Celemín-Viñuela A. Dental profile of a community of recovering drug addicts:Biomedical aspects. Retrospective cohort study. Med Oral Patol Oral Cir Bucal. 2013; 18 (4): e671-679. [ Links ]
8. De-Carolis C, Boyd GA, Mancinelli L, Pagano S, Eramo S. Methamphetamine abuse and »,» ®,® §,§ ­, ¹,¹ ²,² ³,³ ß,ß Þ,Þ þ,þ ×,× Ú,Ú ú,ú Û,Û û,û Ù,Ù ù,ù ¨,¨ Ü,Ü ü,ü Ý,Ý ý,ý ¥,¥ ÿ,ÿ ¶,¶ meth mouth »,» ®,® §,§ ­, ¹,¹ ²,² ³,³ ß,ß Þ,Þ þ,þ ×,× Ú,Ú ú,ú Û,Û û,û Ù,Ù ù,ù ¨,¨ Ü,Ü ü,ü Ý,Ý ý,ý ¥,¥ ÿ,ÿ ¶,¶ in Europe. Med Oral Patol Oral Cir Bucal. 2015; 20 (2): e205-210. [ Links ]
9. World Health Organization. Oral Health Surveys: Basic Methods. Fifth Edition. Ginebra: WHO Press; 2013. 137p. [ Links ]
10. Brown C, Krishnan S, Hursh K, Yu M, Johnson P, Page K, Shiboski CH. Dental disease prevalence among methamphetamine and heroin users in an urban setting: a pilot study. J Am Dent Assoc. 2012; 143 (9): 992-1001. [ Links ]
11. Shekarchizadeh H, Khami MR, Mohebbi SZ, Virtanen JI. Oral health behavior of drug addicts in withdrawal treatment. BMC Oral Health. 2013; 13:11. [ Links ]
12. Bodmer M, Enzler F, Liakoni E, Bruggisser M, Liechti ME. Acute cocaine-related health problems in patients presenting to an urban emergency department in Switzerland: a case series. BMC Res Notes. 2014; 7:173. [ Links ]
13. Grov C, Kelly BC, Parsons JT. Polydrug use among club-going young adults recruited through time-space sampling. Subst Use Misuse. 2009; 44(6):848-864. [ Links ]
14. Titsas A, Ferguson MM. Impact of opioid use on dentistry. Aust Dent J. 2002; 47(2):94-98. [ Links ]
15. Cho CM, Hirsch R, Johnstone S. General and oral health implications of cannabis use. Aust Dent J. 2005; 50 (2): 70-74. [ Links ]
16. Ma H, Shi XC, Hu DY, Li X. The poor oral health status of former heroin users treated with methadone in a Chinese city. Med Sci Monit. 2012; 18(4):PH51-55. [ Links ]
17. Brand HS, Gonggrijp S, Blanksma CJ. Cocaine and oral health. Br Dent J. 2008; 204 (7): 365-369. [ Links ]
Received: April 02, 2018; Accepted: August 15, 2018
 Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
