










Servicios Personalizados
Revista

Articulo
 texto en
texto en  Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
Links relacionados
Compartir

 Permalink
PermalinkOdontoestomatología
versión impresa ISSN 0797-0374versión On-line ISSN 1688-9339
Odontoestomatología vol.18 no.28 Montevideo nov. 2016
Food consumption during school playtime: survey design and validation
Moncunill, Irma Alicia*, Bella, Marcela**, Cornejo, Lila Susana***
* PROCON Researcher. Professor. Evolutive Psychology Department. School of Dentistry, Universidad Nacional de Córdoba. Argentina.
** Associate Professor. Preventive and Community Dentistry II Department. School of Dentistry, Universidad Nacional de Córdoba. Argentina.
*** PROCON Researcher. Professor Cellular Biology B Department. School of Dentistry, Universidad Nacional de Córdoba. Argentina.Abstract
Objective: To develop and validate a diagnostic tool for food consumption patterns in children’s school playtime to contextualize health-promotion strategies. Method: The content was developed according to information obtained with other instruments in this context. The iconographic format was prioritized in the options. Validation included a panel of experts, a validity of field test and Cronbach alpha coefficient.
Results: The instrument was modified by removing a question of desirability bias and the spatial distribution of icons and words to avoid reiteration bias; we added new products, suggested by the panel of experts. The children of the first school cycle showed difficulty in the reading comprehension of slogans, which they overcame by modifying the font and the way the test was applied, thus giving greater viability to the test.
Conclusion: The application of an instrument to survey food habits adapted to the psycho-cultural-cognitive potential of respondents provided a valid diagnosis to design contextualized health-promoting strategies. Adapted to the age and educational level of respondents.
Keywords: Food preferences, Food habits, Food consumption, Children.
Received on: 15 Mar 16 - Accepted on: 04 Aug 16
Introduction
Collective Health contributes to the study of health, diseases and health care as social processes. It studies disease production and distribution in society as part of social reproduction, analyzing them in the context of health care practices. In its practice field, it focuses on the policies, practices, technologies and tools relevant for an intervention (1).
In order to understand and explain the problems in the field of health care, Minayo (2) states that several viewpoints are needed, including historical, contextual, structural and relational aspects, regularities, singularities and, broadly speaking, the interventions and interpretations of individuals in their production of reality.
Thus, in order to study food habits it is important to consider the conditioning factors that underlie practices and the meaning individuals attach to them.
Several studies report on the interrelation between nutrition and oral health (3). Oral health and medical conditions with oral manifestations may be associated to nutritional deficiencies and the cariogenic nature of certain foods (4). So can mastication and deglutition dysfunctions with symptoms of discomfort and pain. We must take an interdisciplinary approach to address these aspects of the health-disease process associated to eating habits, so as to study them not only as epidemiological variables, but also as complex bioecological and sociocultural processes.
In trying to broaden the spectrum in health care studies, Arnaiz (5), among other authors, draws a correlation between the current deterioration of food habits and sociocultural factors.
Advertising and availability of “supply” also determine and restrict people’s “food choices”, even long before we are able to consciously consider them (6).
Food consumption is tied to the cultural patterns developed by individuals in each social context, therefore, the diagnostic tools to be used need to be designed with these contexts in mind. The research conducted by our interdisciplinary team confirms this (7, 8), and is concurrent with the latest studies (9) which report that any initiatives undertaken with children, families and schools should not merely focus on information sharing but rather on the problematization and consideration of the options and conditioning factors of the everyday environment.
Additionally, our current lifestyle and globalization not only undermine cultural food diversity but have also made “junk food” consumption a widespread free-time activity, for example during school playtime. This has led authors as Fischler (10) to speak about “snacking” when referring to informal meals, considering “gastro-anomie a concept to describe modern societies from a sociological standpoint”.
The concept of “snacks or refreshments” is associated to the time and place of consumption. The main characteristic of these foods is that they are consumed in short periods lasting 15 minutes at most. This consumption occurs in a non-formal eating context.
Candy is featured as the main snack for children. From an anthropological standpoint, it is acknowledged as a product mainly for children, which is usually consumed away from regular meal times and not normally considered nutritious by general standards (11).
Although the current trend is to seek information about food ingredients, this does not seem to include the candy children usually eat during school playtime and, in many cases, this information is not even available in the package label, even though there are provisions in place which require so.
The subliminal messages in the advertisements we see in the media, whose target population is children, reinforce candy consumption by focusing on the social and emotional aspects that trigger feelings of enjoyment when consuming these products.
Unlike in other MERCOSUR countries where there are policies and regulations addressing healthy eating in school premises, there are no provisions for food consumption during school playtime in the city of Córdoba, Argentina. The sale of candy or sweets is not regulated for school premises or nearby areas.
Although Ministries and National, Local and Municipal Education Boards have recently implemented school programs to modify eating habits during playtime, these either did not survive over time or did not reach all the schools nationwide (11, 13).
Moreover, there is inconsistency between the cariogenic and non-cariogenic child nutrition discourses promoted by teachers and the actual food consumption patterns fostered by the institution through the school kiosk. This was observed in the interviews with elementary schools teachers during the focus groups initially conducted as part of the situation assessment:
“There is great discrepancy: we are like God and the Devil at the same time. We tell them not to eat candy but we sell lollipops” (teacher M).
“But we still face the same problem: children bring their own candy from home, so the problem doesn’t lie in the school kiosk alone” (teacher L).
Health promotion is a complex practice that requires knowing and respecting the logic, times, priorities, meanings and cultural health practices, which are all unique to every social context. Thus, in order to design contextualized health promotion strategies that are linked to food habits, it is necessary to use diagnostic tools that are customized to the psycho-cognitive and cultural characteristics of the communities they target. Among the many data collection methods used in research, participant observation, interviews and surveys are the most relevant. The latter allow us to reach a wider audience and facilitate data analysis (14). It is important to differentiate the rating scales when we speak about surveys. They allow for an incremental scaling of the items, assigning global scores by the end of the evaluation. Conversely, data collection surveys, symptom inventories, standardized interviews and forms do not have an incremental nature: these merely collect data without assigning ratings (15).
The design and validation of an instrument to address food habits during school playtime became necessary in our attempt to overcome certain weaknesses identified by our research team (7, 8) in previous studies undertaken with school-age children. The surveys used in those studies explored the frequency of carbohydrate intake and recollection of sugar consumption.
Within the framework of a contextualized health promotion initiative, we have set out the objective to design and validate a collective diagnostic instrument on food consumption habits during school playtime to contextualize health promotion strategies that are linked to eating habits. Based on our target population and implementation context, we decided that a data collection survey was the most suitable tool for this purpose.
Method
A total of 240 children aged 6-13 were surveyed in 2010 at the Professor Miguel Luciani School in the neighborhood of Barrio Ramón J. Cárcano in the city of Córdoba, Argentina (south-east area). Their parents and/or guardians signed an informed consent and agreed for their children to take part in the survey.
To design and validate the contextualized survey we contemplated feasibility, reliability and validity of content with the following procedure (15-17).
Purpose of the survey
- • Inquire about school children’s preferences and food consumption patterns during school playtime.
- • Identify differences between actual and desired snack consumption during school playtime.
Survey feasibility forecast
The questions and instructions were designed based on the respondents and adapted to the cognitive and reading comprehension level of school-age children.
Slogans were purposely short and concise and printed in lower case. An iconographic format was selected over written text for the content of the multiple choice options.
To simplify the administration, instructions were drafted so as to allow for self-administration in groups no larger than 30 children working at once.
Structure and content
The original survey comprised a section to record demographic data and five questions about nutrition.
Regarding answer format, one question followed a YES/NO dichotomous pattern and the other four were multiple choice answers; three of them were in iconographic format (Fig. 1) and one had written text. (Fig. 2).
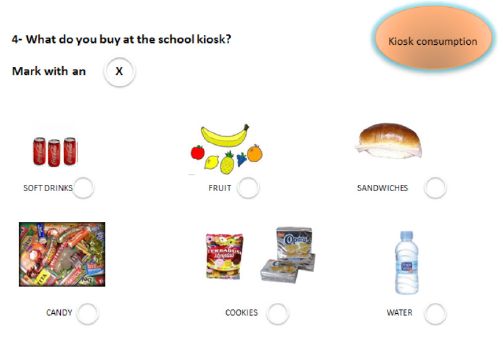
The selection of answers included items known to be consumed by the children in the same research context, based on the information previously obtained with other methods (surveys to parents, photographs of the products sold in school premises and/or nearby, participants observations of food consumption during school playtime, classification and analysis of food leftovers and containers found in school trash cans). Simple scoring was used for answer coding.
The questions were presented following the logical time and place sequence order of the eating behaviors children display during the hours spent in school premises, focusing on playtime and the school kiosk.

Validation
Validation included a panel of experts, field and pilot tests, Cronbach’s alpha was used to measure survey reliability.
Panel of experts
The survey was assessed by health care professionals (educators, biologists, psychologist, dentists and nutritionists) and elementary school teachers. The experts issued recommendations in terms of survey form, structure and content, based on their own area of expertise.
Field test
It was conducted with children from Professor Miguel Luciani School, subject to prior authorization from the school and informed consent signed by parents. The survey was administered to 30 children of both sexes, randomly selected (five per class) based on the order listed in the attendance register: students with an uneven number were selected. Children from the first (6 to 8 years old) and second (9 to 13 years old) school cycle took part in the survey. An observer recorded user behaviors in a field notebook as they answered the survey. The children who took part in this initial validation phase were later excluded from the student sample surveyed in the pilot test.
Pilot test
With the prior authorization of school authorities, the survey was administered to 240 students aged between 6 and 13, of both sexes, at Professor Miguel Luciani School. It was administered in writing, answered individually and simultaneously in groups of 30 to 35 students. A time slot of 40 minutes was allocated for each group within school hours. The test was administered by 4 surveyors, previously calibrated with the help of the teacher in charge of each grade and the observer who developed the field book.
The foods mentioned in student answers were later classified according to the different food groups under the “Food Guidelines for the Argentinean Population” (18), which provides tools to promote healthy and nutritious behaviors using graphs and providing practical advice. The pictures show local foods, very familiar to most Argentineans. In addition, the diet is based on the traditions and food availability in our country.
Reliability
Cronbach’s alpha was used to assess survey reliability based on the results of the pilot test.
Analysis and discussion of the results
Panel of experts validation
The teachers who were part of the panel of experts suggested slogans should be written in printed lower case to make it easier for children to understand the text. Length, clarity and accuracy of the slogans were considered appropriate and the estimated time for survey completion was 15 minutes.
The participating health care professionals suggested including, among the potential answers, water and other food products (bread, biscuits, fruit) made available by the institution at the school cafeteria, as these were set aside by some children to be consumed during school playtime. In addition, some items were renamed based on cultural patterns and the name under which the product was available.
Field test
The test was conducted in the classroom, following the usual seating arrangement and during the time authorized by the institution for this purpose.
An observation log was kept on children’s willingness or refusal to participate, length of the survey, time used to answer the slogans and difficulties that children in the different school grades faced.
In terms of question consistency and understanding, oral instructions were necessary for clarification.
Regarding test length, reading comprehension difficulties were reported in first grade groups (6 years old). Since understanding took up an excessive amount of time, text format was then changed and block capital letters were used instead.
Since the food icons presented in black and white to avoid color influences posed some difficulties, the name of each item in block capital letters was presented next to the icons to aid children’s understanding.
To control potential information biases, such as central tendency, spatial distribution of the options was arranged with no vertical or horizontal justification. The layout of the response options was also modified as they were grouped in word columns. The new spatial distribution design was balanced on both sides of the diagram.
Food icons that were repeated in more than one question as potential answers were re-arranged in different places to avoid reiteration bias.
Pilot test
Although the redesigned test was administered, showcasing block capital letters instead of lower case, observers still reported difficulties for children to understand and answer the questions in the 6-8 age group. The difficulties observed in younger children promoted the implementation of two administration modalities based on the age of the children:
a) Individual oral administration for children aged 6 to 8.
b) individual written self-administration for children 9 to 13, administered in groups no larger than 30 children working at once.
Although a visual icon representation of money was presented on the question about the amount of money children bring to spend at the school kiosk, children were not able to identify in their answers the difference between the actual money spent and the desired amount to purchase products. This information was later confirmed by cross-checking survey answer results against the observations of their behaviors as school kiosk patrons. Due to the lack of consistency in the results, the question was later removed based on desirability bias.
The analysis of the responses showed that 96.25 % of the children consume products during school playtime, 14.71 % bring snacks from home, 17.84 % purchase snacks before coming to school, 31.60 % purchase snacks in the school kiosk and 6.06 % are treated to snacks by classmates. In 29.79 % of cases there is a combination of options. The foods mentioned in the answers were then classified based on the food groups under the “Food Guidelines for the Argentinean Population” (18). In terms of the type of foods consumed during school playtime, the types more commonly observed were under the sugars and sweets group (76 %), followed by: cereals and cereal products (8 %), edible fats and oils (6 %), dairy products (6 %) and fruit (4 %) in contrast, what children reported enjoying the most was sugars and sweets (29 %), cereals (17 %), dairy products (13 %), fruit (12 %) and edible fats and oils (6 %).
Based on the DAILY FOOD INTAKE graph under the “Food Guidelines for the Argentinean Population” (18) and food cariogenic potential, the consumption preference profile is healthier than the actual consumption profile. The differences between actual and preferred consumption show that food consumption is determined by the interplay of several factors, especially advertising, which drives not only preferences but also supply and demand (19).
As financial and sociocultural factors influence food consumption, it is necessary to study them more thoroughly in order to develop intervention strategies to promote healthier food consumption patterns during school playtime.
Reliability
As Cronbach’s alpha was 0.909, we can say that the instrument designed was consistent, as it surveys information with a high reliability level.
Conclusion
The diagnostic survey on children food consumption during school playtime herein was used in a participative research project (20), and the results obtained set the baseline for the design on nutritional strategies customized to the specific context.
Regarding food patterns, we consider that both the attribution of new significances as well as the adoption of food consumption patterns during school playtime require contextualized and validated diagnostic instruments that can provide data to be used as input to design interdisciplinary strategies for health promotion.
Co-authors
IA Moncunill participated in the original idea and structure of this paper. IA Moncunill, MI Bella and LS Cornejo participated in writing, reviewing and approving the version for publication.
References
2. De Souza Minayo MC. Editorial: Interdisciplinariedad y pensamiento complejo en el área de la salud. Salud Colectiva, Buenos Aires Abril 2008; 4 (1): 5-8.
3. Quiñónez Ybarra ME, Rodríguez Calzadilla A, González Cabrera B, Padilla González C. Morbilidad bucal: Su relación con el estado nutricional en niños de 2 a 5 años de la Consulta de Nutrición del Hospital Pediátrico Docente de Centro Habana. Rev Cubana Estomatol [revista en la Internet]. 2004 Abr [citado 2012 Mar 19] ; 41(1): Disponible en: http://scielo.sld.cu/scielo.php?script=sci_arttext&pid=S0034-75072004000100001&lng=es.
4. Aguzzi A, Dorronsoro de Cattoni S. Patrones de consumo de carbohidratos y salud bucodental en niños de diferentes estratos socioeconómicos. Práctica Odontológica 1999. 20: 6-16.
5. Gracia Arnaiz M. Qué y cuánto comer: tomando medidas frente a las sociedades obesogénicas. Salud Colectiva 2009; 5(3):363-376.
6. Patel Raj. Obesos y famélicos. Buenos Aires, Marea, 2008 citado por Piaggio L, Concilio C, Rolón M, Macedra G, Dupraz S. Alimentación infantil en el ámbito escolar: entre patios, aulas y comedores Salud Colectiva 2011; 7 (2): 199-213.
7. Cornejo L, Hilas E, Moncunill I. Integración de las dimensiones clínico-odontológicas sialoquímicas, microbiológicas, físico ambientales, nutricionales y socioculturales para el diseño de estrategias de promoción de salud bucal. Claves en odontología 2003; 53:8-12.
8. Cornejo L S, Moncunill I , Hilas E. Una Estrategia diferente en la promoción de la salud bucal. Claves en Odontología 2007; 60:55-59.
9. Piaggio L, Concilio C, Rolón M, Macedra G, Dupraz S. Alimentación infantil en el ámbito escolar: entre patios, aulas y comedores Salud Colectiva 2011; 7 (2): 199-213.
10. Fischler C. Gastro-nomía y gastro-anomia: Sabiduría del cuerpo y crisis biocultural de la alimentación contemporánea. En: Contreras Hernández J, compilador. Alimentación y cultura. Necesidades, gustos y costumbres. Barcelona: Universitat de Barcelona; 1996.
11. Jakson P, Romo M, Castillo M, Castillo Durán C. Las golosinas en la alimentación infantil. Análisis antropológico nutricional. Rev. Méd Chile 2004; 132:1235-1242.
12. CESNI (Centro de estudios sobre nutrición infantil). Kioscos Saludables, Citado 04/08/2016 Disponible en: www.fmed.uba.ar/depto/nutri_saludpublica/.../8%20Kioscos-Saludables.CESNI.pdf
13. Argentina, Córdoba. Subsecretaría de estado de promoción de igualdad y calidad de la educación. Educación Alimentaria y Nutricional Saludable. Citado 04/08/2016. Disponible en: http://www.igualdadycalidadcba.gov.ar/SIPEC-CBA/publicaciones/Educ_Ali_Nutr_Escuela.pdf
14. Smith P, Morrow R. Ensayos de campo de intervenciones en salud en países en desarrollo. Organización Panamericana de la Salud. 1998; Cap 9:153-175.
15. García de Yébenes Proas MJ, Rodríguez Salvanés F, Carmona Ortells L. Validación de cuestionarios Reumatol Clin. 2009; 5(4):171–177.
16. Huerta JM. Procedimiento para redactar y validar los cuestionarios para los estudios de investigación y evaluación. Universidad de Puerto Rico. Recinto Universitario de Mayagüez. Colegio de Ciencias Agrícolas. 2005. citado 04/08/2016. Disponible en : http://academic.uprm.edu/jhuerta/HTMLobj-127/GUIAS1.pdf
17. Arribas M. Diseño y validación de cuestionarios. Matronas Profesión 2004; 5(17): 23-29.
18. Argentina. Córdoba. Ministerio de Salud de la Nación. Guías Alimentarias para la Población Argentina, Buenos Aires 2016.
19. Diaz Ramirez G, Souto-Gallardo MC, Bacardí Gascón M, Jiménez-Cruz A. Efecto de la publicidad de alimentos anunciados en la televisión sobre la preferencia y el consumo de alimentos: revisión sistemática. Nutr. Hosp., 2011. 26(6): 1250-1255

