










Services on Demand
Journal

Article
 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Related links
Share

 Permalink
PermalinkOdontoestomatología
Print version ISSN 0797-0374On-line version ISSN 1688-9339
Odontoestomatología vol.17 no.26 Montevideo Nov. 2015
The need for orthodontic treatment according to severity of malocclusion in adult patients
Peláez, Alina Noelia*, Gimenez Laura Itati **, Mazza, Silvia Matilde***
* Senior Teaching Assistant. Full-time position. Department of Research Methodology. School of Dentistry. Universidad Nacional del Nordeste. Argentina.
alin_pelaez@yahoo.com.ar
**Assistant Professor, Biostatistics and Experimental Design.Master's Degree in Health Sciences Research. School of Dentistry. Universidad Nacional del Nordeste. Argentina
*** Professor. Department of Research Methodology. School of Dentistry. Universidad Nacional del Nordeste. Argentina.
Abstract
Objective: To determine the need for orthodontic treatment according to severity of malocclusion using the Dental Aesthetic Index (DAI) in adult patients attending the Dentistry University Hospital, School of Dentistry, National University of the Northeast (UNNE). Methodology: A cross-sectional descriptive study was conducted on 154 patients aged 18 to 65. They were divided into two age groups: young adults and mature adults. The DAI was used to assess the need for orthodontic treatment according to severity of malocclusion, and its statistical significance according to sex and age group was analyzed. Results: 70% of the patients studied needed orthodontic treatment as they showed different degrees of severity of malocclusion. In 43% of the cases treatment was mandatory. The highest severity of malocclusion was found in males and mature adults. Conclusion: Severe malocclusion was the most prevalent condition, with a greater need for treatment in mature adult males.
Keywords: dental aesthetics, Dental Aesthetic Index, sex, age group.
Received on: 11 Dec 14 - Accepted on: 28 Jul 15
Peláez, Alina Noelia*, Gimenez Laura Itati **, Mazza, Silvia Matilde***
* Senior Teaching Assistant. Full-time position. Department of Research Methodology. School of Dentistry. Universidad Nacional del Nordeste. Argentina.
alin_pelaez@yahoo.com.ar
**Assistant Professor, Biostatistics and Experimental Design.Master's Degree in Health Sciences Research. School of Dentistry. Universidad Nacional del Nordeste. Argentina
*** Professor. Department of Research Methodology. School of Dentistry. Universidad Nacional del Nordeste. Argentina.
Abstract
Objective: To determine the need for orthodontic treatment according to severity of malocclusion using the Dental Aesthetic Index (DAI) in adult patients attending the Dentistry University Hospital, School of Dentistry, National University of the Northeast (UNNE). Methodology: A cross-sectional descriptive study was conducted on 154 patients aged 18 to 65. They were divided into two age groups: young adults and mature adults. The DAI was used to assess the need for orthodontic treatment according to severity of malocclusion, and its statistical significance according to sex and age group was analyzed. Results: 70% of the patients studied needed orthodontic treatment as they showed different degrees of severity of malocclusion. In 43% of the cases treatment was mandatory. The highest severity of malocclusion was found in males and mature adults. Conclusion: Severe malocclusion was the most prevalent condition, with a greater need for treatment in mature adult males.
Keywords: dental aesthetics, Dental Aesthetic Index, sex, age group.
Received on: 11 Dec 14 - Accepted on: 28 Jul 15
Introduction
Nowadays, malocclusion is one of the most frequent oral cavity anomalies. It is defined as an abnormal occlusion in which teeth are not in a normal position in relation to adjacent teeth in the same jaw or to the opposing teeth when the jaws are closed. Malocclusion is not a disease but a morphological variation which may or may not be associated with pathological conditions (1).
This occlusal disorder causes changes to the craniofacial structures, affecting temporomandibular articulation, neuromuscular systems or other soft tissues. These problems bring about unpleasant signs and symptoms for the patient, which in turn effect changes on facial aesthetics and on the functions of the stomatognathic system such as mastication, deglutition, breathing and phonation (2-4).
The effect of malocclusion is not only functional and/or aesthetic: it also has a psychosocial impact due to the demands of today’s world (5, 6). Our face is at the core of communication, and the smile is the door to human relations. Therefore, dental care is becoming more relevant, especially teeth alignment on dental arches (7). As the general population’s appreciation for the benefits of pleasant dentofacial proportions increases, and as orthodontic appliances are more widely accepted, requests for treatment are on the increase. This is especially the case of the adult population wishing to keep their teeth functional and aesthetically pleasing in the long term (8).
Adulthood is a stage of functional balance where growth is complete and individuals have reached their physical and intellectual peak (9). An adult is defined as a person who has ceased to grow, which happens, biologically, at around 18 years of age. Patients between 18 and 35 years of age are usually concerned about aesthetics and exhibit more periodontal and restorative problems. Patients over 36 usually exhibit complications as they may lack a full complement of teeth (10).
Orthodontic treatment in an adult patient aims mainly to improve the person’s quality of life. Adults seek this type of treatment to correct malocclusion, improve function, dental and facial aesthetics and oral health. These patients exhibit more severe problems, regarding both number and complexity. Complications in adult patients with need of orthodontic treatment frequently include tooth migration due to tooth loss. These problems cause generalized gaps between the arches, which may lead to inclinations or rotations resulting in premature contacts and severe malocclusion problems (11).
Several methodologies and indexes have been developed to quantify the presence and severity of malocclusion so as to determine its relation and impact on aesthetics and the need for treatment. The World Health Organization (WHO) (12) has opted for the Dental Aesthetic Index (DAI) (13). Different criteria have been described to achieve an ideal index: the most important ones are validity and reliability (14, 15).
Since its creation in 1986, the DAI has proven to be reliable and valid, as well as simple and easy to apply (13). This is shown in various studies (16-19).
It is a very useful index, especially because it provides scores that can be quantified, thus providing information about the morphological, functional and aesthetic aspects classified into severity levels. It is then possible to determine the need for orthodontic treatment, and to provide guidelines for health prevention programs by establishing priorities of access to care facilities in the community (20, 21).
In the light of the above, the aim of this study was to determine the need for orthodontic treatment according to severity of malocclusion using the Dental Aesthetic Index (DAI) in adult patients attending the Dentistry University Hospital, School of Dentistry, National University of the Northeast (UNNE).
Materials and methods
A cross-sectional observational descriptive study was conducted. The research protocol was approved by the Ethics Committee of the School of Dentistry of the UNNE. Between March and July of 2011, 2290 patients attended the Dentistry University Hospital, School of Dentistry of the UNNE for comprehensive dental care. Inclusion and exclusion criteria were applied to the group as explained below.
Inclusion criteria: adults patients that gave their consent to participate in the study. Exclusion criteria: patients under 18 years of age, completely edentulous patients, patients suffering from a significant systemic pathology, patients that had received or were receiving any kind of orthodontic treatment. According to these criteria, the target population was formed by 1540 patients. Systematic random sampling was used to select 154 patients, at intervals 1 and 10. The resulting sample was of 10% of the population under study.
Clinical examination: patients were provided a fact sheet including the procedures and aims of the study to be conducted. After the examination, the DAI was applied, and the ten variables of the index regarding dentition, spacing and occlusion were analyzed. All the clinical information was recorded by the same examiner, who had been especially trained. Intra-examiner calibration was done by measuring DAI components twice (with an interval higher than 1 hour) on the same patient, by the same examiner and with the same instrument on 15 randomly selected patients. Pearson’s correlation analysis and simple linear regression analysis were used to test the consistency of both measurements, where a y=x line is adjusted, where y: DAI value estimated by measuring the components of the second measurement, and x: DAI value estimated by measuring the components of the first measurement. Pearson’s correlation coefficient was r=0.99 (p-value<0.0001), and in the regression analysis the estimation of parameter α was not significantly different from zero (p-value=0.3673). Parameter estimation was equal to 0.97, and differed significantly from zero (p-value=0.0001), with an R2=0.98. This shows a high correlation between both measurements, which are linearly related through a line starting from the origin of the coordinate system which has a slope of approximately 45º. This proves the consistency of both measurements.
The variables expressed in millimeters were measured using William-Fox (Hu-Friedy) probe. The DAI was calculated and the data were collected following the WHO guidelines included in the Oral Health Surveys: Basic Methods (12). The following are the variables used:
1) Missing teeth: dentition was evaluated by recording the number of permanent teeth lost, from the second premolar tooth of one side to that of the contralateral side in both arches. Incisors, canines and premolars where the extraction gaps had been filled with a prosthesis were not considered missing.
2) Crowding: to determine crowding in the incisal segments we applied the following criteria: 0: no crowding, 1: one segment crowded (upper or lower) and 2: two segments crowded (upper and lower).
3) Spacing: to determine spacing in the incisal segments we applied the same criteria as for crowding: 0: no spacing, 1: one segment spaced (upper or lower) and 2: two segments spaced (upper and lower).
4) Diastema: a midline diastema as defined in millimeters, measuring the space between permanent upper or lower central incisors.
5) Largest anterior maxillary irregularity: the anterior maxillary irregularities considered were rotations and/or displacements of incisors outside the arch. The irregularity is measured in millimeters.
6) Largest anterior mandibular irregularity: the criteria were the same used for the anterior maxillary sector.
7) Maxillary overjet: it was measured in millimeters considering the distance between the vestibular surface of the lower incisor and the incisal edge of the most slanting upper incisor. If upper and lower incisors are in an edge to edge relation, the score was zero.
8) Mandibular overjet: it was measured as the maxillary overjet, and it was determined as an anterior cross-bite.
9) Anterior open bite: when there was no occlusal vertical contact between upper and lower incisors. The area with the highest open bite was recorded in millimeters.
10) Anteroposterior molar relation: recorded based on the first permanent upper and lower molars, evaluating both sides with the teeth in occlusion. The relation was recorded as normal or with mesial or distal displacement. When it was not possible to evaluate molars because they were missing, partially erupted, altered by caries or restorations, canines and premolars were considered.
Once all the index variables had been recorded, the DAI equation was applied to calculate the final score using the following formula:
Missing teeth (x 6) + Crowding + Spacing) + Diastema (x 3) + Maxillary irregularity + Mandibular irregularity + Maxillary overjet (x 2) + Mandibular overjet (x 4) + Anterior open bite (x 4) + Anteroposterior molar relation x 3) + 13 = DAI
The score for each of the ten variables or occlusal characteristics analyzed for each patient was multiplied by the corresponding coefficient or DAI equation weighting. The ten resulting new values were added and a constant of value = 13 was added to such result. Each patient was given a final score which determined the severity of malocclusion and the need for orthodontic treatment as per the weighting interval where the patient was placed.
DAI weighting intervals according to the score obtained are as follows:
• ≤ 25 points: normal occlusion or mild malocclusion.
• Between 26 and 30 points: defined malocclusion, elective treatment.
• Between 31 and 35 points: severe malocclusion, treatment is highly desirable.
• 36 points onwards: very severe malocclusion, treatment is mandatory.
Patients were divided into two age groups covering the age interval of the individuals attending the hospital in the period when this study was conducted: between 18 and 35 years of age, young adults; and between 36 and 65 years of age, mature adults (10).
The values obtained were evaluated using Chi-square data exploratory analysis graphical techniques to test the independence of the malocclusion levels defined as per DAI, sex and age. Infostat statistical software (22) was used to analyze the data.
Results
Out of the 154 patients evaluated, 58% were female and 42% male; 65% were in the 18-35 age group (young adults) and 35% in the 36-65 age group (mature adults) (Table N°1).
Table N°1: Sample distribution according to sex and age group
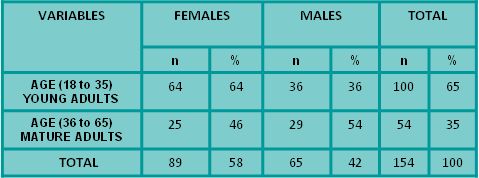
Table N°2 shows the evaluation of the need for orthodontic treatment according to severity of malocclusion by applying the DAI index: 30% of the patients studied had normal or mild malocclusion and do not need orthodontic treatment, while 70% needed orthodontic treatment according to different degrees of severity of malocclusion, among whom 43% had very severe or disabling malocclusion, making orthodontic treatment mandatory.
Table N°2: Severity of malocclusion and need for orthodontic treatment according to the Dental Aesthetic Index
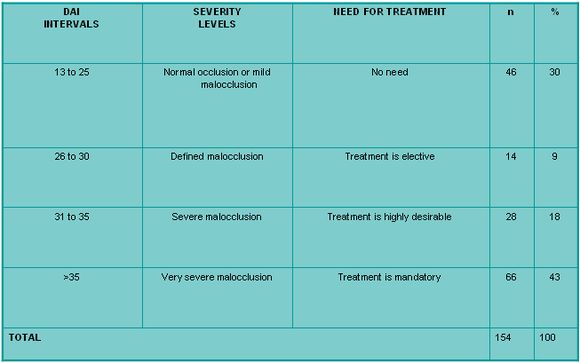
Table N°3. Absolute and relative frequencies of the Dental Aesthetic Index components
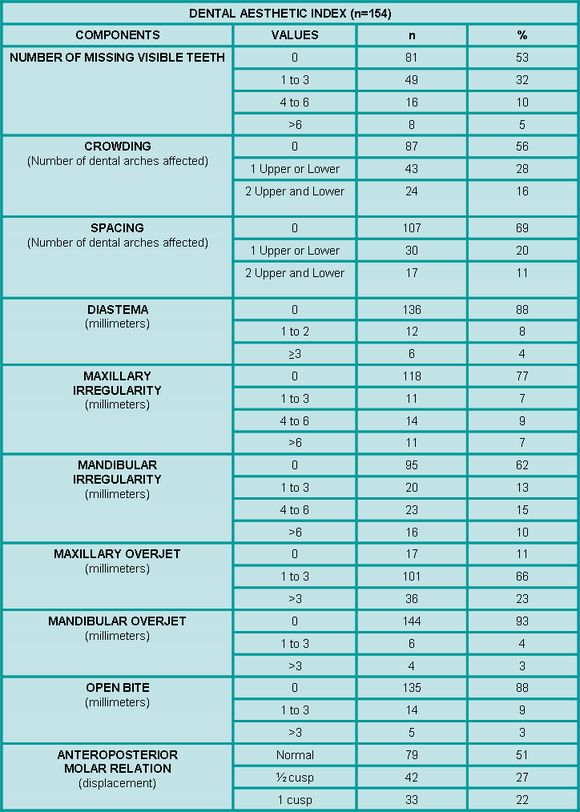
The analysis of the different components shows that the need for orthodontic treatment matches the severity of malocclusion detected.
In 47% of patients there were missing visible teeth, with a statistically significant difference (p < 0.01) between age groups. 65% of young adults had no missing teeth, 30% had between 1 and 3 missing visible teeth, and only 5% had over 3 missing teeth. Among mature adults, 70% had missing visible teeth and only 30% had all the teeth in the anterior sector. Regarding sex, no differences were detected (p=0.3).
Dental crowding in the incisal segment in one or both upper and lower arches was detected in 44% of cases. Mandibular irregularity was higher (>4 mm) at 28%, while maxillary irregularity (>4 mm) was of 16%. Another frequent alteration was molar relation, present in 49% of cases with anteroposterior displacement of ½ cusp or a whole cusp.
Regarding molar relation, no significant differences were found between anteroposterior molar displacement regarding sex (0.993) and age group (p=0.339). Less frequent alterations were open bite and diastema (12%), maxillary overjet (23%) and mandibular overjet (6%).
Table N°4 shows the distribution of the different levels of DAI severity of malocclusion according to sex.
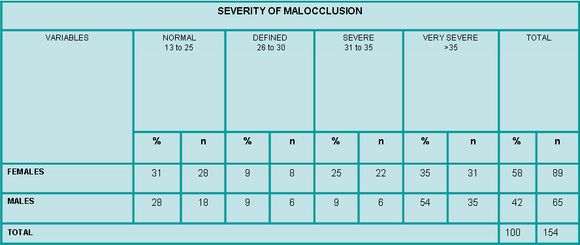
Statistically significant differences were found between both variables (p=0.04). Females presented normal occlusion in 31% of cases and males in 28% of cases. Very severe or disabling malocclusion requiring treatment appeared in 35% of females and in 54% of males. The most notable difference was found in severe malocclusion, where treatment is not mandatory but desirable: it was present in 25% of females and in 9% of males.
Table N°5 shows the distribution of DAI severity of malocclusion according to age group.
Table N°5: Frequency and distribution of severity of malocclusion according to age group (DAI)
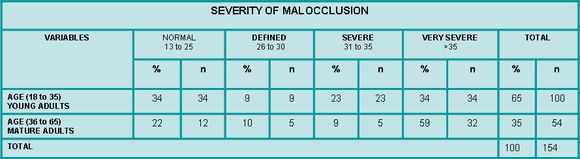
Statistically significant differences were found between both variables (p<0.01). Normal occlusion was highest in the young adult group with 34%, while in mature adults it was present in 22% of cases. The most marked difference was found in severe malocclusion: 23% among young adults and only 9% among mature adults. It is important to emphasize that severe malocclusion was the most prevalent condition among mature adults with 59% of cases, making treatment mandatory.
Discussion
The Dental Aesthetic Index sets forth a series of occlusal characteristics or conditions organized into categories that determine the level of severity of malocclusion according to an ordinal scale. Its value resides in its description of the morphological characteristics of malocclusion and in its therapeutic approach, which focuses on the patients’ need for orthodontic treatment. A further advantage of the index is its reproducibility and ease of intra examiner reliability calibration, as observed in this study.
When applying the DAI on the adult population of the Dentistry University Hospital, School of Dentistry of the UNNE, we observed that 70% of the patients examined had varying levels of malocclusion severity and need for treatment. Very severe malocclusion was the most prevalent with 43% of cases. It is important to note that treatment is mandatory in these cases (Table N°2).
Santos et al. (23) used the DAI to study the prevalence of malocclusion and the need for orthodontic treatment in a population similar to that of this study regarding methodology, number of patients evaluated and age interval. The sample included 156 adult patients aged between 18 and 50 who attended the dental clinics at the Universidad del Estado de Paraíba, Brazil, in 2011. These authors observed that 63.5% of patients showed some level of severity, among whom 47% had severe malocclusion, making treatment mandatory. These results are very similar to those of this research. However, our results differ from those of Bellot et al. (24) obtained in 2012 through an epidemiological study conducted in the health centers of the Valencian Community in Spain. They applied the DAI on 671 adults aged between 35 and 44 and observed that 31.1% of the sample needed orthodontic treatment, figure which is lower than the one observed in our study. Prevalence of DAI malocclusion is also lower in a study conducted in all the departments of Uruguay except the capital among adolescents and young adults aged between 15 and 24, where 33.8% had malocclusion and only 8.54% were cases of very severe malocclusion (25).
The analysis of the Index components separately (Table N°3) shows the high prevalence of malocclusion with need for orthodontic treatment in these patients. The most significant alterations were missing visible teeth (47%), crowding on one or both arches (44%) and anteroposterior molar displacement (49%). These results are very similar to those reported by researchers that have evaluated malocclusion using the DAI in populations over 17 years of age: Santos et al. (23), Bernabé and Flores-Mir (26), Claudino and Traebert (27).
As for the connection between severity of malocclusion, need for orthodontic treatment and sex, statistically significant differences were found (p=0.04) (Table N°4). The most significant difference was found in severe malocclusion: 25% among females and 9% among males. However, we cannot say that females have the greatest need for orthodontic treatment as when compared to males, females showed more cases of normal occlusion and 69% needed orthodontic treatment, this treatment being mandatory in only 35% of cases. In turn, among males, the need for orthodontic treatment was present in 72% of cases, this treatment being mandatory in 54% of cases, which exceeds the values among female patients. When comparing these values to those of other international studies (23, 26, 28, 29), no sex-based differences are found.
As for the connection between severity of malocclusion, need for orthodontic treatment and age group, statistically significant differences were found (p=0.01) (Table N°5). It must be noted that we have not found scientific studies that associate DAI malocclusion to the age groups in this study. Therefore, it is not possible to compare these values to those of other situations. The most marked difference in this connection was found in severe malocclusion: 23% among young adults and only 9% among mature adults. However, when comparing values of severity of malocclusion separately within each age group, among young adults there was an equal distribution between normal occlusion and very severe malocclusion: both prevalent in 34% of cases. However, there was a 59% prevalence of very severe malocclusion among mature adults, where treatment was mandatory. Malocclusion was mainly affected by missing visible teeth in 70% of cases, which compromises dental aesthetics. These values are very similar to those presented by Santos et al. (23).
Conclusion
Adult patients at the Dentistry University Hospital, School of Dentistry of the UNNE, have a great need for orthodontic treatment. We observed that 70% of the patients had varying levels of malocclusion severity, where very severe malocclusion was prevalent: 43% of cases. The need for treatment was mandatory. The high prevalence of malocclusion was reflected in the most frequent alterations: missing visible teeth (47%), crowding on one or both arches (44%) and anteroposterior molar displacement of ½ cusp or a whole cusp (49%).
The highest severity of malocclusion was found in male and mature adults. This age group was mainly affected by a 70% of missing visible teeth. Only 30% of mature adults had all the teeth in the anterior sector.
Given the high prevalence of malocclusion and need for orthodontic treatment, we suggest that new public health care models be developed to anticipate the different types of demand and to plan for satisfactory resource allocation. This is essential as orthodontic treatment services are not easily available and accessible to the general population. These actions aim to promote the supply of orthodontic to foster the implementation of programs including preventive and interceptive actions as well as treatment options. We must remember that malocclusion is a major dental health problem, and hence establish access priorities to care facilities in our community.
References
1.Davies SJ. Malocclusion a term in need of dropping or redefinition? Br Dent J. 2007; 202: 519-520.
2.Gesch D, Bernhardt O, Kocher T, John U, Hensel E, Alte D. Association of Malocclusion and Functional Occlusion With Signs of Temporomandibular Disorders in Adults: Results of the Population-based Study of Health in Pomerania. Angle Orthodon 2004; 74 (4): 512-520.
3.Aznar Martín T, Galán González AF, Martín Castro IM, Domínguez Reyes A. Dental Arch Diameters and relation ship to oral habits. Angle Orthodont 2005; 76(3):34-38.
4.Almeida AB, Leite ICG, Melgaço CA, Marques LS. Dissatisfaction with dentofacial appearance and the normative need for orthodontic treatment: determinant factors. Dental Press J. Orthod. 2014; 19(3):120-126.
5.Klages U, Claus N, Wehrbein H, Zentner A. Development of a questionnaire for assessment of the psychosocial impact of dental aesthetics in young adults. Eur J. Orthod. 2006; 28(2):103-111.
6.Taylor KR, Kiyak A, Huang GJ, Greenlee GM, Jolley CJ, King GJ. Effects of malocclusion and its treatment on the quality of life of adolescents. Am J. Orthod Dentofacial Orthop. 2009; 136(3):382-392.
7.Botero PM, Vélez N, Cuesta DP, Gómez E, González PA, Cossio M, Santos E. Perfil epidemiológico de oclusión dental en niños que consultan a la Universidad Cooperativa de Colombia. Rev CES Odont. 2009; 22(1):9-13.
8.Girón HF, Fernández ST. Ortodoncia en un paciente adulto mayor. Rev Mex Ortodon. 2014; 2 (3):196-203.
9.Cruz ED, Collado OL, Fernández MI, Díaz RB. Factores de riesgo de maloclusiones en adultos. Invest Medicoquir 2012; 4 (2):137-145.
10.Singh G. Ortodoncia, Diagnóstico y Tratamiento. 2 ed. Venezuela Amolca. 2009. p 671-684
11.Ayala - Sarmiento AP, Rivas - Gutiérrez R. El tratamiento de ortodoncia en el paciente adulto. Rev Tamé [en línea]; 2014; 3 (8): 283-287. [Fecha de acceso: 8 julio 2015]. Disponible en:
http://www.uan.edu.mx/d/a/publicaciones/revista_tame/numero_8/Tam148-8.pdf
12.OMS. Encuestas de salud Bucodental. Métodos Básicos. 4ed. Ginebra: Organización Mundial de la Salud, 1997.p 46-52
13.Cons NC, Jenny J, Kohout FJ. DAI: The Dental Aesthetic Index. Iowa City: College of Dentistry, University of Iowa; 1986.
14.Järvinen S. Indexes for orthodontic treatment need. Am J Orthod Dentofacial Orthop 2001: 120: 237-239.
15.Abdullah MS, Rock WP. Assessment of orthodontic treatment need in 5.112 Malaysian children using the IOTN and DAI indices. Community Dent Health. 2001; 18:242–248.
16.Spencer AJ, Allister JH, Brennan DS. Utility of the Dental Aesthetic Index as an Orthodontic Screening Tool in Australia. Adelaide: University of Adelaide; 1992.
17.Jenny J, Cons NC, Kohout FJ, Jakobsen J. Predicting handicapping malocclusion using the Dental Aesthetic Index (DAI). Int Dent J. 1993; 43:128–132.
18.Jenny J, Cons NC. Comparing and contrasting two orthodontic indices, the index of orthodontic treatment need and the dental aesthetic index. Am J Orthod Dentofacial Orthop. 1996; 110:410–416.
19.Beglin FM, Firestone AR, Vig KW, Beck FM, Kuthy RA, Wade D. A comparison of the reliability and validity of 3 occlusal indexes of orthodontic treatment need. Am J Orthod Dentofacial Orthop. 2001; 120:240–246.
20.Tapias MA, Jiménez García R, Lamas F, Carrasco P, Gil A. Prevalencia y distribución de maloclusión en una población infantil de Móstoles. Arch Odontoestomat. 2003; 39 (2): 87-91.
21.Solarte J, Rocha A, Agudelo AA. Perfil epidemiológico de las alteraciones de la oclusión en la población escolar del corregimiento de Genoy, municipio de Pasto, Colombia. Rev Fac Odontol Univ Antioq. 2011; 23(1): 111-125.
22.Di Rienzo JA, Casanoves F, Balzarini MG, Gonzalez L, Tablada M, Robledo CW. InfoStat versión 2013. Grupo InfoStat, FCA, Universidad Nacional de Córdoba, Argentina. [fecha de acceso: 8 julio 2015]. Disponible en: http://www.infostat.com.ar/
23.Santos JA, Barros Florentino VG, Santana Sarmento DJ, Cavalcanti AL. Prevalência de maloclusão e necessidade de tratamento ortodôntico em indivíduos adultos. Act Scientiarum. Health Sciences. 2011; 33 (2): 197-202
24.Bellot-Arcís C, Montiel-Company JM, Manzanera-Pastor D, Almerich-Silla JM. Orthodontic treatment need in a Spanish young adult population. Med Oral Patol Oral Cir Bucal. 2012 Jul 1;17 (4): 638-643
25.Ourens M, Celeste RK, Hilgert JB, Lorenzo S, Hugo FN, Álvarez R, Abegg C. Prevalencia de maloclusiones en adolescentes y adultos jóvenes del interior del Uruguay. Relevamiento nacional de salud bucal 2010-2011. Odontoestomatología [en linea]. 2013, 15: 47-57. [fecha de acceso: 09 de marzo de 2015] Disponible en: http://www.scielo.edu.uy/pdf/ode/v15nspe/v15nspea06.pdf.
26.Bernabé E, Flores-Mir C. Orthodontic Treatment Need in Peruvian Young Adults Evaluated Through Dental Aesthetic Index. Angle Orthodont 2006; 76 (3): 417-421.
27.Claudino D, Traebert J. Malocclusion, dental aesthetic self-perception and quality of life in a 18 to 21 year-old population: a cross section study. BMC Oral Health [en linea] 2013, 13:3. [fecha de acceso: 22 de octubre de 2014] Disponible en: http://www.biomedcentral.com/1472-6831/13/3

