










Services on Demand
Journal

Article
 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Related links
Share

 Permalink
PermalinkOdontoestomatología
On-line version ISSN 1688-9339
Odontoestomatología vol.16 no.24 Montevideo Nov. 2014
Application of parallel measuring techniques in the lateral sectors of the lower dental arch in a population of schoolchildren
Prestia EG*,
Discacciati de Lértora MS**,
Galiana AV***
* Trainee, Pediatric Dentistry Department. Facultad de Odontología, Universidad Nacional del Nordeste.
** Former Assistant Professor at the Pediatric Dentistry Department. MA. Facultad de Odontología, Universidad Nacional del Nordeste
*** Assistant Professor at the Pediatric Dentistry Department. MA. Facultad de Odontología, Universidad Nacional del Nordeste.
andreagaliana@hotmail.com
Abstract
The predictive analysis for mixed-dentition allows us to determine, even before the eruption of permanent canines and premolars, the space these teeth will need within the dental arch, thus facilitating an early diagnosis and adequate treatment planning. The aim of this study was to determine the reliability and validity of two methods that measure the mesio-distal diameters of primary teeth in the lower dental arch. The sample was formed by 80 children treated at the Pediatric Dentistry Department of the FOUNNE and whose ages range between 6 and 8. Their clinical records, dental impressions and study models were prepared. The measurements were taken in mouth (direct method) and in study models (indirect method), using drypoint compass in both cases. The results did not show significant differences, which demonstrates that both methods are equally valid and reliable.
Keywords: Reliability, Mesio-distal diameters, Odontometrics, Primary tooth, Child, Validity of tests.
Received on: 03 Jul 2014 – Accepted on: 08 Oct 2014
Introduction and background
The study and integral analysis of patients in early childhood allows the pediatric dentist to diagnose and intercept alterations that may affect the normal development of the dentition (1). Mesio-distal width of tooth crowns and primary dentition occlusion play a significant role in the spacing and occlusion of permanent dentition (2).
In recent years there has been growing interest in the prevention and early treatment of malocclusion in mixed dentition, as many alterations occur in primary dentition and during deciduous teeth replacement. This is why early and suitable treatment can help reduce, eliminate and even prevent these alterations (3, 4, 5). The predictive analysis for mixed dentition allows us to determine, even before the eruption of permanent canines and premolars, the space these teeth will need within the dental arch, thus facilitating an early diagnosis and a suitable treatment plan. It is essential to consider that this analysis is conducted on a growing child, where time becomes a relevant variable. To diagnose and predict occlusion as part of the routine clinical examination we need to evaluate. Some procedures enhance the accuracy of the diagnosis, for example measurement techniques, which provide information to help diagnose and thus take better decisions in treatment planning.Numerous analysis methods based on measurements have been proposed to complement diagnosis (6, 7, 8): good judgment and development knowledge are essential to take the measurements and apply these methods.
To measure is to compare an element of unknown dimensions to measurement units that cannot be modified. Measurements should be taken as accurately as possible, which is especially difficult to do in children due to their age, and behavior and intellectual stage of development, which can many times render the task particularly difficult. Therefore, it is necessary to find a quality and applicable method to take measurements on children, where the reliability and validity of the procedure or technique become crucial.
Reliability is the degree of precision with which a technique provides information (8). It indicates the extent to which measurement errors can give rise to individual differences in the results obtained, as well as the extent to which the results show real differences in the characteristics evaluated (10). The reliability of the results of taking measurements and applying techniques lies in the accuracy and precision of the measuring procedures. This can be verified, for example with the test‑retest method, taking the same measurement on the same subject, and running parallel tests, using two instruments which measure the same elements. Parallel tests provide a solid basis to estimate the accuracy of a measurement. The level of reliability can be seen when consistency is achieved in different measurements (9).
Validity is another aspect of the quality of a measurement technique. It allows us to evaluate the suitability of quantitative measurement techniques, and to determine the degree to which the instrument measures what it is supposed to measure (13).
Therefore, reliability and validity are two important aspects when evaluating quantitative measurement. By showing that a technique is reasonably reliable and valid for a specific purpose, it is more likely that the study will find significant results (9).
The aim of this study was to determine the reliability and validity of two methods that measure the mesio-distal diameters of primary teeth in the lateral sector of the lower dental arch.
Methods
The sample was formed by 80 children aged between 6 and 8 who were being treated at the Pediatric Dentistry Department of the FOUNNE, Facultad de Odontología, Universidad Nacional del Nordeste, in the city of Corrientes, Argentina. The following criteria were considered to include them in the study: collaborative and healthy children, with healthy teeth in the lower lateral sectors (canine, first and second primary molars) of the dental arch, with no anomalies regarding number, structure and form, and without restorations or fractures that could have modified the mesio‑distal diameter of teeth.
After having written consent signed by the children's parents or guardian, we prepared their Clinical Records following routine general and specific guidelines. We then measured the mesio-distal diameters of teeth, which were selected according to the criteria for inclusion.
To determine validity and reliability, the measurements were taken by the same professional, applying parallel tests and using two instruments which take the same measurements: a. direct method (measurement of mesio-distal diameters in mouth); and b. indirect method (measurement of mesio-distal diameters in study models).
a. Direct method: Observations were conducted in mouth, with natural light, with the child at a 90º sitting position on the dental chair. The surfaces of each tooth in the sector were dried. Then, mesio-distal diameters were measured using a drypoint compass. The useful measurement was the maximum distance from the tooth crown between the proximal contact points of the selected teeth, parallel to the buccal and occlusal surfaces and perpendicular to the long axis of the tooth. To that end, the tips of the compass were placed perpendicular to the occlusal plane in the previously determined places. It was then possible to have a horizontal line which corresponded to the area under study. The measurement was transferred to a millimeter rule, calibrated to a precision of 0.5 mm, and the measurement was determined and expressed in mm (Fig. 1 and 3).
b. Indirect method: The observations were conducted on study models corresponding to each child from the sample. After persuading the patient to cooperate, the impression was taken and the models made. The impressions were made using fast-set alginate, using partial aluminum trays which were previously perforated, adapted and outlined with Utility wax. Then they were emptied using stone cast. The measurement procedure was the same as in the direct method. A drypoint compass was used. The useful measurement was the maximum distance from the tooth crown between the proximal contact points, parallel to the buccal and occlusal surfaces and perpendicular to the long axis of the tooth. The measurement was transferred to a millimeter rule, calibrated to a precision of 0.5 mm to obtain the necessary value (Fig. 2 and 3).


Fig. 1: Direct method. Measurement in mouth Fig. 2: Indirect method. Measurement in model
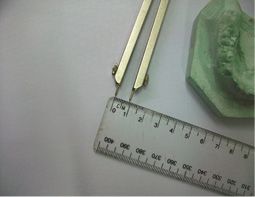
Fig. 3: Measurement transferred to millimeter rule.
Results
The average age of the children was 6.5 years, and 68% of them were male and 32% female. Both the direct and indirect methods (parallel tests) were used in 100% of the children. These were the results obtained:
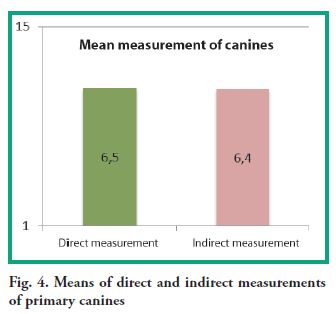
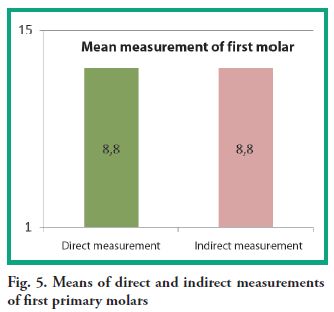
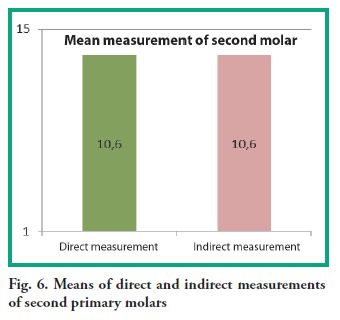
Mean values of mesio-distal width of primary teeth using the direct method were: 6.5 mm for canines, 8.8 mm for the first molar and 10.7 mm for the second molar. Mean values of mesio-distal width of primary teeth using the indirect method were: 6.4 mm for canines, 8.8 mm for the first molar and 10.6 mm for the second molar (Fig. 4, 5 and 6).
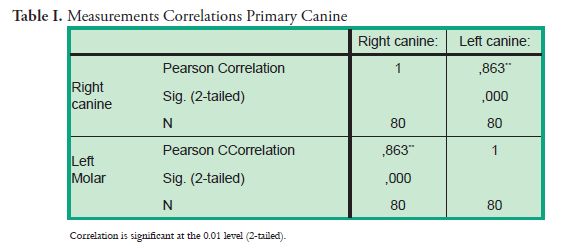
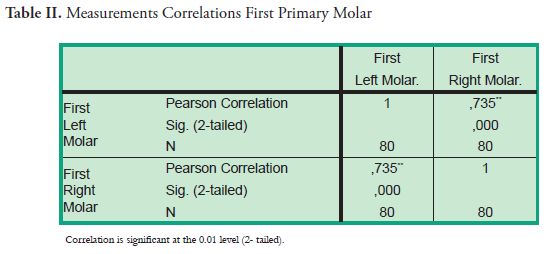
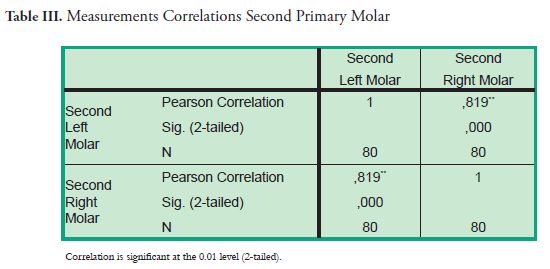
The correlations (Pearson correlation coefficient) determined for both methods showed values between 0.863 and 0.735 for canines and first and second molars, with a significance value of 0.05 (Tables I, II and III).
Discussion and conclusions
The study of occlusion in children as part of a routine exam in Pediatric Dentistry makes it necessary to take measurements for the early diagnosis and prognosis of pathologies in primary and mixed dentition. This study presents findings of interest and to be considered when taking the measurements required, both in clinical studies and applied research.
Numerous authors have conducted research using both the direct and indirect measurement methods to study tooth crown and root diameters, both in primary and permanent teeth (12, 13, 14, 15).
By showing that the technique is reasonably reliable and valid for a specific purpose, we can provide more certainty, and it is more likely that the study will find significant results. According to Bertoni and collaborators (9), the measurements taken in a study should have two important qualities: reliability and validity, so that they can be interpreted and extrapolated. Therefore, before applying a measurement technique in scientific research, we must prove that the technique has these properties.
Regarding reliability, a measuring instrument is reliable when we obtain measurements or data that represent the real value of the variable measured. Camillioni (10) states that reliability may indicate the extent to which there can be measurement errors and individual differences in the results obtained, as well as the extent to which the results show differences in the characteristics evaluated. In this study, after applying parallel tests (in mouth and in models), no significant differences were found, which renders both tests reliable.
Additionally, an instrument can be reliable but not valid (not measure what it intends to), which is not applicable in this case as the data obtained through measurements have been contrasted applying both methods. Both the direct and the indirect technique allow us to measure the mesio-distal distance of primary teeth in the lateral sector. We can thus have values expressed in mm to facilitate diagnosis, prognosis and a suitable treatment plan.
Hernández Sampieri (16) considers it fundamental that an instrument should be reliable and valid: if not, the results of the research should not be taken seriously. In this study, the results obtained showed that both measurement methods are valid and reliable. We agree with Brailosky (17): "Measurement instruments should be valid and reliable", which suggests that either method can be used in clinical research. The choice should be made according to the specific requirements of the study in question. In Pediatric Dentistry, both methods can be suitable depending on the child's behavior, since the indirect method requires taking an impression, which might not be an easy task. The direct method can also pose difficulties if the child does not behave as expected.
When the direct and indirect methods are used in children of school age to measure mesio-distal diameters of primary teeth, the probability of error in either method is minimal (less than 1%), which proves that both methods are reliable and valid.
Prestia EG*,
Discacciati de Lértora MS**,
Galiana AV***
* Trainee, Pediatric Dentistry Department. Facultad de Odontología, Universidad Nacional del Nordeste.
** Former Assistant Professor at the Pediatric Dentistry Department. MA. Facultad de Odontología, Universidad Nacional del Nordeste
*** Assistant Professor at the Pediatric Dentistry Department. MA. Facultad de Odontología, Universidad Nacional del Nordeste.
andreagaliana@hotmail.com
Abstract
The predictive analysis for mixed-dentition allows us to determine, even before the eruption of permanent canines and premolars, the space these teeth will need within the dental arch, thus facilitating an early diagnosis and adequate treatment planning. The aim of this study was to determine the reliability and validity of two methods that measure the mesio-distal diameters of primary teeth in the lower dental arch. The sample was formed by 80 children treated at the Pediatric Dentistry Department of the FOUNNE and whose ages range between 6 and 8. Their clinical records, dental impressions and study models were prepared. The measurements were taken in mouth (direct method) and in study models (indirect method), using drypoint compass in both cases. The results did not show significant differences, which demonstrates that both methods are equally valid and reliable.
Keywords: Reliability, Mesio-distal diameters, Odontometrics, Primary tooth, Child, Validity of tests.
Received on: 03 Jul 2014 – Accepted on: 08 Oct 2014
Introduction and background
The study and integral analysis of patients in early childhood allows the pediatric dentist to diagnose and intercept alterations that may affect the normal development of the dentition (1). Mesio-distal width of tooth crowns and primary dentition occlusion play a significant role in the spacing and occlusion of permanent dentition (2).
In recent years there has been growing interest in the prevention and early treatment of malocclusion in mixed dentition, as many alterations occur in primary dentition and during deciduous teeth replacement. This is why early and suitable treatment can help reduce, eliminate and even prevent these alterations (3, 4, 5). The predictive analysis for mixed dentition allows us to determine, even before the eruption of permanent canines and premolars, the space these teeth will need within the dental arch, thus facilitating an early diagnosis and a suitable treatment plan. It is essential to consider that this analysis is conducted on a growing child, where time becomes a relevant variable. To diagnose and predict occlusion as part of the routine clinical examination we need to evaluate. Some procedures enhance the accuracy of the diagnosis, for example measurement techniques, which provide information to help diagnose and thus take better decisions in treatment planning.Numerous analysis methods based on measurements have been proposed to complement diagnosis (6, 7, 8): good judgment and development knowledge are essential to take the measurements and apply these methods.
To measure is to compare an element of unknown dimensions to measurement units that cannot be modified. Measurements should be taken as accurately as possible, which is especially difficult to do in children due to their age, and behavior and intellectual stage of development, which can many times render the task particularly difficult. Therefore, it is necessary to find a quality and applicable method to take measurements on children, where the reliability and validity of the procedure or technique become crucial.
Reliability is the degree of precision with which a technique provides information (8). It indicates the extent to which measurement errors can give rise to individual differences in the results obtained, as well as the extent to which the results show real differences in the characteristics evaluated (10). The reliability of the results of taking measurements and applying techniques lies in the accuracy and precision of the measuring procedures. This can be verified, for example with the test‑retest method, taking the same measurement on the same subject, and running parallel tests, using two instruments which measure the same elements. Parallel tests provide a solid basis to estimate the accuracy of a measurement. The level of reliability can be seen when consistency is achieved in different measurements (9).
Validity is another aspect of the quality of a measurement technique. It allows us to evaluate the suitability of quantitative measurement techniques, and to determine the degree to which the instrument measures what it is supposed to measure (13).
Therefore, reliability and validity are two important aspects when evaluating quantitative measurement. By showing that a technique is reasonably reliable and valid for a specific purpose, it is more likely that the study will find significant results (9).
The aim of this study was to determine the reliability and validity of two methods that measure the mesio-distal diameters of primary teeth in the lateral sector of the lower dental arch.
Methods
The sample was formed by 80 children aged between 6 and 8 who were being treated at the Pediatric Dentistry Department of the FOUNNE, Facultad de Odontología, Universidad Nacional del Nordeste, in the city of Corrientes, Argentina. The following criteria were considered to include them in the study: collaborative and healthy children, with healthy teeth in the lower lateral sectors (canine, first and second primary molars) of the dental arch, with no anomalies regarding number, structure and form, and without restorations or fractures that could have modified the mesio‑distal diameter of teeth.
After having written consent signed by the children's parents or guardian, we prepared their Clinical Records following routine general and specific guidelines. We then measured the mesio-distal diameters of teeth, which were selected according to the criteria for inclusion.
To determine validity and reliability, the measurements were taken by the same professional, applying parallel tests and using two instruments which take the same measurements: a. direct method (measurement of mesio-distal diameters in mouth); and b. indirect method (measurement of mesio-distal diameters in study models).
a. Direct method: Observations were conducted in mouth, with natural light, with the child at a 90º sitting position on the dental chair. The surfaces of each tooth in the sector were dried. Then, mesio-distal diameters were measured using a drypoint compass. The useful measurement was the maximum distance from the tooth crown between the proximal contact points of the selected teeth, parallel to the buccal and occlusal surfaces and perpendicular to the long axis of the tooth. To that end, the tips of the compass were placed perpendicular to the occlusal plane in the previously determined places. It was then possible to have a horizontal line which corresponded to the area under study. The measurement was transferred to a millimeter rule, calibrated to a precision of 0.5 mm, and the measurement was determined and expressed in mm (Fig. 1 and 3).
b. Indirect method: The observations were conducted on study models corresponding to each child from the sample. After persuading the patient to cooperate, the impression was taken and the models made. The impressions were made using fast-set alginate, using partial aluminum trays which were previously perforated, adapted and outlined with Utility wax. Then they were emptied using stone cast. The measurement procedure was the same as in the direct method. A drypoint compass was used. The useful measurement was the maximum distance from the tooth crown between the proximal contact points, parallel to the buccal and occlusal surfaces and perpendicular to the long axis of the tooth. The measurement was transferred to a millimeter rule, calibrated to a precision of 0.5 mm to obtain the necessary value (Fig. 2 and 3).
Fig. 1: Direct method. Measurement in mouth Fig. 2: Indirect method. Measurement in model
Fig. 3: Measurement transferred to millimeter rule.
Results
The average age of the children was 6.5 years, and 68% of them were male and 32% female. Both the direct and indirect methods (parallel tests) were used in 100% of the children. These were the results obtained:
Mean values of mesio-distal width of primary teeth using the direct method were: 6.5 mm for canines, 8.8 mm for the first molar and 10.7 mm for the second molar. Mean values of mesio-distal width of primary teeth using the indirect method were: 6.4 mm for canines, 8.8 mm for the first molar and 10.6 mm for the second molar (Fig. 4, 5 and 6).
The correlations (Pearson correlation coefficient) determined for both methods showed values between 0.863 and 0.735 for canines and first and second molars, with a significance value of 0.05 (Tables I, II and III).
Discussion and conclusions
The study of occlusion in children as part of a routine exam in Pediatric Dentistry makes it necessary to take measurements for the early diagnosis and prognosis of pathologies in primary and mixed dentition. This study presents findings of interest and to be considered when taking the measurements required, both in clinical studies and applied research.
Numerous authors have conducted research using both the direct and indirect measurement methods to study tooth crown and root diameters, both in primary and permanent teeth (12, 13, 14, 15).
By showing that the technique is reasonably reliable and valid for a specific purpose, we can provide more certainty, and it is more likely that the study will find significant results. According to Bertoni and collaborators (9), the measurements taken in a study should have two important qualities: reliability and validity, so that they can be interpreted and extrapolated. Therefore, before applying a measurement technique in scientific research, we must prove that the technique has these properties.
Regarding reliability, a measuring instrument is reliable when we obtain measurements or data that represent the real value of the variable measured. Camillioni (10) states that reliability may indicate the extent to which there can be measurement errors and individual differences in the results obtained, as well as the extent to which the results show differences in the characteristics evaluated. In this study, after applying parallel tests (in mouth and in models), no significant differences were found, which renders both tests reliable.
Additionally, an instrument can be reliable but not valid (not measure what it intends to), which is not applicable in this case as the data obtained through measurements have been contrasted applying both methods. Both the direct and the indirect technique allow us to measure the mesio-distal distance of primary teeth in the lateral sector. We can thus have values expressed in mm to facilitate diagnosis, prognosis and a suitable treatment plan.
Hernández Sampieri (16) considers it fundamental that an instrument should be reliable and valid: if not, the results of the research should not be taken seriously. In this study, the results obtained showed that both measurement methods are valid and reliable. We agree with Brailosky (17): "Measurement instruments should be valid and reliable", which suggests that either method can be used in clinical research. The choice should be made according to the specific requirements of the study in question. In Pediatric Dentistry, both methods can be suitable depending on the child's behavior, since the indirect method requires taking an impression, which might not be an easy task. The direct method can also pose difficulties if the child does not behave as expected.
When the direct and indirect methods are used in children of school age to measure mesio-distal diameters of primary teeth, the probability of error in either method is minimal (less than 1%), which proves that both methods are reliable and valid.
Referencias
1. Moreno K, Meneses A, Morzan E. Dimensiones de arcos dentarios de niños de 4 a 8 años de edad con diferente estado nutricional. Talara- Piura. Rev. Estomatol Herediana 2004; 14(1-2):18-21.
2. Abu Alhaija ES, Qudeimat MA. Occlusion and tooth/arch dimensions in the primary dentition of preschool Jordanian children. Int J Pediatr Dent. 2003; 13:230-9
3. Almeida ER, Narvai PC, Frazao P, Guedes-Pinto AC. Revised criteria for the assessment and interpretation of oclusal desviations in the deciduos dentition: a public health perspective. Cad. Saúde Pública. 2008; 24(4):897-904
4. Galvão MAB, Dominguez GC, Tormin ST, Akamine A, Tortamano A, Fantini SM. Applicability of Moyers analysis in mixed dentition: A systematic review. Dental Press J Orthod 2013; 8(6):100-5.
5. Marin Manso G, Pérez MO, Califa M, Abdullah E, Al Shawi A, Hisham W, Abdullah A, Al Arshi M. Validación de la ecuación Tanaka–Johnston en una población de escolares yemenita. Revista Cubana de Estomatología. 2009; 46 (4): 23-31.
6. Moyers R. Manual de Ortodoncia. 4ed. Buenos Aires: Editorial Medica Panamericana, 1992: 125-130
7. Da Silva LPM, Gleiser R. Occlusal development between primary and mixed dentitions: a 5-year longitudinal study. J Dent Child (Chic). 2008; 75(3):287-294.
8. Pinto EM, Gondim PPC, Lima NS. Análise crítica dos diversos métodos de avaliação e registro das más oclusões. R Dental Press Ortodon Ortop Facial 2008; 13 (1): 82-91.
9. Bertoni A, Poggi M, Teobaldo M. Evaluación nuevos significados para una nueva práctica compleja. Buenos Aires: Kapeluz, 1996. p72.
10. Camilloni A. Las apreciaciones personales del profesor. Buenos Aires: Centro de Estudiantes de Filosofía y letras CCEFYL. Universidad de Buenos Aires, 1989.
11. Polit DF, Hungler BP. Investigación Científica en ciencias de la salud. 4ed. México: McGraw-Hill Interamericana, 2000. p404.
12. Lease LR, Sciulli PW. Brief Communication: Discrimination between European-American and African-American Children based on deciduous dental metrics and morphology. Am J Phys Anthropol 2005; 60: 126-56.
13. Anderson AA. Dentition and occlusion development in African American children: Mesiodistal crown diameters and tooth-size ratios of primary teeth. Pediatr Dent 2005; 27(2): 121-8.
14. Ngom PI, Diagne F, Idrissi Ouedghriri D, Idrissi Ouedghiri H. Comparative odontometric data between Moroccan and Senegalese. Odontostomatol Trop 2007; 30(117): 17-25.
15. Redondo AM, Barbería E. Tamaño mesiodistal, vestíbulolingual y altura de los primeros molares permanentes de una población española. Correlación con tamaños de las coronas preformadas utilizadas para su restauración. Gaceta Dental. 2008; 188:108-129.
16. Hernández Sampieri R. Metodología de la investigación. México: McGraw-Hill. 4ª Ed. Cap 9. 2006. p273-405.
17. Brailovsky C. Educación médica, evaluación de las competencias. En: Universidad de Buenos Aires. Facultad de Medicina. Aportes para un cambio curricular en Argentina 2001. Buenos Aires: UBA. Facultad de Medicina; OPS, 2001. p110.

