










Services on Demand
Journal

Article
 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Related links
Share

 Permalink
PermalinkCiencias Psicológicas
Print version ISSN 1688-4094On-line version ISSN 1688-4221
Cienc. Psicol. vol.18 no.1 Montevideo 2024 Epub June 01, 2024
https://doi.org/10.22235/cp.v18i1.3150
Original Articles
Exploring suicide stigma in the Peruvian population: a network analysis
1
 http://orcid.org/0000-0002-2604-7822
http://orcid.org/0000-0002-2604-7822
2
http://orcid.org/0000-0001-9976-1560
3
http://orcid.org/0000-0001-6025-8415
4
http://orcid.org/0000-0002-3062-328X
1 Universidad Científica del Sur, Perú, jbanos@cientifica.edu.pe
2 Universidad Peruana Unión, Perú
3 Universidad Ricardo Palma, Perú
4 Universidad César Vallejo, Perú
5 Universidad de San Martín de Porres, Perú
6 Universidad para el Desarrollo, Perú
The public stigma of suicide is a potential barrier to suicide prevention, an obstacle to seeking professional support, and impairs the psychological and physical well-being of affected individuals. The aim of the study was to analyze the association and centrality of public stigma of suicide in Peruvian adults from the general population. A total of 1013 adults (55.6 % women) responded to a suicide stigma questionnaire. A Gaussian network model was estimated, examining its global and local properties and comparing structures according to sex. The results showed stronger associations between noble and dedicated (r = .57), isolated and lonely (r = .47), immoral and an embarrassment (r = .41). The most central nodes and predictability were immoral, vindictive, a shame, lost, and irresponsible. In addition, for both women and men, the central node was immoral, although women described as vindictive and shameful, while men described as lonely and cowardly. In conclusion, there was evidence of stigmatizing attitudes towards people who die by suicide, with women and men presenting different perceptions. Suicide literacy programs can reduce public stigma in the general population.
Keywords: suicide; stereotype; adult; stigma; mental health literacy; network analysis
El estigma público del suicidio es una barrera potencial para su prevención, un obstáculo para la búsqueda de apoyo profesional y perjudica el bienestar psicológico y físico de las personas afectadas. El objetivo de este estudio fue analizar la asociación y centralidad del estigma público del suicidio en adultos peruanos de población general. Participaron 1013 adultos (55.6 % mujeres) que respondieron un cuestionario de estigma del suicidio. Se estimó un modelo de red gaussiano para examinar sus propiedades globales, locales y comparación de estructuras según sexo. Los resultados demostraron asociaciones más fuertes entre nobles y dedicadas (r = .57), aisladas y solitarias (r = .47), inmorales y una vergüenza (r = .41). Los nodos centrales y de predictibilidad fueron inmorales, vengativos, vergüenza, perdidos e irresponsables. Además, tanto para las mujeres y hombres, el nodo central fue inmorales, aunque las mujeres describieron como vengativos y una vergüenza, mientras que los hombres como solitarios y cobardes. En conclusión, se evidenció actitudes estigmatizantes hacia las personas que mueren por suicidio, en donde las mujeres y hombres presentan una percepción diferente. Los programas de alfabetización sobre el suicidio pueden reducir el estigma público en la población general.
Palabras clave: suicidio; estereotipo; adulto; estigma; alfabetización en salud mental; análisis de redes
O estigma público do suicídio é uma barreira potencial para a prevenção do suicídio, um obstáculo para a busca de apoio profissional, e prejudica o bem-estar psicológico e físico das pessoas afetadas. O objetivo do estudo foi analisar a associação e a centralidade do estigma público do suicídio em adultos peruanos da população em geral. Um total de 1.013 adultos (55,6% de mulheres) responderam a um questionário de estigma de suicídio. Foi estimado um modelo de rede gaussiana, examinando suas propriedades globais e locais e comparando estruturas segundo o sexo. Os resultados mostraram associações mais fortes entre nobres e dedicados (r = .57), isolados e solitários (r = .47), imorais e uma vergonha (r = .41). Os nós mais centrais e previsíveis foram imorais, vingativos, uma vergonha, perdidos e irresponsáveis. Além disso, tanto para as mulheres quanto para os homens, o nó central foi imorais, embora as mulheres hajam descrito como vingativos e uma vergonha, enquanto os homens como solitários e covardes. Em conclusão, são evidenciadas atitu des estigmatizantes em relação às pessoas que morrem por suicídio, com mulheres e homens tendo percepções diferentes. Os programas de alfabetização sobre o suicídio podem reduzir o estigma público na população em geral.
Palavras-chave: suicídio; estereótipo; adulto; estigma; alfabetização em saúde mental; análise de redes
Suicide is a persistent public health problem that continues to affect individuals, families, and communities in general. According to the World Health Organization (WHO), 703 000 people die by suicide each year, but it is emphasized that 77 % of those deaths are more frequent in low- and middle-income countries (WHO, 2021). In the Americas region, suicide is the third leading cause of death in young people aged 20-24 years, although people aged 45-59 years have the highest rate; similar results are reported in Peru, implying that suicide deaths is a complex problem involving any stage of development (Pan American Health Organization (PAHO), 2022; Roman-Lazarte et al., 2021). However, the figures are likely to be an underestimate because some suicides are classified as unintentional injuries. Despite this, the various efforts to identify risk and protective factors are important to address its complexity, given that there is no common cause attributed to suicide, but rather it emerges from the interaction between psychological, biological and sociocultural factors (O'Connor & Nock, 2014). In this scenario, professional health care, family environment and social support, are the first contact of help and support for an individual's communication or crisis situation. However, a systematic review on factors associated with seeking professional help for suicidal behaviors identified that one of the potential barriers was stigmatizing attitudes toward mental health problems, professional treatment, and suicide (Han et al., 2017).
Along the same lines, the WHO states that one of the obstacles to adequate suicide prevention is stigma (WHO, 2021). Although stigma is a complex construct with variable definitions, in the field of suicidology it has been defined as personal stigma and public stigma. The former is approached from the personal experience of the individual, where perception and experiences have consequences on the affected group, such as people bereaved by suicide and individuals with a personal or family history of suicidal behaviors (Baños-Chaparro, 2022; Sheehan et al., 2020). While public stigma is defined as society's negative attitudes, behaviors, and beliefs about suicide (Sheehan et al., 2017). The latter is of interest to the current study, given that suicide is not strictly a personal problem, but also a societal one. Members of a community or society occupy an important role in preventing suicide, especially in dealing with stigma and isolation (Fitzpatrick, 2015).
Recent general population-based studies identified public stigma as a barrier to suicide prevention, due to lack of awareness as a prominent public health problem and the spread of stereotypes (eg, "People who die by suicide are cowards"), prejudice (e.g., "I feel panicked if I go near that person who attempted suicide"), and discrimination (restriction of rights and opportunities) about suicide deaths (An et al., 2022; Sheehan et al., 2017; Oliffe et al., 2016). Research on suicide stigma in Australian general population described people who die by suicide as irresponsible and cowardly (stigma), lost, isolated and lonely (isolation), and brave and dedicated (glorification) (Batterham et al., 2013a). Another study in South Korea identified labels of incompetent, immoral, selfish, and deviant to society (An et al., 2022), while in Canada, support for the stereotypes of lost, lonely, isolated, and disconnected was evident (Oliffe et al., 2016). In addition, there appears to be differential behavior with respect to sex, where men consider people who die by suicide to be weak, cowardly, and conceptualize suicide as a shameful and sinful act (Pereira & Cardoso, 2018), while women consider them to be disconnected, lost, and lonely (Oliffe et al., 2016).
In this sense, it is important to raise awareness in the general community and reduce stigma so that the society of a given country can make progress in suicide prevention. Recent advances in the field of psychology are driven by the network model, an alternative approach to the biomedical model. In this regard, the biomedical model holds that signs and symptoms are grouped together because they share a common cause, i.e., the underlying disease entity (Borsboom & Cramer, 2013). In contrast, the network approach to psychopathology indicates that disorder is an emergent phenomenon that arises from the interactions of symptoms and their tendency to causally reinforce each other (Isvoranu et al., 2022). From this perspective, a disorder is not a latent entity that causes the emergence and covariation of symptoms (biomedical model), rather the symptoms and the associations between them, are the disorder itself (Borsboom & Cramer, 2013). By way of introduction, a network structure is composed of nodes (symptoms, attitudes, and so on) and edges (correlations). Therefore, network analysis is not only restricted to symptoms and the comorbidity between them, but also incorporates an individual's attitudes and traits (Baños-Chaparro et al., 2022; Dalege et al., 2017; Ramos-Vera et al., 2022) and physical problems (Ramos-Vera et al., 2021), extending the network architecture from psychology to medicine (Isvoranu et al., 2021).
In a brief review of the literature, we found no evidence of analysis of suicide stigma at any stage of development from a network approach. Given that evidence suggests that suicide stigma is found to be more prevalent in the general population and, even more so, with low or very low levels of education (Batterham et al., 2013a; Park et al., 2015), we chose to explore this construct in the general population without completed higher education. The general objective of the research was to analyze the association and centrality of public stigma of suicide in Peruvian adults from the general population. In addition, as a specific objective, a comparison of networks according to sex was carried out to verify differences linked to the public stigma of suicide.
Materials and methods
Design
The purpose of the research was to analyze the conditional associations of the variables (nodes) included in the network. In that sense, the research design is non-experimental and quantitative approach, being basic, cross-sectional and associative (Ato et al., 2013).
Participants
A total of 1013 Peruvian adults participated in the study, selected by non-probabilistic convenience sampling with the following inclusion criteria: a) age 18 years or older, b) residing in Metropolitan Lima, c) not having completed higher education (technical, university or postgraduate) and d) acceptance of informed consent.
In this sense, the participation of women (55.6 %) and men (44.4 %) was similar and the average age was 35 years (SD = 13.2) in a range of 18 to 89 years. In relation to the characteristics of the participants, there was a high percentage of singles (42 %), followed by married (23.4 %) and cohabitants (22.5 %). The predominant level of education was completed secondary school (48.4 %), incomplete technical (20.4 %) and incomplete university (11.4 %), and the majority had a current job (78.4 %) and lived in an urban area (70.8 %). Likewise, 66.6 % indicated that they did not have a chronic illness, had not consumed alcohol in the last 12 months (72.5 %), had no outstanding financial debts (69.2 %) and had not been fired (64.6 %) or demoted (71.4 %) at work at some time in their lives.
Instrument
Sociodemographic questionnaire. A section was prepared to collect sociodemographic information on the participants, where the following questions were asked: sex, age, marital status, level of education, job, area of residence, chronic disease, alcohol consumption in the last 12 months, outstanding financial debts and whether they had been fired or demoted from their jobs.
Stigma of Suicide Scale - Short Form (SOSS-SF). The scale consists of 16 items and assesses public stigma towards suicide through three dimensions (stigma, isolation and glorification) developed in Australia (Batterham et al., 2013b) and translated into Spanish in the Peruvian population (Baños-Chaparro et al., 2023). In that sense, each item consists of a description of a word linked to a person who dies by suicide (e.g., "In general, people who die by suicide are irresponsible"), with five response options (from 1: strongly disagree to 5: strongly agree). Total scoring is done for each dimension and high scores indicate greater stigma toward people who die by suicide. In this study, acceptable reliability was obtained for the stigma dimension (ω = .88), isolation (ω = .83) and glorification (ω = .77).
Procedure
The collection of information was carried out in person during September and October 2022 in the various districts of Metropolitan Lima and respecting the current recommendations on Covid-19. Four recruiters (FLD, DJR, JMC, PYL) trained in the survey content and format explained to each participant the objective of the research, the anonymity of their responses, voluntary participation, the confidentiality of the information collected, and the freedom to leave the study at any time. The order of presentation of the survey was informed consent, demographic questions, and psychological instrument. The survey was given to adults who signed the informed consent form and received no financial reward.
Data analysis
Initially, the descriptive statistics of central tendency (arithmetic mean) and dispersion (standard deviation) of the items were explored. Likewise, the internal consistency of its total score was evaluated through a structural equation method (omega coefficient) for each dimension, with acceptable values greater than .70 (McDonald, 1999). Along the same lines, prior to the analysis of a network structure, the topological overlap of the nodes was examined, determining a redundancy greater than 25 % with a p-value of .05 to determine statistical significance (Jones et al., 2021).
From the preliminary analyses, a network was constructed using a pairwise Markov random field (PMRF) which is a class of undirected network models where variables are represented by nodes connected by edges (blue lines are positive correlations and red lines are negative correlations) that indicate the conditional association between two variables after controlling for all other variables in the network (Isvoranu et al., 2022). Given the ordinal nature of the items, a graphical Gaussian model (GGM) quantifying edges with partial correlation coefficients was estimated and Spearman's correlation method, recommended for non-normally distributed data, was employed (Isvoranu & Epskamp, 2021). To ensure a sparse and interpretable model, the graphical absolute minimum selection and shrinkage operator (GLASSO; Friedman et al., 2008) algorithm was used in combination with the extended Bayesian information criterion (EBIC; Chen & Chen, 2008), with a fit parameter set at γ = .50, commonly recommended for estimating multivariate GGM models (Isvoranu et al., 2022). For the network design, the Fruchterman-Reingold algorithm was used, which uses an iterative process to calculate a layout such that the most connected nodes will be pulled towards the center of the network and the most disconnected nodes will be placed at the periphery of the network (Fruchterman & Reingold, 1991).
Subsequently, the network architecture was analyzed through its global properties (inference in the general network) and local properties (inference in specific parts of the network). Regarding the global metrics, the organization of nodes was explored through the transitivity (C△) that determines the average global clustering of nodes in a network and, as well, the average properties of edges through the average shortest path length (APL) that quantifies the average of the shortest distances between each pair of nodes (Isvoranu et al., 2022). Since some network structures may have high node clustering but low APL, the small-world index (S) was calculated which assesses the degree of association between nodes, with S > 1 being recommended (Humphries & Gurney, 2008). Regarding local metrics, the centrality of nodes was analyzed through the expected influence, which considers the edges of a node with another node in opposite directions and, the predictability, which calculates the explained variance (R2) of each node (Haslbeck & Waldorp, 2018).
On the other hand, a precision and stability analysis of the estimated network model was carried out. Regarding accuracy, the nonparametric bootstrapping method based on 1000 samples was applied to construct the 95 % confidence intervals (CI) of the weights of the network edges. While, in the stability analysis for the expected influence index, it was performed using the case-dropping bootstrap procedure, which removes participants from the data iteratively (e.g., 10 %, 20 %, and so on). This method can be summarized by the correlation stability coefficient (CS), which should be greater than .25 and preferably greater than .50 (Isvoranu et al., 2022). Whereas, to assess differences between independent groups (e.g., females vs. males), a network comparison test (NCT; van Borkulo et al., 2022) based on 1000 random permutations was applied. This process was performed based on network structure invariance using the M statistic and global strength invariance using the S statistic. The statistical process was performed in the free software Rstudio version 4.1.1 with the packages bootnet, qgraph, psych, mgm, careless, MBESS, Network Comparison Test and networktools (Epskamp et al., 2018; Haslbeck & Waldorp, 2020; Jones, 2021; Kelley, 2007; Revelle, 2018, van Borkulo et al., 2022).
Ethical considerations
The present study respected the guidelines of the Declaration of Helsinki and the code of ethics mentioned in chapter three for good research practices of the College of Psychologists of Peru (2017). All participants were informed about the conditions of anonymity, confidentiality and voluntariness of participation.
Results
Global and local properties of the network structure
In relation to central tendency and dispersion, it was observed that the mean was located between item 15 (M = 2.53) and item 10 (M = 3.24), while item 5 presented the highest standard deviation (SD = 1.12) (Table 1). In the analysis of topological overlap there were no suggestions, showing the absence of redundancy among the nodes included in the network.
In terms of global structure, an APL of 1.5, a C△ of .60 and, therefore, an S-index of 1.29 were observed, considering a small-world network topology. In Table 1, one can observe the properties of the local structure, the most central nodes according to the expected influence (EI) were immoral (EI = 1.14), vindictive (EI = .98), an embarrassment (EI = .96) and lost (EI = .94). Likewise, the mean predictability was 47.2 %, locating the highest predictability in the immoral (63.3 %), a shame (62.2 %), vindictive (59.3 %), isolated (58.5 %) and irresponsible (58.4 %) nodes.
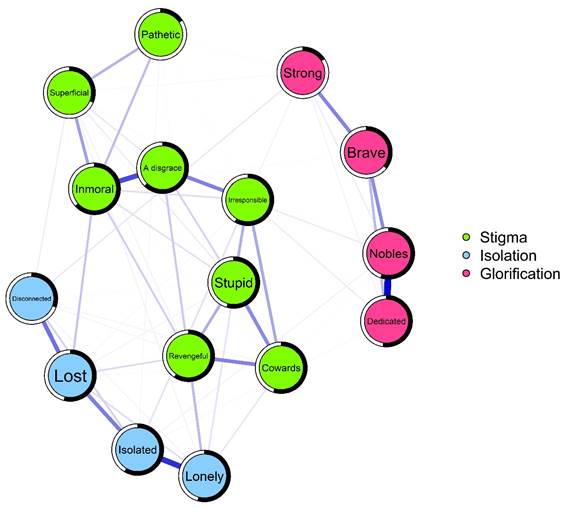
The network structure of suicide stigma is presented in Figure 1. In that sense, it is evident that the network model had a connectivity of 6.55, density .05 and a number of connections of 62, where 51 are positive and 11 negative edges. In addition, it is observed that the strongest conditional associations arose between noble and dedicated (r= .57), isolated and lonely (r= .47), immoral and an embarrassment (r = .41). Similarly, to a lesser magnitude, lost and disconnected (r = .32), isolated and lost (r = .29), as well as a shame and irresponsible (r = .28).
Table 1: Item content, descriptive statistics and local network properties
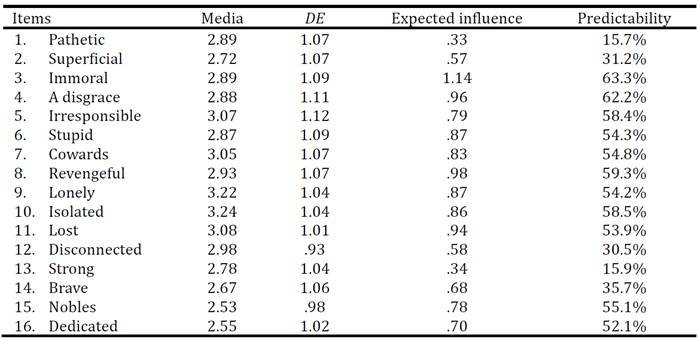
Note:SD: standard deviation.
Accuracy of the network structure and stability of the centrality index
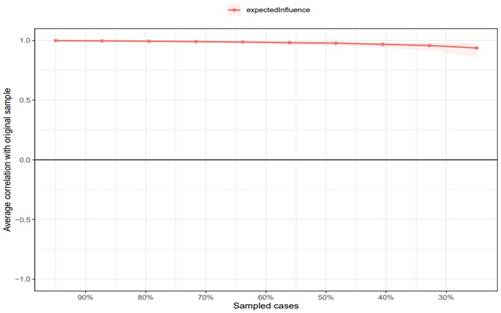
Overall, the bootstrap CIs for the edges were narrow and, for the most part, non-overlapping (Figure 2). In addition, the estimate of the EI index was stable, with a CS coefficient ≈ .75, which suggests that 75 % of the data could be removed to retain a 95 % certainty of a .70 correlation with the original data set (Figure 3).
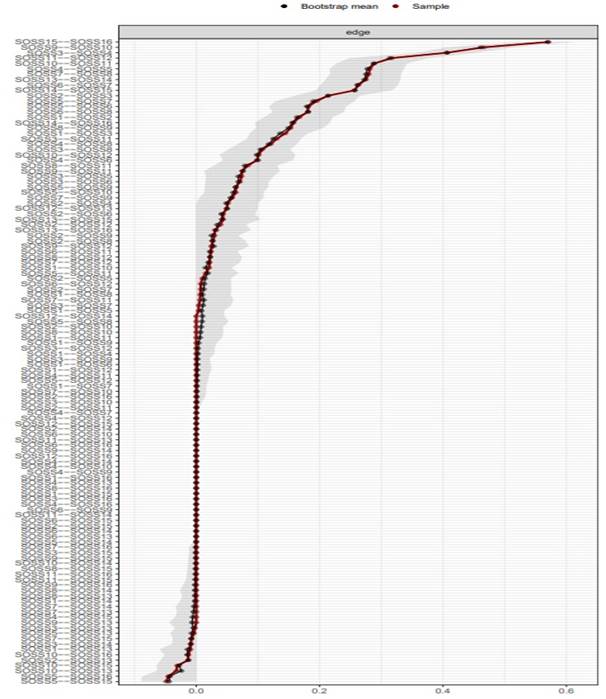
Figure 2: Nonparametric bootstrap nonparametric confidence intervals of estimated edges for suicide stigma
Comparative analysis of networks by gender
In Figure 4, the global characteristics between the network of women (n = 563) and men (n = 450) are reported. The invariance test based on their structure indicated that they were not significantly different (M = .151, p = .367) and neither at the overall strength level (S = .239, p = .481). In fact, the correlation between both network structures is similar (r = .92). Regarding EI, for both women and men, the central node was immoral (EIwomen = 1.08, EImen = 1.19). However, other central nodes were evident for women as vindictive (EI = 1.05) and an embarrassment (EI = 1.02), while for men they were lonely (EI = .97) and cowardly (EI = .90).

Discussion
For adequate suicide prevention, it is important to identify potential barriers that are a relevant factor in the general community. Among the various barriers, public stigma of suicide is a prominent problem today. In this research, we analyzed the public stigmatizing attitudes of suicide in the general population and assessed the differences in stigma between women and men.
In relation to the global properties of the network, the analysis shows that the different descriptions of people who die by suicide were not redundant (absence of overlap) and maintained adequate connectivity. In this regard, the strongest conditional associations emerged between noble and dedicated (glorification), isolated and lonely (isolation), immoral and a disgrace (stigma). Although there are no other studies from the network approach, the relationships found represent the multidimensionality of the construct and agree with the scientific literature in describing public stigma attitudes to suicide as a complex and pervasive problem in contemporary society. One qualitative study found that suicide-related stigma was linked to a lack of awareness and education, further attributing deaths in terms of stigma and isolation (Monteith et al., 2020), while another study highlights that stereotypes and prejudice were more prevalent in people who attempted suicide (Sheehan et al., 2017). This suggests that social interactions based on shared principles and beliefs give rise to stigmatizing attitudes towards people who attempt or die by suicide in a society and, consequently, public stigma could internalize into personal stigma, where those affected see themselves as noble, dedicated, an embarrassment or cowards (Batterham et al., 2013a, Sheehan et al., 2017).
On the other hand, the local properties indicated a greater centrality for descriptions such as immoral, vindictive, a shame and lost, similar results were found for predictability, although additionally the descriptions of isolated and irresponsible were highlighted. This indicates that most of those descriptions were the ones that were most strongly connected with the rest of the nodes included in the network and that such attitudes are the most representative in the study population. The findings are in line with other previous work, where a general Australian community describes people who die by suicide as irresponsible, lost and isolated (Batterham et al., 2013a), in South Korea as immoral and vindictive (An et al., 2022), while in Canada they qualify as lost, isolated and lonely (Oliffe et al., 2016), being necessary to consider in literacy programs, those descriptions to reduce the public stigma of suicide in such population and mitigate these attributions aimed at a concept of isolation and stigma in affected people.
Along the same lines, in the comparison of networks according to gender, it was identified that both structures were similar in terms of association and connectivity. However, when exploring the most central nodes in the network, it was found that although both genders shared a similar attitude (immoral), they differed in other descriptions such as vengeful and shameful (women) and lonely and cowardly (men). This coincides with the literature where men mostly denominate suicide as an act of cowardice and weakness to face life's problems (Pereira & Cardoso, 2018), a different perception to women where deaths by suicide are qualified as a manifestation of revenge, disconnected and lost in the world, as well as an action of shame for the resolution of conflicts, being a stigmatizing attitude more prevalent in adulthood (Oliffe et al., 2016; Pereira & Cardoso, 2018).
In this context, suicide is a public health problem that continues to be affected by public stigma in contemporary societies. Several studies based in culturally different countries have reported high levels of stigmatizing attitudes towards people who die by suicide (An et al., 2022; Batterham et al., 2013a; Oliffe et al., 2016; Pereira & Cardoso, 2018), which involves a great challenge for health professionals and general community worldwide. The implications of the study provide insight into the attitudes of the general Peruvian adult population about suicide, and this knowledge is fundamental for the development of strategies aimed at decreasing public stigma. A growing body of research highlights that social campaigns or suicide prevention programs aimed at the general community, families, health professionals and affected individuals, based on literacy orientations, associated factors, treatment and preventive actions, can reduce the public stigma of suicide, promote social support or health professional care seeking and decrease suicide deaths (de Matos e Souza & Bisol, 2021; van der Burgt et al., 2021). This would overcome the barrier to seeking treatment and combat the idea to the stigmatized person that the best solution to their problems and suffering is suicide, in addition to stereotypes and prejudices. On this basis, the findings would also serve as a source of meaningful and evidence-based information to promote a national suicide prevention plan in the Peruvian context, starting from a multisectoral approach in coordination with governmental and nongovernmental agencies at the national level and in each province led by a ministry of health, whose principle and purpose is to address the complexity of suicidal behaviors from an individual, community and social category (Baños-Chaparro et al., 2021).
Finally, despite the strengths of the study, such as its statistical method employed, considerable sample size and initial information on the public stigma of suicide in the general Peruvian population, it is necessary to recognize some limitations in the study. First, the sampling method was by convenience and inclusion criteria, which may not be representative for the entire general adult population of Peru, suggesting not to extend the findings to other stages of development (e.g., adolescents), adults with completed higher education and other departments of the country. Second, the current analysis was based on cross-sectional data; therefore, it is not possible to infer causality, i.e., the directions of the edges. The exploratory results of this study could be confirmed with directed network analysis. Third, the information collected was from self-report scores, which may limit capturing a psychological phenomenon. Fourth, the analyses were based on the public stigma of suicide, with the personal stigma of suicide needing to be explored and the analyses replicated. The network structure and attitudes towards this group of people are likely to be very different in terms of stereotypes, prejudice and discrimination. Fifth, a fundamental aspect is the scarcity of dissemination of information and education on public stigma about suicide, accompanied by taboo, myths and the absence of a national suicide prevention plan. Lack of disclosure may be an important factor in the estimation of public stigma of suicide. However, the current study allows reducing this gap by providing empirical evidence on the subject and making its relevance in contemporary society visible.
Conclusion
Negative cultural beliefs and attitudes towards people who die by suicide not only affect the family and social environment of the deceased, but also in the advancement of suicide prevention in a society, since it is an obstacle to seeking professional help, detracts from suicide as an important public health problem, and impairs the psychological and physical well-being of stigmatized individuals.
The findings of the study showed stigmatizing attitudes towards people who die by suicide, with women and men who do not have completed higher education showing a different perception. Social campaigns and suicide literacy prevention programs can reduce public stigma in the general population without higher education, promote social and professional support, and reduce suicide deaths. Considering the different perceptions of men and women in such strategies would be an appropriate method to address the public stigma of suicide. In that sense, health professionals, social scientists and society in general play an important role in suicide prevention. Suicide deaths are preventable and a better understanding of the stigma in a country without a national plan or policy on suicide is an initial but very important step for education, prevention and intervention in the Peruvian national context.
REFERENCES
An, S., Lee, H., Lee, J., & Kang, S. (2022). Social stigma of suicide in South Korea: A cultural perspective. Death Studies, 1-9. https://doi.org/10.1080/07481187.2022.2051096 [ Links ]
Ato, M., López, J. J., & Benavente, A. (2013). Un sistema de clasificación de los diseños de investigación en psicología. Anales de Psicología, 29(3), 1038-1059. http://doi.org/10.6018/analesps.29.3.178511 [ Links ]
Baños-Chaparro, J. (2022). Duelo por suicidio: ¿Qué sucede después en la familia? Revista de Investigación en Psicología, 25(1), 159-170. https://doi.org/10.15381/rinvp.v25i1.22287 [ Links ]
Baños-Chaparro, J., Lamas Delgado, F., Ynquillay-Lima, P., Jacobi-Romero, D. J., & Fuster Guillen, F. G. (2022). Análisis de red de la comorbilidad entre síntomas de ansiedad e insomnio en adultos. Revista Cubana de Medicina Militar, 51(2), e02201891. [ Links ]
Baños-Chaparro, J., López-Vega, D. J., Lamas Delgado, F., Jacobi-Romero, D. J., Marín-Contreras, J., & Ynquillay-Lima, P. (2023). Traducción y validez del Stigma of Suicide Scale Short Form (SOSS-SF) en población peruana. Revista Cubana de Medicina Militar, 52(2), e02302553. [ Links ]
Baños-Chaparro, J., Ynquillay-Lima, P., Lamas Delgado, F., & Fuster Guillen, F. G. (2021). Análisis de redes de las conductas suicidas en adultos peruanos. Revista Cubana de Medicina Militar, 50(3), e02101450. [ Links ]
Batterham, P. J., Calear, A. L., & Christensen, H. (2013a). Correlates of suicide stigma and suicide literacy in the community. Suicide and Life-Threatening Behavior, 43(4), 406-417. https://doi.org/10.1111/sltb.12026 [ Links ]
Batterham, P. J., Calear, A. L., & Christensen, H. (2013b). The Stigma of Suicide Scale: Psychometric properties and correlates of the stigma of suicide. Crisis: The Journal of Crisis Intervention and Suicide Prevention, 34(1), 13-21. https://doi.org/10.1027/0227-5910/a000156 [ Links ]
Borsboom, D., & Cramer, A. (2013). Network analysis: An integrative approach to the structure of psychopathology. Annual Review of Clinical Psychology, 9, 91-121. https://doi.org/10.1146/annurev-clinpsy-050212-185608 [ Links ]
Chen, J., & Chen, Z. (2008). Extended Bayesian information criteria for model selection with large model spaces. Biometrika, 95(3), 759-771. https://doi.org/10.1093/biomet/asn034 [ Links ]
Colegio de Psicólogos del Perú. (2017). Código de ética y deontología. http://api.cpsp.io/public/documents/codigo_de_etica_y_deontologia.pdf [ Links ]
Dalege, J., Borsboom, D., van Harreveld, F., & van der Maas, H. L. (2017). Network analysis on attitudes: A brief tutorial. Social Psychological and Personality Science, 8(5), 528-537. https://doi.org/10.1177/1948550617709827 [ Links ]
De Matos e Souza, F. G., & Bisol, L. W. (2021). Suicide prevention in Brazil: General concepts and the experience of a life support program (PRAVIDA). Current Research in Psychiatry, 1(2), 27-30. https://doi.org/10.46439/Psychiatry.1.010 [ Links ]
Epskamp, S., Borsboom, D., & Fried, E. I. (2018). Estimating psychological networks and their accuracy: A tutorial paper. Behavior Research Methods, 50, 195-212. https://doi.org/10.3758/s13428-017-0862-1 [ Links ]
Fitzpatrick, S. J. (2015). Suicidology as a social practice. Social Epistemology, 29(3), 303-322. https://doi.org/10.1080/02691728.2014.895448 [ Links ]
Friedman, J. H., Hastie, T., & Tibshirani, R. (2008). Sparse inverse covariance estimation with the graphical lasso. Biostatistics, 9(3), 432-441. https://doi.org/10.1093/biostatistics/kxm045 [ Links ]
Fruchterman, T. M., & Reingold, E. M. (1991). Graph drawing by force-directed placement. Journal of Software: Practice and Experience, 21(11), 1129-64. https://doi.org/10.1002/spe.4380211102 [ Links ]
Han, J., Batterham, P. J., Calear, A. L., & Randall, R. (2017). Factors Influencing Professional Help-Seeking for Suicidality: A Systematic Review. Crisis: The Journal of Crisis Intervention and Suicide Prevention, 39(3), 175-196. https://doi.org/10.1027/0227-5910/a000485 [ Links ]
Haslbeck, J. M., & Waldorp, J. (2020). mgm: Estimating time-varyinf mixed graphical models in high-dimensional data. Journal of Statistical Software, 93(8), 1-46. https://doi.org/10.18637/jss.v093.i08 [ Links ]
Haslbeck, J. M., & Waldorp, L. J. (2018). How well do network models predict observations? On the importance of predictability in network models. Behavior Research Methods, 50, 853-861. https://doi.org/10.3758/s13428-017-0910-x [ Links ]
Humphries, M. D., & Gurney, K. (2008). Network ‘Small-World-Ness’: A quantitative method for determining canonical network equivalence. PLoS ONE, 3(4), e0002051. https://doi.org/10.1371/journal.pone.0002051 [ Links ]
Isvoranu, A. M., & Epskamp, S. (2021). Which estimation method to choose in network psychometrics? Deriving guidelines for applied researchers. Psychological Methods. https://doi.org/10.1037/met0000439 [ Links ]
Isvoranu, A. M., Abdin, E., Chong, S. A., Vaingankar, J., Borsboom, D., & Subramaniam, M. (2021). Extended network analysis: from psychopathology to chronic illness. BMC Psychiatry, 21(1), 119. https://doi.org/10.1186/s12888-021-03128-y [ Links ]
Isvoranu, A. M., Epskamp, S., Waldorp, L. J., & Borsboom, D. (2022). Network psychometrics with R. Routledge. [ Links ]
Jones, P. J., Ma, R., & McNally, R. J. (2021). Bridge centrality: A network approach to understanding comorbidity. Multivariate Behavioral Research, 56(2), 353-367. https://doi.org/10.1080/00273171.2019.1614898 [ Links ]
Kelley, K. (2007). Methods for the behavioral, educational, and social sciences: An R package. Behavior Research Methods, 39, 979-984. https://doi.org/10.3758/BF03192993 [ Links ]
McDonald, R. P. (1999). Test theory: A unified treatment. Lawrence Erlbaum Associates. [ Links ]
Monteith, L. L., Smith, N. B., Holliday, R., Dorsey Holliman, B. A., LoFaro, C. T., & Mohatt, N. V. (2020). “We're Afraid to Say Suicide”: Stigma as a barrier to implementing a community-based suicide prevention program for rural veterans. The Journal of Nervous and Mental Disease, 208(5), 371-376. https://doi.org/10.1097/NMD.0000000000001139 [ Links ]
O'Connor, R. C., & Nock, M. K. (2014). The psychology of suicidal behaviour. The Lancet Psychiatry, 1(1), 73-85. https://doi.org/10.1016/S2215-0366(14)70222-6 [ Links ]
Oliffe, J. L., Ogrodniczuk, J. S., Gordon, S. J., Creighton, G., Kelly, M. T., Black, N., & Mackenzie, C. (2016). Stigma in male depression and suicide: A Canadian sex comparison study. Community Mental Health Journal, 52, 302-310. https://doi.org/10.1007/s10597-015-9986-x [ Links ]
Organización Mundial de la Salud. (2021). Suicidio. https://www.who.int/es/news-room/fact-sheets/detail/suicide [ Links ]
Organización Panamericana de la Salud. (2022). Prevención del Suicidio. https://www.paho.org/es/temas/prevencion-suicidio [ Links ]
Park, S., Kim, M. J., Cho, M. J., & Lee, J. Y. (2015). Factors affecting stigma toward suicide and depression: A Korean nationwide study. International Journal of Social Psychiatry, 61(8), 811-817. https://doi.org/10.1177/0020764015597015 [ Links ]
Pereira, A. G., & Cardoso, F. M. (2018). Stigmatising attitudes towards suicide by gender and age. CES Psicología, 12(1), 1-16. https://doi.org/10.21615/cesp.12.1.1 [ Links ]
Ramos-Vera, C., Baños-Chaparro, J., & Ogundokun, R. O. (2021). The network structure of depressive symptomatology in Peruvian adults with arterial hypertension. F1000Research, 10, 19. https://doi.org/10.12688/f1000research.27422.2 [ Links ]
Ramos-Vera, C., Serpa-Barrientos, A., Baños-Chaparro, J., Vallejos-Saldarriaga, J., & Saintila, J. (2022). Enneagram typologies and healthy personality to psychosocial stress: A network approach. Frontiers in Psychology, 13, 1051271. https://doi.org/10.3389/fpsyg.2022.1051271 [ Links ]
Revelle, W. (2018). Psych: Procedures for Personality and Psychological Research. Northwestern University. [ Links ]
Roman-Lazarte, V., Moncada-Mapelli, E., & Huarcaya-Victoria, J. (2021). Evolución y diferencias en las tasas de suicidio en Perú por sexo y por departamentos, 2017-2019. Revista Colombiana de Psiquiatría, 50(1), 1-8. https://doi.org/10.1016/j.rcp.2021.03.005 [ Links ]
Sheehan, L., Dubke, R., & Corrigan, P. W. (2017). The specificity of public stigma: A comparison of suicide and depression-related stigma. Psychiatry Research, 256, 40-45. https://doi.org/10.1016/j.psychres.2017.06.015 [ Links ]
Sheehan, L., Oexle, N., Dubke, R., Ting Wan, H., & Corrigan, P. W. (2020). The self-stigma of suicide attempt survivors. Archives of Suicide Research, 24(1), 34-57. https://doi.org/10.1080/13811118.2018.1510797 [ Links ]
van Borkulo, C. D., Boschloo, L., Kossakowski, J., Tio, P., Schoevers, R., Borsboom, D., & Waldorp, L. (2022). Comparing network structures on three aspects: A permutation test. Psychological Methods . https://doi.org/10.1037/met0000476 [ Links ]
van der Burgt, M. C., Beekman, A. T., Hoogendoorn, A. H., Berkelmans, G., Franx, G., & Gilissen, R. (2021). The impact of a suicide prevention awareness campaign on stigma, taboo and attitudes towards professional help-seeking. Journal of Affective Disorders, 279, 730-736. https://doi.org/10.1016/j.jad.2020.11.024 [ Links ]
How to cite: Baños-Chaparro, J., Aranda-Turpo, J., Lamas Delgado, F., Jacobi-Romero, D. J., Marín-Contreras, J., & Ynquillay-Lima, P. (2024). Exploring suicide stigma in the Peruvian population: a network analysis.Ciencias Psicológicas, 18(1), e-3150. https://doi.org/10.22235/cp.v18i1.3150
Authors’ contribution (CRediT Taxonomy): 1. Conceptualization; 2. Data curation; 3. Formal Analysis; 4. Funding acquisition; 5. Investigation; 6. Methodology; 7. Project administration; 8. Resources; 9. Software; 10. Supervision; 11. Validation; 12. Visualization; 13. Writing: original draft; 14. Writing: review & editing. J. B. CH. has contributed on 1, 3, 5, 6, 7, 12, 13, 14; J. A. T. in 1, 5, 6, 11, 13, 14; F. L. D. in 2, 5, 13, 14; D. J. J. R. in 5, 13, 14; J. M. C. in 5, 13, 14; P. Y. L. in 10, 13, 14.
Received: December 19, 2022; Accepted: February 01, 2024
 Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
