











 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo

 Permalink
Permalink
By January 2022, the United States of America had little more than 4 million breast cancer survivors (American Cancer Society, 2022). In Mexico, the National Cancer Institute (INCan) has a registry of 3,800 survivors until 2019, of which about 48 % are from breast cancer and 79% have a survival greater than 5 years (Instituto Nacional de Cancerología, 2018).
The fear of recurrence is one of the main affectations with prevalence ranging from 39 % to 97 % of which more than 80 % report moderate or high levels of this fear (Fiszer et al., 2014; Merckaert et al., 2017; National Comprehensive Cancer Network (NCCN), 2022; Park & Lim, 2022; Simard et al., 2013). Unlike some anxiety disorders, fear of recurrence is a response to a real threat, and this particular fear is experienced by many survivors up to 10 years after completing treatments (Thewes et al., 2012).
There are several instruments that assess fear of cancer recurrence among which The Concerns About Recurrence Scale (CARS; Vickberg, 2003) stands out because it´s the only one designed specifically for breast cancer survivors.
The original version through an exploratory factor analysis was formed by 26 items distributed in four factors significantly correlated with each other that explained 70% of the variance and evaluated the specific concerns about the recurrence. Two validations of the scale have been published in breast cancer survivor populations, one Japanese (Momino et al., 2014) with 26 items and four factors with two of them renamed as “Self-concept” and “Roles”. The other one is a Dutch version (van den Beuken-van Everdingen et al., 2008) who also identified four factors but a total of 20 items. Both versions showed significant correlations between factors, adequate internal consistency (Japan: α = .85 to .94; Dutch: α = .94 overall fear, α = .88 to .94 by subscales) and evaluated convergent validity with The Hospital Anxiety and Depression Scale (HADS) but only the Dutch version has a confirmatory factor analysis with adequate fit indices (SRMR = 0.088, CFI = .956).
Based on this data and the lack of evidence about the use of the CARS in Latin America, we considered necessary to comply with the objective of examine the internal consistency, confirmatory factorial structure, and convergent validity of the CARS in Spanish for Mexico for its future clinical use in this population with the explicit approval of the entire process by the original author Suzanne M. Johnson Vickberg.
Method
Design
An instrumental study carried out at the Breast Tumor Clinic of The National Cancer Institute of México. The scale adaptation procedure was by translation, re-translation. The original English version was translated into Spanish by two certified translators with knowledge in the areas of health psychology and psychology. Then, the Spanish version was sent to a third bilingual expert for its re-translation to English. Since there were no differences in the wording with the original scale, an adequate translation was confirmed to proceed to evaluation by judges for validity check (Mora-Ríos et al., 2013). Fifteen judges’ experts in psychology, health psychology, medicine and nursing (with experience in oncology) evaluated the understanding of the items, instructions and response options based on the criteria of writing, relevance, content validity, face validity, theoretical validity and language appropriate for the population of this Spanish version.
From this judgment the following changes were made: a synthesis of instructions, wording modification in the item 12 (“Threaten my identity, how I see myself” to “Affect how I see myself”), and two wording proposals for the last answer option (very much or extremely). Content validity was agreed for all items as well as face validity, theoretical validity and appropriate language for the population.
Then, proceed to the pilot test with the population of interest (Carretero Dios & Pérez Meléndez, 2005). The pilot test was carried out in a sample of 30 participants according to the international guidelines of Koller et al. (2007) to assess difficulty, confusion or offensive questions, comprehension of item 12 was confirmed with the new redaction, as well as the answer option extremely as more understandable.
Participants
Through intentional sampling, 200 participants (30 additional for a pilot test) were selected based on the criteria for choosing the sample of Nunnally and Bernstein (1995), who suggest 5 to 10 subjects by item, and Hernández Sampieri et al. (2016), which establish a criterion of 30 to 60 participants for pilot test. Women over 18 years of age, with a confirmed diagnosis of breast cancer (stages 0-III), who had completed cancer treatment (although they could be receiving hormonal treatment), had started surveillance phase and who voluntarily agreed to participate in the study were included. The study was approved by the Research Committee and the Research Ethics Committee of the hospital where the study was conducted under registration number (019/067/POI) (CEI/1345/18). The data collection was carried out through the review of electronic files and directly with patients from November 2019 to March 2020.
Measures
Clinical identification card prepared ad hoc for this study to collect sociodemographic and clinical data of the participants such as age, marital status, confirmed diagnosis, received treatments, etc.
Concerns About Recurrence Scale (CARS) (Vickberg, 2003). Consisting of 30 questions: four questions with 6 Likert-type response options to evaluate general fear of recurrence and 26 questions that conform four factors: concerns about health, concerns about womanhood, concerns about roles, and concerns about death; with five response options ranging from 0 (not at all) to 4 (extremely) to determine specific concerns about recurrence. Overall fear index showed general reliability of α = .87 and by subscale from α = .89 to α = .94.
Hospital Anxiety and Depression Scale for Mexican oncological population (HADS-M) (Galindo Vázquez et al., 2015). Version validated and adapted for the Mexican oncological population, it’s a self-applied 12-item questionnaire with four Likert-type response options with a total satisfactory Cronbach α coefficient of .86 and specific of .79 for anxiety and .80 for depression. The cut-off points indicate, from zero to five, clinical absence of anxiety or depression, from 6-8 mild anxiety/depression, from 9 to 11 moderate anxiety/depression and from 12 onwards severe anxiety/depression.
Procedure
Potential participants were identified through the hospital's electronic record system to verify inclusion criteria, then, were recruited in the waiting room of the Breast Tumor Clinic of The National Cancer Institute of México. After explanation of the research and the inclusion criteria, each decided to participate freely under the signature of the informed consent and answered the questionnaires with the support of a researcher.
Analysis of data
Given that the distribution of items and factors of the scale have been previously adjusted with the theory, the purpose of making the confirmatory factorial analysis (CFA) was to corroborate the structure of the instruments according to its theoretical model, which represents a methodological contribution to the instrument.
According to Finney and DiStefano (2006), who suggest that if the observed data have many categories, at least five response options and a distribution close to normal, the CFA was carried out using the maximum likelihood model and the evaluation of the fit of the model was based on the fit indices mean square error of approximation (RMSEA = .50-.80), standardized root mean squared residual (SRMR ≤ 0.08); as well as the CFI and TLI ≥ .90 values (Batista-Foguet et al., 2004; Herrero, 2010; Morata-Ramirez et al., 2015).
Cronbach's alpha reliability index was considered for the total scale and each factor, and the convergent validity was evaluated through Pearson's correlation with the HADS Scale considering a significance level of p < .05.
Using quartiles, the cutoff points for each factor were established. The original version of the scale (Vickberg, 2003) designated scores below the 25th quartile as being of no concern, scores between the 26th and 50th percentile as being of little or some concern, scores between the 51st and 75th percentile as being of moderate concern, and scores above the 75th percentile as being of extreme concern. The cut-off points of the general fear subscale (first four items) were not modified from the original version because these items did not undergo any change.
Results
The data were analyzed with the statistical package STATA 14 for Windows (StataCorp, 2015). A total of 200 women between 29 and 81 years old participated (mean age of 52+ 9.5 years); most of them (72 %) without a partner, practicing the Catholic religion (72.5 %), with a low socioeconomic level (71.4 %) and dedicated home (65 %). Almost half of them with a basic educational level (47.5 %), considering the national educational average of 9.1 years of study (Table 1).
An average survival time of 52 months (4.3 years) was observed, 34 % with some comorbidity, among which, the most frequent were cardiovascular and metabolic (31 %). Eighty-eight % of the participants were diagnosed in an early stage of the disease (0-IIIA), either radical or simple mastectomy, was the surgery mostly performed (66.5 %) with 74.5 % who did not undergo a process of cosmetic reconstruction of the breast. Forty-one % received a combination scheme of 2 treatments and finally 10.5 % were positive for some genetic mutation, being alteration in BRCA1 the most frequent (38 %) followed by BRCA 2 with 28.6 %. (Table 1).
On the other hand, 26.7 % reported having had some mental health problem prior to the evaluation, mainly anxiety or depression (10 % each); when evaluating this symptomatology with the HADS scale, 26.5 % of the participants reported some level of anxiety symptoms (mild, moderate or severe, according to the cut-off points of the version in Spanish for Mexico for cancer patients; Galindo Vázquez et al., 2015) and a 17.5 % of depression symptoms.
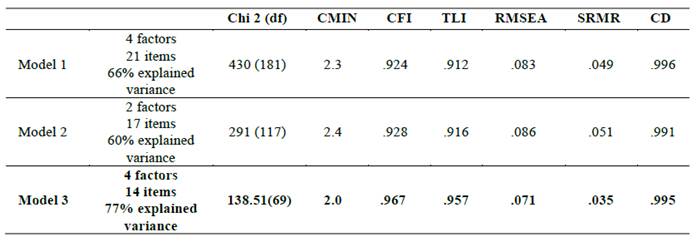
CFA for the specific concerns section resulted in 14 questions with factor loadings from .63 to .94, distributed in four factors that explained 77 % of the variance renamed “General Concerns”, “Functionality”, “Self-concept” and “Concerns for Death” (Figure 1). It is important to mention that during the process, different models were probed among which stand out a 26 items-four factor model, a bifactor model with 17 items and the final model for which the main goodness-of-fit indices were adequate: CFI = .967, TLI = .957, RMR = 0.035, RMSEA = .071, Coefficient of determination CD = .995 showing to be the best option with better fit-indices and greater parsimony (Table 2).
As it shows in the model (Figure 1), 12 questions were eliminated, due to their low factorial loads (< .40), to the fact that they scored in more than one factor, to their low discrimination capacity in the response options and/or their clinical relevance. For example, items such as “Makes me feel less feminine”, “Affects my spirituality or my faith”, “Makes me feel less of a woman”, “Damage my self-confidence” even showed low understanding on the part of the participants from the moment of piloting the instrument.
The four independent questions about general fear that was excluded from the factorial analysis showed a Cronbach's α of .923 (according to analysis carried out based on the original version). The described model obtained by the factor analysis (with 14 items distributed in 4 factors) showed a Cronbach's α general reliability index of α = .94, and by factor of α = .87 for General-Concerns, Functionality α = .91, Self-concept α = .78, Death α = .86 and the general fear subscale α = .92. This shows that CARS-M is reliable for measuring fear of breast cancer recurrence and the specific concerns derived from said fear.
Table 1: Sample characteristics
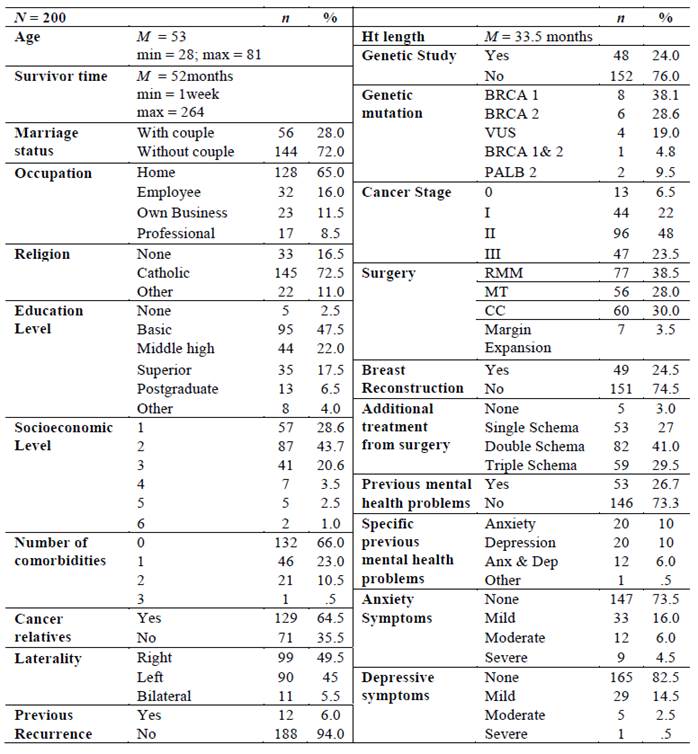
Note: Mutation n = 21. Ht: Hormone-therapy; RMM: Radical Modified Mastectomy; MT: Simple Mastectomy; CC: Conserved Surgery; VUS: Variant of uncertain meaning (Spanish acronym). Single Schema: chemotherapy, radiotherapy or hormonotherapy; Double Schema: 2 treatment combination; Triple Schema: chemo, radio & hormonotherapy. Anx: Anxiety; Dep: Depression.
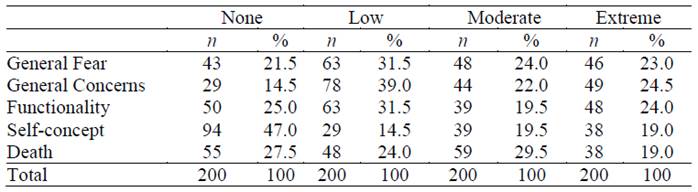
With the cut-off points stablished it is observed that 48 % reported moderate to extreme fear of recurrence with main concerns about their functionality could be affected as a result of a recurrence (53.5 % moderate extreme) or could cause death (48.5 %) (Table 3).
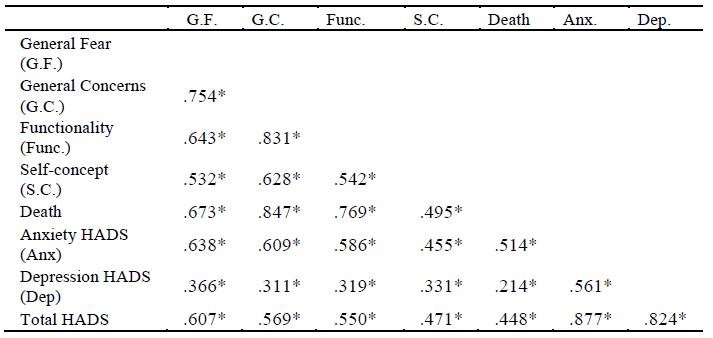
The CARS-M positively correlated with the HADS scale (r = .587; p = .01) and the HADS anxiety subscale (r = .625; p = .01). Likewise, all factors correlated positively and moderate to high with each other (r = .628-.847; p < .001) and with the general fear subscale of the CARS-M (r= .532-.754; p < .001) as shows in Table 4.
Discussion
The described results show CARS-M scale as the first valid and reliable instrument to measure this construct in Mexico and Latin America, an instrument easy to use in clinical settings and understandable for the population. However, unlike the original version and both previous validations (Japan and Dutch), Mexican version was formed by 14 items. As part of the cultural adaptation process, the factors Health, Role and Womanhood were restructured and renamed according to the characteristics of the items, remaining as General Concerns, Self-concept and Functionality. This because the terms were considered more appropriate in relation to their content and language of the population. So, these adjustments reveal socio-cultural differences between populations, for example, education level, level of literacy that could derive in the ability to understand the reagents.
The adequate fit indices show that the CARS is a valid instrument for use in the screening of cancer survivors, even virtually. When comparing the scores of fear of recurrence between the Mexican population, the United States and the Netherlands, they show similarity (55 %, 56 % and 47 % respectively) with 53 % reporting none or minimum levels comparing with 46 % and 44 %.
Nevertheless, it should be noted that practically a quarter of the participants (21.5 %) have no fear of recurrence, which should be analyzed and compared with other populations, since not having any fear could be considered poor functioning and imply a lack of self-care behaviors (Jones et al., 2016). So, according to the literature, it could be considered that the participants show a possible avoidant coping style which leads to minimizing the situation and greater negative consequences on health (Lai et al., 2020) or face a phenomenon of hopelessness (Ravindran et al., 2019).
This avoidance is one of the coping styles most reported by breast cancer survivors using strategies such as self-distraction, denial, behavioral and cognitive disconnection, alcohol and drug use, or self-blame (De Vries et al., 2014; Lashbrook et al., 2018; Mutsaers et al., 2016). It has also been observed that marital status affects resilience and avoidant coping style, concluding that the partner plays an important role in the recovery from the survivors (Lai et al., 2020; Lashbrook et al., 2018; Ravindran et al., 2019). Remembering that 72 % of the participants are single, it leads us to consider further the hypothesis that an avoidant coping style is associated with those low levels of fear of recurrence.
Conclusions
The CARS-M scale shows adequate psychometric properties for its use in the screening and evaluation process of Mexican breast cancer survivors and in clinical and virtual settings.
In general terms, Mexican breast cancer survivors has low (31 %) to moderate (24 %) levels of fear of recurrence. Scores that fall within the world reported range (39- 97 %) with 70 % showing some degree of fear, 78 % in the present study (NCCN, 2022; Simard et al., 2013; Thewes et al., 2012). And the main concern derived from a possible recurrence is that related to the risk of losing their life as was reported by Vickberg (2003), Lai et al., (2020), Lengacher et al., (2016) or Mutsaers et al., (2016).
The study has some limitations such as the use of a convenience sample, affecting the external validity as it has little representativeness capacity to generalize the results. With this, it is suggested to expand the sample by randomly selecting from different hospitals. Equally, it is suggested to simultaneously study coping styles to obtain better conclusions on the subject. Finally, the use of a structured clinical interview to determine the clinical levels of fear of recurrence more accurately as proposed by Mutsaers et al. (2016) and Simard and Savard (2015).

