










Services on Demand
Journal

Article
 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Related links
Share

 Permalink
PermalinkCiencias Psicológicas
Print version ISSN 1688-4094On-line version ISSN 1688-4221
Cienc. Psicol. vol.17 no.1 Montevideo 2023 Epub June 01, 2023
https://doi.org/10.22235/cp.v17i1.2922
Original articles
Analysis of the psychometric properties of the Self-Care Scale for Argentina

1 Universidad Católica Argentina, Instituto Universitario Hospital Italiano de Buenos Aires, Argentina, marisa@behrends.com.ar
2 Universidad Católica Argentina, Argentina
3 Universidad de Ciencias Empresariales y Sociales, Universidad Nacional del Chaco Austral, Argentina
The purpose of this paper is to report the psychometric properties and normative data of the Self-Care Scale in the Argentine population. The scale evaluates the self-care from an integral view of the construct, this includes the external aspects of the self-care, the intrapsychic self-care and the relational aspects of how human take care of themselves. The scale consists of 31 items that are answered from a Likert format that involve seven possible answers. A non-experimental, cross-sectional, instrumental-type study was designed. A non-probabilistic sample made up of 768 subjects residing in different provinces of the Argentine Republic was established. When carrying out the construct validity studies, the Exploratory Factor Analysis indicates the grouping of the items into six factors. With the Confirmatory Factor Analysis, it was observed that the six-factor model presented a good fit. The results show an adequate internal consistency of the test and an adequate test-retest stability after five weeks. The results obtained in the research carried out are consistent with the findings of the original study, which indicates that the studies of the psychometric properties of the scale are reliable and valid to be used in the general Argentine population.
Keywords: psychometric properties; Self-Care Scale; reliability; validity
El propósito del presente artículo es informar las propiedades psicométricas y los datos normativos de la Escala de Autocuidado en población argentina. Dicha escala mide el autocuidado desde una conceptualización amplia e integral que incluye los aspectos materiales externos del autocuidado, el autocuidado intrapsíquico y los aspectos relacionales de cómo los humanos se cuidan a sí mismos. La escala está compuesta por 31 ítems que se responden con un formato tipo Likert de siete opciones de respuesta. Se diseñó un estudio no experimental, transversal, de tipo instrumental. Se estableció una muestra no probabilística conformada por 768 participantes de la República Argentina. Al realizar los estudios de validez de constructo se efectuó el Análisis Factorial Exploratorio observándose la agrupación de los ítems en seis factores. Con el Análisis Factorial Confirmatorio se observó que el modelo de seis factores presentó un buen ajuste. Los resultados muestran una adecuada consistencia interna del test y una adecuada estabilidad test-retest luego de cinco semanas. En su conjunto, los resultados obtenidos en la investigación realizada son concordantes con los hallazgos del estudio original lo que indica que las propiedades psicométricas de la escala son confiables y válidos para ser utilizados en población general argentina.
Palabras clave: propiedades psicométricas; Escala de Autocuidado; fiabilidad; validez
O objetivo deste artigo é informar as propriedades psicométricas e os dados normativos da Escala de Autocuidado na população argentina. Dita escala mede o autocuidado a partir de uma conceituação ampla e integral, que inclui os aspectos materiais externos do autocuidado, o autocuidado intrapsíquico e os aspectos relacionais de como os seres humanos cuidam de si. A escala está composta por 31 itens que são respondidos em um formato do tipo Likert com sete opções de resposta. Foi desenhado um estudo não experimental, transversal, do tipo instrumental. Foi estabelecida uma amostra não probabilística composta por 768 sujeitos da República Argentina. Ao realizar os estudos de validade de construto, foi efetuada a Análise Fatorial Exploratória, observando-se o agrupamento dos itens em seis fatores. Com a Análise Fatorial Confirmatória, observou-se que o modelo de seis fatores apresentou um bom ajuste. Os resultados demostram uma adequada consistência interna do teste e uma adequada estabilidade teste-reteste após cinco semanas. Como um todo, os resultados obtidos na pesquisa realizada são consistentes com os achados do estudo original, o que indica que as propriedades psicométricas da escala são confiáveis e válidas para uso na população geral argentina.
Palavras-chave: propriedades psicométricas; Escala de Autocuidado; confiabilidade; validade
In recent years, an established topic that has gained space in different fields is that of self-care. Improvements in the living conditions, the development in health care and medical attention have produced a change in the lifestyle of the population, generating an increase in life expectancy. This change places each individual in a key role in their own health care. Hence the importance of people carrying out effective self-care behaviors (Nuno-Solinis et al., 2013). Rivera Álvarez (2006) points out the social impact of individual self-care actions, recognizing its value as a duty and right for oneself and for the community, with its consequent impact on the health system.
Self-care favors the maintenance of good personal health, reducing the impact of future conditions and, therefore, their need for treatment in the Public Health System. Having an instrument capable of measuring and operationalizing the self-care construct serves as a tool that makes it easier for health professionals to assess the level of self-care of individuals in order to provide effective and beneficial assistance. Education by health professionals is ultimately successful when self-care behaviors are carried out by people without the supervision, support and daily follow-up of the professional, that is, these self-care behaviors can be carried out autonomously by individuals (Olivella-Fernández et al., 2012). In turn, this intervention is useful in the short and long term, since self-care habits in the young population guarantee the quality of life of the elderly (Loredo-Figueroa et al., 2016). The importance of carrying out effective self-care behaviors for health not only has implications for managing to control or recover from diseases, but also has an impact when it comes to preventing diseases and health conditions and, in turn, promoting well-being. (Schneider Hermel et al., 2015).
Although it is a concept that has received different conceptualizations, depending on the theoretical tradition, in a very broad sense, self-care could be defined as the commitment to practices that promote well-being (González-Vázquez et al., 2018). According to Naranjo et al. (2017) “self-care is a regulatory human function that each individual must apply deliberately in order to maintain their life and their state of health, development and well-being” (p. 2).
A pioneer in the study of this concept was Dorothea Orem, who proposed the Self-Care Deficit Theory, composed of the self-care deficit theory, the self-care theory, and the nursing systems theory (Naranjo et al., 2017). This author refers to self-care agency as the ability of people to take care of themselves by performing specific actions for this purpose (Orem, 2001).
On the other hand, Riegel et al. (2012, 2021) develop the Mid-Range Theory of Chronic Disease Self-Care, where self-care is defined as a health maintenance process through health promotion and disease management practices, including prevention, treatment and rehabilitation. This theoretical model specifies three concepts: (a) self-care maintenance, with behaviors that tend to preserve health, (b) self-care follow-up, such as routine tests, and (c) self-care management, such as changes in the diet. As Riegel et al. (2019) point out, self-care is carried out throughout the health-disease process. Although when a person suffers from a disease, the need for self-care is clearly seen, it is essential in states of health precisely for the prevention of any condition. However, any condition makes it clear whether self-care patterns are adaptive or not.
Self-care practice refers to engaging in behaviors that maintain and promote physical, emotional, mental, and social well-being. This practice can include behaviors such as resting the number of hours necessary for each person, adequate and healthy eating, sleep behaviors, physical exercise, brushing teeth, maintaining a social support network, developing emotional regulation skills, practicing meditation, personal therapy, religious or faith practices that each one professes, among others (Myers et al., 2012; Riegel et al., 2012).
Nuno-Solinis et al. (2013) from a behavioral perspective, define it as the set of tasks that an individual carries out to preserve both physical and emotional health, and guarantee the proper management of chronic diseases. Self-care can be learned as an attitude that allows the development of healthy behaviors to promote well-being (Naranjo et al., 2017). González-Vázquez et al. (2018) state that emotional and cognitive factors, which are often left aside in the approach, play a key role when it comes to understanding the phenomenon. According to these authors, behavioral conceptualizations, directed at the outside world, leave aside psychological aspects, which must be addressed in greater depth.
From childhood, people internalize the early care experiences they receive from the adults in charge. Those who grow up in environments with varying degrees of neglect, or even abusive or negligent environments, would not develop healthy patterns of self-care because these practices were not learned from childhood and the way they were treated shapes the way they later, as adults, experience self-care (González et al., 2009; Mosquera & González, 2011; Ryle & Kerr, 2020).
González-Vázquez et al. (2018) developed a more comprehensive conceptualization of the construct that includes three dimensions: (a) the external material aspects of self-care, (b) intrapsychic self-care, and (c) the relational aspects of how humans care for themselves through interactions with others (González & Mosquera, 2015; González-Vázquez et al., 2018).
In relation to the measurement of the construct, there are different tools, such as the Diabetes Self-Care Inventory by Ausili et al. (2017), or the High Blood Pressure Self-Care Inventory version 3.0 by Dickson et al. (2021) based on the Mid-Range Theory of Chronic Illness Self-Care, or the Self-Care Agency Rating Scale (ASA) developed by Evers in 1989 that measures self-care agency, a central concept in Self-Care Deficit Theory.
However, based on the more comprehensive conceptualization carried out by González-Vázquez et al. (2018), the authors saw the need to create a scale that measures this construct from a broader and deeper perspective that includes the three dimensions they propose. The material dimension implies the ability to look for good things, seek positive experiences and try to satisfy one's own needs. The internal dimension implies the intrapsychic capacity to look at oneself positively and, at the same time, realistically. Finally, the interpersonal dimension is related to the search for positive interactions with others to satisfy one's interpersonal needs for support and self-care. From this perspective, self-care is then defined as “the conduct directed by the individual to preserve and improve health and well-being; it is a pattern of relationship with the person, with the world and with another” (González-Vázquez et al., 2018, p. 374).
These three dimensions are the foundations of the self-care scale created by González-Vázquez et al. (2018), which has 31 items that the person responds to with a Likert-type scale. The final version of the Self-Care Scale was applied to a sample of 273 psychiatric outpatients in La Coruña, Spain (González-Vázquez et al., 2018).
As described in preceding paragraphs, the term self-care has been used for several decades, mainly in the area of medicine, with different conceptualizations depending on the tradition that defines it. On the other hand, researchers from different countries are developing more and more interventions about self-care to improve health both individually and in the community, due to its value in clinical medicine and psychology, but also in public health (Oltra, 2013; Riegel et al., 2021).
Given the importance of self-care in promoting health and preventing disease in the entire population, it is relevant to have an evaluation tool that studies it from a broad but deep theoretical perspective, in the Argentine population. Although, as has been seen, there are various measurement tools, in the present work we have chosen to study the Self-Care Scale of González-Vázquez et al. (2018) whose theoretical model contemplates the external, intrapsychic and relational dimensions of self-care.
The general objective of this work is to study, in a preliminary way, the psychometric properties of the Self-Care Scale by González-Vázquez et al. (2018) in Argentine population. The specific objectives are: (a) to preliminarily analyze the factorial structure of the scale and the dimensionality of the construct, (b) to preliminarily analyze the internal consistency and temporal stability of the Self-Care Scale in the general population.
Method
Sample
A sample of 768 adults was formed, thus having an estimation sample (n = 423) to perform the exploratory factor analysis (EFA) and a validation sample (n = 345) for the confirmatory factor analysis (CFA). The participants were volunteers and did not receive any compensation for their collaboration. Of the 423 participants belonging to the estimation sample, 52.6 % were women and 47.4 % were men. The average age was 35.18 (SD = 1.24, Min = 18, Max = 81). Regarding marital status, 43.2 % said they were married or living with their partner, 47.2 % reported being single, 8.6 % divorced, and 1 % widowed. The remaining 345 participants in the validation sample had an average age of 34.12 (SD = 1.13, Min = 18, Max = 76). Regarding their place of residence, 15.2 % reported living in the north of the country, 81.9 % in the central region, and the remaining 2.9 % reported living in the south. Regarding marital status, 41.2 % said they were married or living with their partner, 45.2 % reported being single and 13.6 % divorced.
Instruments
Sociodemographic survey. Through this instrument, data were obtained on sex, age, the date on which the questionnaire was completed, place of residence, marital status, educational level attained, activity or profession.
Self-Care Scale (González-Vázquez et al., 2018). It has 31 items. The items are statements to which the subject will respond using a Likert-type scale with seven response options: totally disagree, quite disagree, somewhat disagree, neither agree nor disagree, somewhat agree, quite agree, and totally agree. The scale is made up of six subdimensions: (a) Self-destructive behavior with α = .90; (b) Lack of tolerance of shared positive affect with α = .75; (c) Difficulty in accepting and asking for help with α = .75; (d) Resentment over not receiving reciprocity with α = .77; (e) Absence of positive activities with α = .67; (f) Not taking into account one’s own needs with α = .76. The full scale gave an α = .91
Design
A non-experimental, cross-sectional, instrumental study was designed (Ato et al., 2013). Regarding the sampling method, it was a non-probability convenience sample.
Procedure
The participants were informed of the purposes of the research, the confidentiality of the data and their right to refuse to participate and withdraw from the research whenever they consider it necessary. The instruments used to measure the variables were distributed through social networks through Google Forms. The form presented an informed consent, which was in the first part of the distributed survey, before the inventory items began and without the possibility of continuing to answer it without first checking the terms and conditions checkbox. After five weeks, a new survey administration was carried out with the same modality to a third of the subjects of the sample.
Data analysis
First, the univariate normality of the data was examined through the indicators of skewness and kurtosis, for which values between +/- 2 are desirable (Tabachnick & Fidell, 2013). For the identification of univariate atypical cases, the Z-scores were examined, considering as extreme values those that exceeded Z = +/- 3.29. For the detection of multivariate atypical cases, the Mahalanobis distance was obtained as a criterion with p values less than .001 (Tabachnick & Fidell, 2013). Then, studies were carried out to verify the internal structure of the scale through EFA and CFA. It is known that some authors criticize the joint use of these analyses (Pérez-Gil et al., 2000). However, numerous works choose to implement both, justifying the use of two procedures (Martorell et al., 2011; Pechorro et al., 2017; Perugini & Castro Solano, 2018). The EFA was calculated through the MLR method using an Oblimin rotation using an asymptotic matrix of correlations, just like the original scale. The CFA was performed using a robust estimator of weighted least squares means and variance adjusted (WLSMV-R), and since the variables were ordinal, the same matrix was obtained as in the EFA, since it is more appropriate for this type of data (Freiberg Hoffmann et al., 2013). According to Hu et al. (1992) the following goodness-of-fit indices were considered: Chi-square (χ2), comparative fit index (CFI), Bollen’s incremental fit index (IFI; Bollen & Long, 1993), and root mean square error of approximation (RMSEA). Regarding the criteria of acceptable fit values, a value of .90 is considered in CFI (Kline, 2018; Stegmann, 2017), as well as values less than or equal to .08 in RMSEA (Browne & Cudeck, 1993). The evidence based on the internal structure was evaluated through the examination of the factorial loads, standardized loads greater than the limit of > .30 were considered acceptable (Hair et al., 2006; Nunnally & Bernstein, 1994), and, in terms of the correlations between factors, values > .19 are considered very low, between > .20 and < .39 as low, between > .40 and < .59 as moderate, between > .60 and < .79 as high, and < .80 as very high (Brown, 2006; Evans, 1996). To know the reliability of the scale from the point of view of its internal consistency, the ordinal alpha statistic was used, which is recommended for multidimensional scales with few items (Bryant & Satorra, 2012; Dominguez-Lara, 2012; Espinoza & Novoa-Muñoz, 2018) and that offers an approximation of reliability based on the factorial structure. In addition, to analyze the temporal stability of the items on the scale, the test-retest statistical test was administered to 268 people at two intervals of five weeks. The results were processed using R (Version 3.6.0) and the R Studio interface (Version 1.4.1717) using the ggplot2 packages for data visualization (Villanueva & Chen, 2019), psycho (Revelle, 2018) and psychometric (Fletcher & Fletcher, 2013), to estimate some psychometric properties. While lavaan (Rosseel et al., 2017), semPlot (Epskamp et al., 2019) and semTools (Jorgensen et al., 2018) were used to calculate and plot the Structural Equation Model. For the realization of the normative scores, the statistical program SPSS in its version 25 was extracted.
Results
Descriptive analysis
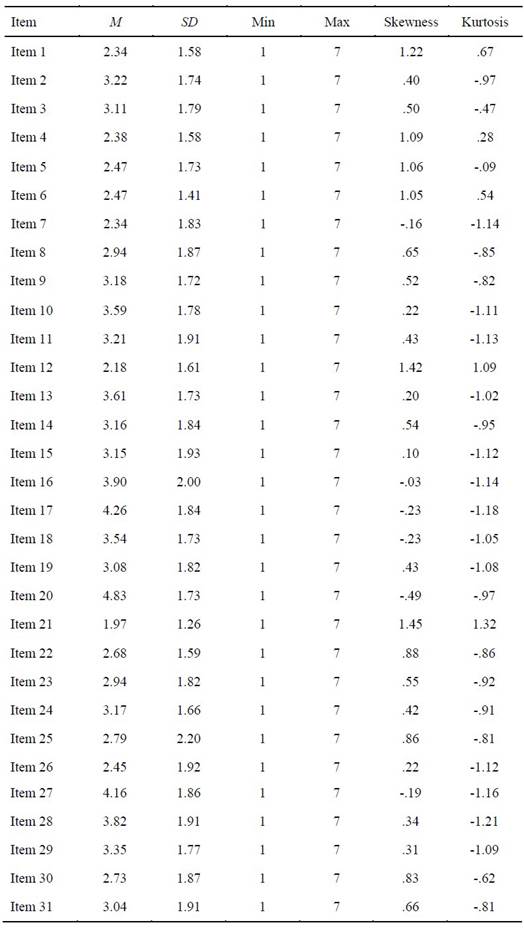
A preliminary analysis of the scale items was performed with the intention of obtaining univariate normality. As can be seen in Table 1, basic descriptive statistics were obtained by calculating means and standard deviations. In addition, the skewness and kurtosis indices were calculated. The values recommended by Tabachnick and Fidell (2013) are close to 0 and lower than 1.96.
Construct validity
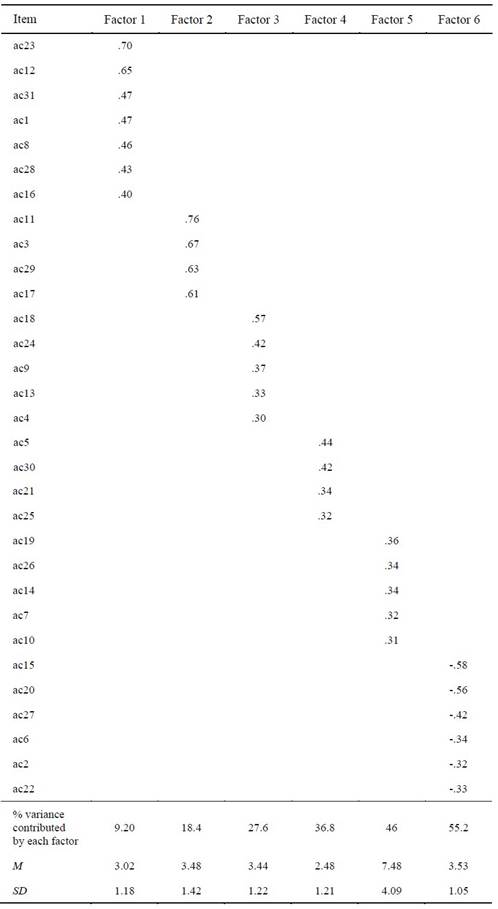
The sample was divided into two parts, an estimation sample (n = 423) to perform the EFA and a validation sample (n = 345) for the CFA. Table 2 shows the EFA, the robust method of maximum likelihood was used and from the Varimax rotation, it determined the grouping of 31 items in six latent variables. The factorial solution yielded values considered adequate equal to .87 for the Kaiser Meyer Olkin index (KMO) and for the Barlett Sphericity Test (χ²= 231.97; SD = 0.30; p < .000). The exploratory factor analysis explained 55.2 % of the variance of the scores.
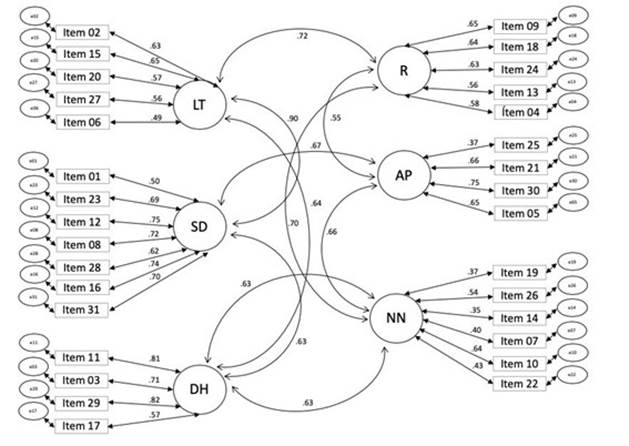
Next, the CFA of the Self-Care Scale was performed. The Robust Maximum Likelihood estimation method was used and, since the variables were ordinal, the polychoric matrix was used. When assessing the goodness of fit of the model, different indices were examined: Chi-square (χ2), comparative fit index (CFI), Bollen's incremental fit index (IFI) and root mean square error of approximation (RMSEA). All indicated that the six-factor model presented a good fit: χ2 = 1436.218, p <.000; IFC = .964; IFI = .969; RMSEA = .062 90% CI (.058, .062), p < .001. In addition, Figure 1 shows the regression weights for each item that were between moderate (> .40 and < .59), high (> .60 and < .79) and very high (< .80; Brown, 2006; Evans, 1996).
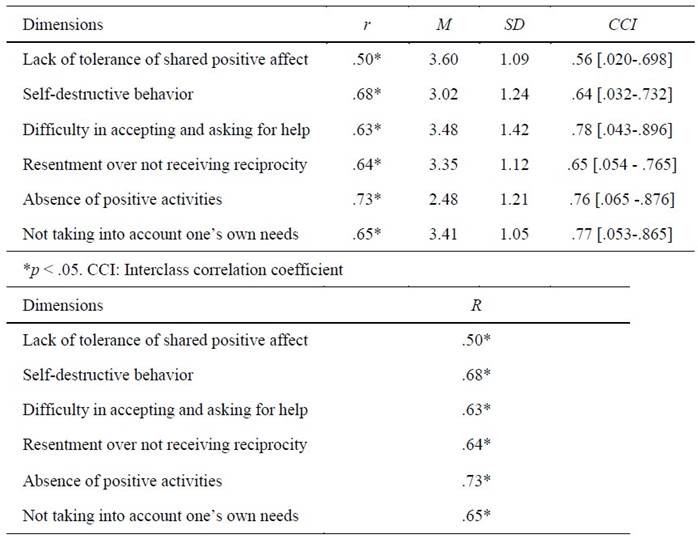
Regarding the internal consistency of the scale, the following ordinal alpha indexes were obtained for the subdimensions: Lack of tolerance of shared positive affect = .82; Self-destructive Behavior = .79; Difficulty in accepting and asking for help = .80; Resentment over not receiving reciprocity = .83; Absence of positive activities = .78 and Not taking into account one’s own needs = .80. Finally, in Table 3, the test-retest correlations can be observed in a period of time of five weeks. The results reported that the correlations between the dimensions were positive and significant between moderate and high.
Normative data
Table 4 grouped the mean scores and the levels that indicate the presence of each dimension of the Self-Care Scale in participants from the general population. In turn, the percentiles of each dimension were defined. To obtain the percentile values, the raw scores obtained in each dimension must be added and divided by the number of items. A T score greater than 50 indicates the presence of the dimension that makes up the self-care construct.
Table 4: Normative Data of the Self-Care Scale (n = 768)
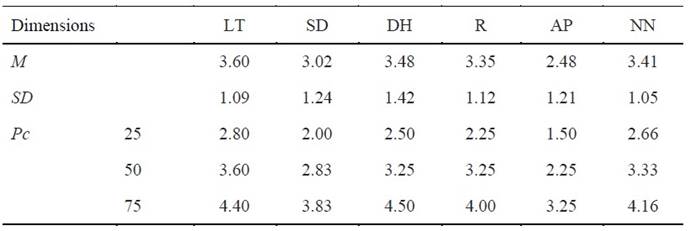
Note: Pc: Percentile; LT: Lack of tolerance of shared positive affect; SD: Self-destructive behavior; DH: Difficulty in accepting and asking for help; R: Resentment over not receiving reciprocity; AP: Absence of positive activities; NN: Not taking into account one’s own needs.
Discussion
This study reports the results of the analysis of the psychometric properties of the Self-Care Scale, reporting the validity based on the internal structure, the reliability by consistency and temporal stability of the score (González-Vázquez et al., 2018) in the Argentine general population. The importance of adapting this scale to our environment is based on the need to have a tool that measures this construct due to its relevance to people's health in general and the impact it has on the Health System in particular.
Self-care can be considered a complement to the actions carried out by the health services for the care of a population, as a shared responsibility (Rivera Alvarez, 2006), both individually and collectively, giving the Health System a relevant role in the monitoring of the matter. The importance of having a valid and reliable instrument for its evaluation in the local population stands on these pillars, which would be very useful for health professionals. As the bibliography points out, self-care can be learned as an attitude that allows the development of healthy behaviors, which is why it is important to consider the emotional and cognitive aspects, since they play a key role in understanding the phenomenon and favoring its development (González-Vázquez et al., 2018; Riegel et al., 2012).
When carrying out the construct validity studies, the EFA was carried out, observing the grouping of 31 items into six factors, which is in agreement with the original study (González-Vázquez et al., 2018). The factorial solution yielded values considered adequate. The EFA explained 55.2 % of the accumulated variance, similar to the reference study in which this value is 55.3 %. From CFA it was observed that the six-factor model presented a good fit.
In relation to the internal consistency of the subdimensions, unlike the original scale, it was decided to use the alpha ordinal statistic because it is more appropriate for the type of matrix that the inventory presents, which is why it could not be compared with the Cronbach's alpha statistic of the original scale. However, it can be inferred that the internal consistency values in the dimensions of both scales are similar. Finally, in relation to the test-retest correlations in a period of five weeks, the results reported that the correlations between the dimensions were positive and significant between moderate and high, which indicates the stability of the measures obtained as well as the data obtained by the interclass correlation coefficient.
Finally, some limitations should be noted. The first is that it was not possible to form a sample of similar proportions with respect to the sex variable, in which two out of three people in the sample are women. The second limitation is that the sample to which the Self-Care Scale was administered is not representative of the entire Argentine population, since it is made up mostly of inhabitants of the Autonomous City of Buenos Aires and Greater Buenos Aires. For this reason, it is advisable in the future to consider that the study be replicated in an expanded sample that includes the rest of the Argentine provinces. In conclusion, as a whole, the results obtained in this work are in agreement with the original study carried out by González-Vázquez et al. (2018). This indicates that the studies of the psychometric properties of the scale are reliable and valid to be used in the Argentine general population.
REFERENCES
Ato, M., López, J. J., & Benavente, A. (2013). Un sistema de clasificación de los diseños de investigación en psicología. Anales de Psicología, 29(3), 1038-1059. https://doi.org/10.6018/analesps.29.3.178511 [ Links ]
Ausili, D., Barbaranelli, C., Rossi, E., Rebora, P., Fabrizi, D., Coghi, C., Luciani, M., Vellone, E., Di Mauro, S., & Riegel, B. (2017). Development and psychometric testing of a theory-based tool to measure self-care in diabetes patients: the self-care of diabetes inventory. Trastornos Endócrinos de BMC, 17(1), 1-12. https://doi.org/10.1186/s12902-017-0218-y [ Links ]
Bollen, K. & Long, J. (1993). Testing structural equation models. Sage. [ Links ]
Brown, T. A. (2006). Confirmatory factor analysis for applied research. Guilford Publications. [ Links ]
Browne, M. W. & Cudeck, R. (1993). Alternative ways of assessing model fit. In K. A. Bollen & J. S. Long (Eds.), Testing structural equation models (pp. 136-162). Sage. [ Links ]
Bryant, F. B. & Satorra, A. (2012). Principles and practice of scaled difference Chi-Square testing. Structural Equation Modeling: A Multidisciplinary Journal, (19), 372-398. https://doi.org/10.1080/10705511.2012.687671 [ Links ]
Dickson, V. V., Fletcher, J., & Riegel, B. (2021). Psychometric testing of the Self-care of Hypertension Inventory version 3.0. Journal of Cardiovascular Nursing, 36(5), 411-419. https://doi.org/10.1097/JCN.0000000000000827 [ Links ]
Dominguez-Lara, S. (2012). Propuesta para el cálculo del Alfa Ordinal y Theta de Armor. Revista de Investigación en Psicología, 15(1), 213-217. [ Links ]
Epskamp, S., Stuber, S., Nak, J., Veenman, M., & Jorgensen, T. D. (2019). semPlot: Path Diagrams and Visual Analysis of Various SEM Packages’ Output (Version 1.1. 2) (Computer software). https://cran.r-project.org/web/packages/semPlot/semPlot.pdf [ Links ]
Espinoza, S. C. & Novoa-Muñoz, F. (2018). Ventajas del alfa ordinal respecto al alfa de Cronbach ilustradas con la encuesta AUDIT-OMS. Revista Panamericana de Salud Pública, (42), e65. https://doi.org/10.26633/RPSP.2018.65 [ Links ]
Evans, J. D. (1996). Straightforward statistics for the behavioral sciences. Brooks/Cole Publishing. [ Links ]
Fletcher, T. D. & Fletcher, M. T. D. (2013). Package psychometric. http://cran. rproject. org/web/packages/psychometric/psychometric. pdf Vol 4. [ Links ]
Freiberg Hoffmann, A., Stover, J. B., de la Iglesia, G., & Fernández Liporace, M. (2013). Correlaciones Policóricas y Tetracóricas en Estudios Exploratorios y Confirmatorios. Ciencias Psicológicas, 7(2), 151-164. https://doi.org/10.22235/cp.v7i1.1057 [ Links ]
González, A., Seijo, N., & Mosquera, D. (2009, August 27-29). EMDR in complex trauma and dissociative disorders (Paper presentation). 14th EMDR International Association Annual Conference, Atlanta, GA, United States . [ Links ]
González, A. & Mosquera, D. (2015). EMDR y disociación. El abordaje progresivo (2nd ed.). Ediciones Pléyades. [ Links ]
González-Vázquez, A. I., Mosquera-Barral, D., Knipe, J., Leeds, A. M., & Santed-German, M. A. (2018). Construction and initial validation of a scale to evaluate self-care patterns: The Self-Care Scale. Clinical Neuropsychiatry, 5(6), 373-378. [ Links ]
Hair, J. F., Black, W. C., Babin, B. J., Anderson, R. E., & Tatham, R. L. (2006). Multivariate Data Analysis. Pearson Prentice Hall. [ Links ]
Hu, L. T., Bentler, P. M., & Kano, Y. (1992). Can test statistics in covariance structure analysis be trusted? Psychological Bulletin, 112(2), 351. https://psycnet.apa.org/doi/10.1037/0033-2909.112.2.351 [ Links ]
Jorgensen, T. D., Pornprasertmanit, S., Schoemann, A. M., Rosseel, Y., Miller, P., Quick, C., & Garnier-Villarreal, M. (2018). semTools: Useful tools for structural equation modeling. R package version 0.5-1 (Computer software). https://cran.r-project.org/web/packages/semTools/semTools.pdf [ Links ]
Kline, R. B. (2018). Response to leslie hayduk’s review of principles and practice of structural equation modeling. Canadian Studies in Population, 45(3-4), 188-195. https://doi.org/10.25336/csp29418 [ Links ]
Loredo-Figueroa, M. T., Gallegos-Torres, R. M., Xeque-Morales, A. S., Palomé-Vega, G., & Juárez-Lira, A. (2016). Nivel de dependencia, autocuidado y calidad de vida del adulto mayor. Enfermería Universitaria, 13(3), 159-165. https://doi.org/10.1016/j.reu.2016.05.002 [ Links ]
Martorell, M. C., González, R., Odoñez, A., & Gómez, O. (2011). Estudio confirmatorio del cuestionario de conducta antisocial (CCA) y su relación con variables de personalidad y conducta antisocial. Revista Iberoamericana de Diagnóstico y Evaluación - e Avaliação Psicológica, 31(2), 35-52. [ Links ]
Mosquera, D. & González, A. (2011). Del apego temprano al TLP. Mente y cerebro, (46), 18-27. [ Links ]
Myers, S. B., Sweeney, A. C., Popick, V., Wesley, K., Bordfeld, A., & Fingerhut, R. (2012). Self-care practices and perceived stress levels among psychology graduate students. Training and Education in Professional Psychology, 6(1), 55-66. https://doi.org/10.1037/a0026534 [ Links ]
Naranjo, Y., Concepción, J., & Rodríguez, M. (2017). La teoría déficit de autocuidado: Dorothea Elizabeth Orem. Revista Gaceta Médica Espirituana, 19(3). https://revgmespirituana.sld.cu/index.php/gme/article/view/1129 [ Links ]
Nunnally, J. C. & Bernstein, I. H. (1994). Psychometric theory (3rd ed.). McGraw Hill. [ Links ]
Nuno-Solinis, R., Rodríguez-Pereira, C., Pinera-Elorriaga, K., Zaballa-González, I., & Bikandi-Irazabal, J. (2013). Panorama de las iniciativas de educación para el autocuidado en España. Gaceta Sanit, 27(4), 332-337. https://doi.org/10.1016/j.gaceta.2013.01.008 [ Links ]
Olivella-Fernández, M. C., Bastidas-Sánchez, C. V., & Castiblanco-Amaya, M. A. (2012). La adherencia al autocuidado en personas con enfermedad cardiovascular: abordaje desde el Modelo de Orem. Aquichan, 12(1), 53-61. [ Links ]
Oltra, S. (2013). El autocuidado, una responsabilidad ética. Gaceta de Psiquiatría Universitaria, 9(1), 85-90. [ Links ]
Orem, D. E. (2001). Nursing: Concepts of practice. Mosby. [ Links ]
Pechorro, P., Kahn, R. E., Ray, J. V., Raine, A., & Gonçalves, R. A. (2017). Psychometric properties of the Reactive-Proactive Aggression Questionnaire among a sample of detained and community girls. Criminal Justice and Behavior, 44(4), 531-550. https://doi.org/10.1177/0093854816686395 [ Links ]
Pérez-Gil, J. A., Moscoso, S. C., & Rodríguez, R. M. (2000). Validez de constructo: el uso de análisis factorial exploratorio-confirmatorio para obtener evidencias de validez. Psicothema, 12(Suplemento), 442-446. [ Links ]
Perugini, M. L. L. & Castro Solano, A. (2018). Influencia de virtudes organizacionales sobre satisfacción, compromiso y performance laboral en organizaciones argentinas. Interdisciplinaria, 35(1), 171-188. https://doi.org/10.16888/interd.2018.35.1.9 [ Links ]
Revelle, W. (2018). Psych: Procedures for personality and psychological research (Version 1.9. 12.31) (Computer software). Northwestern University. [ Links ]
Riegel, B., Dunbar, S. B., Fitzsimons, D., Freedland, K. E., Lee, C. S., Middleton, S., Stromberg, A., Vellone, E., Webber, D. E., & Jaarsma, T. (2021). Self-care research: Where are we now? Where are we going? International Journal of Nursing Studies, (116), 103402. https://doi.org/10.1016/j.ijnurstu.2019.103402 [ Links ]
Riegel, B., Jaarsma, T., & Strömberg, A. (2012). A middle-range theory of self-care of chronic illness. Advances in Nursing Science, 35(3), 194-204. https://doi.org/10.1097/ANS.0b013e318261b1ba [ Links ]
Riegel, B., Jaarsma, T., Lee, C. S., & Strömberg, A. (2019). Integrating symptoms into the middle-range theory of self-care of chronic illness. ANS. Advances in Nursing Science, 42(3), 206-215. https://doi.org/10.1097/ANS.0000000000000237 [ Links ]
Rivera Álvarez, L. N. (2006). Capacidad de agencia de autocuidado en personas con hipertensión arterial hospitalizadas en una clínica de Bogotá, Colombia. Revista de Salud Pública, 8(3), 235-247. https://doi.org/10.1590/s0124-00642006000300009 [ Links ]
Rosseel, Y., Oberski, D., Byrnes, J., Vanbrabant, L., Savalei, V., Merkle, E., & Rosseel, M. Y. (2017). Package lavaan. http://lavaan.org [ Links ]
Ryle, A. & Kerr, I. B. (2020). Introducing cognitive analytic therapy: principles and practice of a relational approach to mental health. John Wiley & Sons. [ Links ]
Schneider Hermel, J., Pizzinato, A., & Calderón Uribe, M. (2015). Mujeres con cáncer de mama: apoyo social y autocuidado percibido. Revista de Psicología, 33(2), 439-467. https://doi.org/10.18800/psico.201502.008 [ Links ]
Stegmann, G. (2017). Review of A Beginner’s Guide to Structural Equation Modeling, by Randall E. Schumacker y Richard G. Lomax. Structural Equation Modeling: A Multidisciplinary Journal, 24(3), 475-477. https://doi.prg/10.1080/10705511.2017.1280798 [ Links ]
Tabachnick, B. & Fidell, L. S (2013). Using Multivariate Statistics (6th ed.). Pearson. [ Links ]
Villanueva, R. A. M. & Chen, Z. J. (2019). ggplot2: Elegant graphics for data analysis (2ª ed.). Springer. [ Links ]
How to cite: Rodriguez de Behrends, M., Trovero, A., Eidman, L. (2023). Analysis of the psychometric properties of the Self-Care Scale for Argentina. Ciencias Psicológicas, 17(1), e-2922. https://doi.org/10.22235/cp.v17i1.2922
Authors’ participation: a) Conception and design of the work; b) Data acquisition; c) Analysis and interpretation of data; d) Writing of the manuscript; e) Critical review of the manuscript. M. R. d. B. has contributed in a, b, c, d, e; L. E. in b, c, e; A. T. in b, d.
Received: June 06, 2022; Accepted: December 15, 2022
 Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
