










Servicios Personalizados
Revista

Articulo
 texto en
texto en  Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
Links relacionados
Compartir

 Permalink
PermalinkCiencias Psicológicas
versión impresa ISSN 1688-4094versión On-line ISSN 1688-4221
Cienc. Psicol. vol.16 no.2 Montevideo dic. 2022 Epub 01-Dic-2022
https://doi.org/10.22235/cp.v16i2.2241
Original Articles
Influence of mindfulness levels on emotional regulation, depression, anxiety and stress dimensions in a Brief Intervention Program in candidates for the OAB exam

1 Universidade do Vale do Rio dos Sinos, Brasil
2 Universidade do Vale do Rio dos Sinos, Brasil, manu-beneton@outlook.com
3 Universidade do Vale do Rio dos Sinos, Brasil
In this study, a six-meeting mindfulness intervention was conducted with Brazilian Bar Association (OAB) exam applicants, with 42 participants. This is a quantitative, correlational and explanatory research. Linear regression showed explanatory power between the awareness dimension and the consciousness and clarity dimensions of emotional regulation in the pre and post-intervention. In the pre-test, the acceptance dimension correlates with Strategies, Non-acceptance and Impulse; in the post-test, Acceptance extends its explanatory power to all dimensions of emotional regulation. This study also points to a significant increase between the explanatory power of acceptance and the grand total of the emotional regulation scale. The correlation with depression, anxiety and stress was also up to acceptance, highlighting the increase in explanatory power regarding stress, in the post-test.
Keywords: mindfulness; depression; anxiety; stress
Neste estudo foi realizada uma intervenção de seis encontros com candidatos ao exame da Ordem dos Advogados do Brasil (OAB) com 42 participantes. Essa pesquisa é quantitativa, correlacional e explicativa. A regressão linear apresentou poder de explicação entre as dimensões awareness com as dimensões consciência e clareza da regulação emocional no pré e pós intervenção. Já a dimensão aceitação se correlaciona com estratégias, não aceitação e impulso no pré teste, sendo que no pós a aceitação apresenta poder de explicação em todas as dimensão de regulação emocional. Também se aponta para um crescimento significativo entre o poder de explicação da aceitação e o total geral da escala de regulação emocional. A correlação com a depressão, ansiedade e o estresse também ficou à cargo da aceitação, destacando o acréscimo do poder de explicação no pós teste sobre o estresse.
Palavras-chave: mindfulness; depressão; ansiedade; estresse
En este estudio se realizó una intervención de seis reuniones con candidatos para el examen del Colegio de Abogados de Brasil (OAB) con 42 participantes. Esta investigación es cuantitativa, correlacional y explicativa. La regresión lineal mostró poder de explicación entre las dimensiones conciencia con las dimensiones conciencia y claridad de regulación emocional en el pre y post intervención. La dimensión de aceptación se correlaciona con estrategias, no aceptación e impulso en el pre-test, y en el post-aceptación tiene poder de explicación en todas las dimensiones de la regulación emocional. También apunta a un crecimiento significativo entre el poder de explicación de la aceptación y el total general de la escala de regulación emocional. La correlación con depresión, ansiedad y estrés también estuvo a cargo de la aceptación, destacando el aumento del poder de explicación en el post de estrés.
Palabras clave: mindfulness; depresión; ansiedad; estrés
Mindfulness (Mfs) can be understood as the awareness that emerges when one directs attention to the present time without criticism or judgment. In addition to this, Mfs relates to the capacity in training self-regulation and attention control, which assist in promoting more assertive behaviors, minimizing thought distortions. These distortions can result in automatic and reactive emotional responses, as well as behavioral responses, associated with suffering (Kabat-Zinn, 2003). The practice of Mfs develops a greater connection between mind and body, and refines the ability to recognize the experience as a whole, seeking a friendly and compassionate attitude (Tang et al., 2012). The promotion of a Mfs posture is fundamentally achieved via meditative practices, with its core in Buddhist practices (Silva, 2019).
Operationally, Mfs is based on two important components: Awareness and Acceptance. The concept of Awareness, in this context, is understood as the monitoring of internal and external events, contemplating the scope of experience in its wholeness, without privileging particular aspects. In its turn, Acceptance concerns how one behaves regarding the present moment. It is the experience lived free of defenses, beliefs, or judgments (Silveira et al., 2012). Mfs practices recognize that emotions should not be controlled or suppressed, but tolerated and experienced (Leahy et al., 2013).
Research involving Mfs has emphasized the role of these practices in both clinical and non-clinical groups, connecting itself with emotional regulation (ER), presenting positive impacts on participants' health and life quality (Pires et al., 2018). Groups of practitioners have demonstrated a decrease in negative mood states, as well as a decrease in ruminative and distracting thoughts, and behaviors. Additionally, a reduction in emotional reactivity is verified, also affecting physiological aspects of emotions, highlighting the positive influence of Mfs on these (Hölzel et al., 2011).
ER concerns how individuals deal with their emotions and how they experience and express them. ER studies have been broadened due to the relationship between this construct and psychological disorders (Coutinho et al., 2010). Coutinho et al. (2010) conceptualize ER difficulties in six dimensions: limited access to ER strategies, non-acceptance of emotional responses, lack of emotional consciousness, difficulty in controlling impulses, difficulty in acting according to goals, and lack of emotional clarity.
ER includes the individuals’ coping strategies for dealing with intense emotions, adaptive or not (Leahy et al., 2013). The study by Garnefski and Kraaij (2007) demonstrates that there is a significant inverse association between symptoms of anxiety, depression and ER strategies (Coutinho et al., 2010). Although anxiety, depression and stress are considered distinct phenomena, they display characteristics in common, including negative affections, emotional distress and physiological alterations, composing a tripartite model (Vignola & Tucci, 2014).
Nowadays, increased levels of depression, anxiety and stress have been observed in the normative (non-clinical) population, with several associated causes. As triggers of these conditions, it is possible to point out: lifestyle, lack of social support, accumulation of activities and increased psychological demands, among others (Bonafé et al., 2016). Clark and Watson (1991) propose a tripartite model for assessing data regarding depression and anxiety, in which specific symptoms of each condition are grouped separately, and shared symptoms of both are grouped. This understanding defines the tripartite model as containing two distinct factors (depression and anxiety) and, also, a mixed factor (overlapping symptoms) designated as distress factor (Martins et al., 2019).
Anxiety can be conceived as a vague and unpleasant feeling of apprehension or fear that arises from the anticipation of dangers; it comes from comparing previous experiences with perceptions of current contexts. Depression, on the other hand, is an emotional disorder related to a feeling of hopelessness. It does not relate to a specific emotion, but to a wide range of them. Stress is defined as an emotional state that varies according to an evaluation of experiences conceived as threatening, harmful, or challenging (Vignola & Tucci, 2014).
The aforementioned constructs relate to performance; thus, a certain amount of anxiety can be useful, functional, and even necessary to enable actions. Anxiety can also be understood as a natural reaction when it induces the prevention and reduction of effects in situations perceived as intimidating (Reis et al., 2017). However, after certain limits, anxiety levels generate maladaptations, and, in test contexts, a decrease in performance (Casari et al., 2014).
The study by Dias (2014), whose sample consisted of 187 undergraduate students, depicts the relation between anxiety and academic stress, which is observed in the following dimensions: demands of academic life, evaluative pressures, and parental pressures. Dias (2014) found positive correlations, as an increase in anxiety creates episodes of academic stress, with a significant impact on performance. Additionally, this study points to the relation between depressive symptoms and performance, demonstrating impairments both in performance and social relationships. It is also pointed out that psychic illnesses during undergraduation range from 15 to 25 %.
There are several stress factors in academic life, but, in this context, situations in which students are tested can emerge as one of stress main sources (Casari et al., 2014). Research carried out by Loricchio and Leite (2012) indicates that the perspective of professional qualification constitutes a stress factor for the Brazilian Bar Association (OAB) exam applicants. The findings indicate that 65.2 % of those who passed and 75 % of those who failed were facing some kind of stress. This research demonstrates significant approval among applicants displaying a lower degree of anxiety; it also relates stress and anxiety to worse performance on the exam.
The OAB exam is taken by graduates in Law who seek admission to this class entity, representing a strong stressor for this population (Loricchio & Leite, 2012). It has been carried out in a unified manner throughout Brazil, since 2009. Its national approval rates are considered low (OAB, 2018).
Nowadays, it is suggested that Mfs-based interventions can function as a powerful strategy to optimize performance. Even though it was designed for a different context, the study by Carraça et al. (2018), found alterations in performance, levels of Mfs, and psychological flexibility in professional soccer players after taking an eight-week program. The randomized pilot study by García-Rubio et al. (2016) examined the effectiveness of a brief four-session Mfs intervention in elementary school students. It was found that academic performance in the experimental group was maintained, while in the control group, a decrease was observed.
Araújo (2018) conducted a study about a three-consecutive-day program of Mfs practices. As a result, it was verified that, in the experimental group, there was a reduction in anxiety, perceived stress, and negative affections. Mfs levels as micro-events moderators, well-being and performance, were examined by Santos (2019). It was observed that more attentive and conscious individuals display better adaptation to daily life, even after negative events, something that directly impacts emotions.
Mfs-based interventions have been extensively studied. Therefore, the findings coming from this area can be extended, as to verify the relation between levels of Mfs in other constructs, as well as possible changes in its explanatory power post interventions. The importance of comprehending this relation can favor emotional health prevention, as this acknowledgment can help develop more targeted and assertive programs. To analyze these modifications in a population about to face a challenge such as the OAB exam, can add to the preparation for this kind of situation, surpassing the preparation solely limited to the theoretical scope, by using emotional balance as a positive factor in performance tests.
Method
Study design
This is a pre-experimental study, presenting a descriptive, analytical and correlational approach aimed at understanding the association and explanatory power of Mfs levels in ER difficulties, depression, anxiety, and stress.
Participants
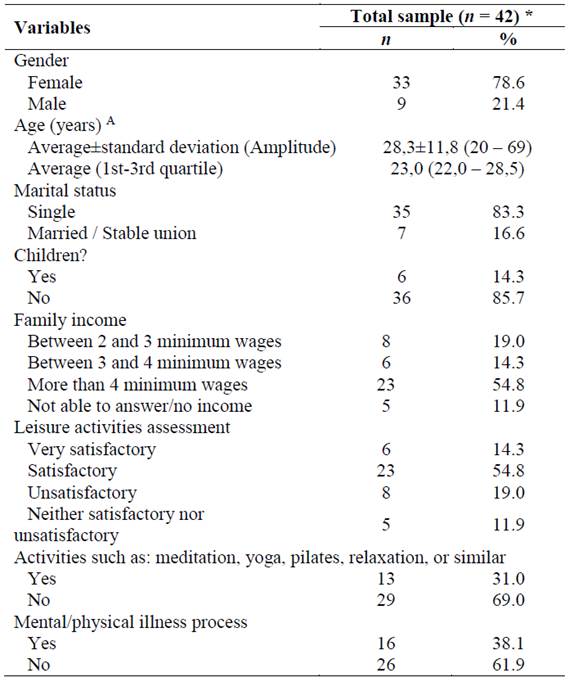
Initially, 72 candidates interested in preparing for the OAB exam registered to take part in this study. The inclusion criteria established were: participation in four meetings, and filling in the pre-and post-test instruments. After the analysis, 42 subjects were selected. The sample is described in Table 1.
Instruments
Sociodemographic Data Questionnaire. Specially designed for this study, it seeks to identify the sample in terms of age, gender, marital status, family income, leisure activities, meditative practices, and previous illness, among others.
Philadelphia Mfs Scale (PMS). This is a five-point, 20-item Likert scale, divided into acceptance and awareness dimensions. The concept of awareness is conceived as comprising the experiential scope, with monitoring of internal and external events. As for the concept of acceptance, it is understood as the action of sticking to the present moment, free from defenses, beliefs, or judgments. The Brazilian version used was adapted by Silveira et al. (2012) and the dimensions presented internal consistency indices of .86 and .82. In this study, the PMS presented acceptable reliability in both dimensions: awareness (αC = .61) and acceptance (αC = .74).
Difficulties in Emotional Regulation Scale (DERS 36). This self-report scale assesses typical levels of ER difficulties. The version used is by Coutinho et al. (2010); it is compartmentalized into six domains: non-acceptance (of negative emotions), objectives (when the subject is taken by negative emotions, presenting inability to engage in goal-directed behaviors), impulse (poor impulse control in the presence of negative emotions), strategies (limited ER strategies perceived to be effective), consciousness (lack of emotional consciousness) and clarity (lack of emotional clarity). The DERS 36 contains 36 items on a five-point scale, to be rated according to the subjects’ perspective: from one (rarely applies to me) to five (almost always applies to me). This instrument was selected due to its high internal consistency (α = .93), good test-retest reliability (rs = .88) and adequate construction. This scale presented minimum reliability of .70 (αC) for the objectives dimension, while the maximum reached 0.91 (αC) in the non-acceptance dimension. Concerning other dimensions of ER, the estimates for reliability remained in the satisfactory classification: impulse (αC =.77); consciousness (αC = .80); strategies (αC = .77); and clarity (αC =.72).
Depression, Anxiety, and Stress Scale (DASS-21). Translated and validated into Brazilian Portuguese by Vignola and Tucci (2014), the DASS-21 is a set of three, Likert-type, four-point self-report subscales. Cronbach's alpha was .92 for depression, .90 for stress, and .86 for anxiety, indicating good internal consistency for each subscale. The analysis and distribution of factors among the factorial subscales indicated that the structure of three distinct factors is appropriate. The estimates indicated satisfactory reliability (αC ≥ .70) in the three dimensions: anxiety (αC = .73), depression (αC = .84) and stress (αC = .89).
Ethical Procedures and Data Collection
The application of a brief Mfs program in OAB exam applicants was approved by the Ethics Committee of the Universidade do Vale do Rio dos Sinos under the number 3080231, according to the precepts of Resolution 466/12 of the National Health Council. The intervention was considered an extension activity in the two participating institutions, which actively advertised it on their media channels and were responsible for participants’ enrollment in the groups. All participants signed the Free and Informed Consent Term.
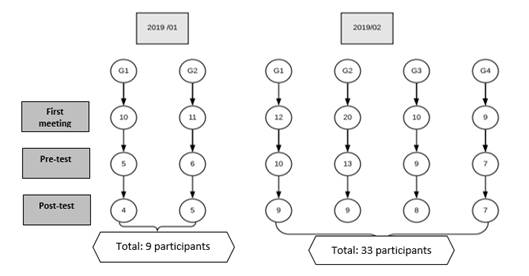
In the first half of 2019, the intervention was simultaneously carried out in two groups. As for the second half of 2019, four simultaneous groups were held. The program started with 72 individuals, and the final sample of the study accounted for 42 participants, who were distributed as described in the flowchart below (Figure 1), which depicts participants' adherence.
Intervention
A five-week group meeting intervention was carried out, as well as an individual meeting after the second week. The group meetings focused on psychoeducation, relevant topics regarding the establishment of study routines, and strategies for taking the exam as well as the theoretical or practical foundations of Mfs. The individual meeting was aimed at understanding in which kind of circumstances each participant lives, seeking to adapt practices and routines to these circumstances. The Mfs techniques used in the intervention were adapted from Mindfulness: How to find peace in a frantic world, by Williams and Penman (2015).
The first meeting focused on information about the fundamentals of Mfs, and on how to organize a study routine for taking the OAB exam. In this opportunity, a meditation activity was conducted, and the term regarding adherence to research and the Free and Informed Consent Term were handed out. Near the end, Time 1 instruments were distributed: PMS, DERS 36 and DASS 21, in addition to the sociodemographic questionnaire. All instruments were applied once more in the sixth meeting (Time 2), except for the sociodemographic questionnaire.
The second meeting was dedicated to an activity of returning to focus, free of judgment or self-criticism. Also on this occasion, food was brought into the activity, providing an opportunity to eat and exercise mindfulness simultaneously. The third meeting was held individually; the fourth focused both on strategies for taking the OAB exam and the concept of autopilot. The fifth meeting focused on self-judgment and self-criticism. In the last one, there was the inclusion of Mfs postures for day-to-day experiences, and instruments regarding Time 2 were filled in. In these meetings, participants were given specific materials on Mfs and also on meditation audios.
Data Analyses Procedures
Results were presented using descriptive statistics absolute and relative distribution (n-%), as well as measures of central tendency and variability. The variables' data distribution was analyzed via Kolmogorov-Smirnov test.
In the linearity relationship of the PMS, when compared to the DERS 36 and the DASS 21, the Pearson Correlation coefficient was used, respecting the classification criteria: very weak (from .00 to .19); weak correlation (from .20 to .39); moderate correlation (from .40 to .69); strong correlation (from .70 to .89); and very strong correlation (from .90 to 1.0) (Cohen, 1988). In order to propose the predictive models, a simple linear regression analysis was performed, taking into account the comparison of regression coefficients between the evaluation periods. For each predictive model, the regression coefficients (β), the p-value of the predictor variables, as well as the coefficient of determination of the model, are indicated.
Results
This study aimed at determining the correlation and explanatory power of two dimensions from the PMS scale (Awareness and Acceptance), on the grounds of the ER difficulties scale and the Depression, Anxiety, and Stress scale. These correlations and explanatory power were measured at two times (before and after the application of a Mfs-based intervention).
The PMS was correlated with the DESR 36 and the DASS 21, according to the results described in Table 2. It was found that, in the initial assessment, there were significant correlation results from the Awareness dimension with the consciousness and clarity dimensions of the DERS 36. These results demonstrated a negative correlation, as well as ratings from weak (.200 ≤ r ≤ .399) to moderate (.400 ≤ r ≤ .699), in both assessment moments (pre and post-intervention). Considering the analysis of the acceptance dimension in the PMS, statistically significant and negative correlations, with moderate intensity, were detected (.400 ≤ r ≤ .699) in the initial assessment of the dimensions: Non-acceptance, Impulse, Strategies and the scale grand total. However, regarding the results observed in the final assessment, the correlations were significant and negative regarding the six dimensions of the DERS 36, with magnitudes ranging from weak (.200 ≤ r ≤ .399) to moderate (.400 ≤ r ≤ .699).
Comparing the analysis of the PMS to the DASS 21, a correlation was identified only in the acceptance dimension. In the initial assessment, the representative results occurred with anxiety and stress. As for the final assessment, significant correlations occurred between the depression and stress dimensions.
Concerning the predictive capacity of the PMS over the DERS 36, it was found that the dimension awareness was representative to explain the consciousness dimension (Pre: βp = -0.512; p = .001; R2 aj = 0.262 / Post: βp = -0.508; p = .001; R2 aj = 0.258) as well as the clarity dimension (βp = -0.332; p = .034; R2 aj = 0.110 / Post βp = -0.466; p= .002; R2 aj = 0.217).
Table 2: Pearson's correlation coefficient of the PMS compared to the DERS 36 and the DASS 21, in the pre and post-intervention assessments
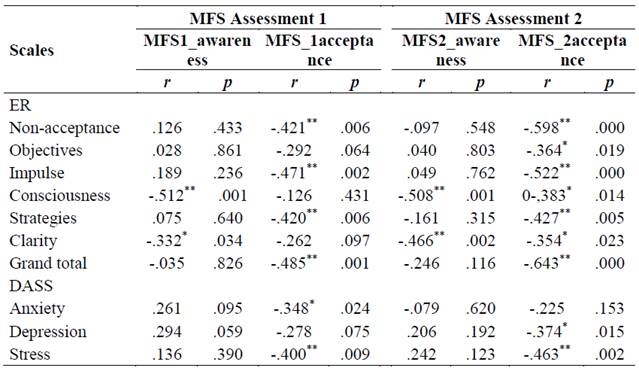
Note: r: Pearson's correlation coefficient. Ratings: very weak (from .00 to .19); weak (from .20 to .39); moderate (from .40 to .69); strong (from .70 to .89) and very strong (from .90 to 1.0).
In the prediction analysis of the acceptance dimension (PMS), the results were representative in the pre-intervention for strategies (Pre: βp = -0.420; p = .006; R2 aj= 0.155), non-acceptance (Pre: βp = -0.421; p = .006; R2 aj = 0.177) and impulse (Pre: βp = -0.471; p = .002; R2 aj = 0.202), as well as for the total score of the DERS 36 (Pre: βp = -0.485; p = .001; R2 aj = 0.216 / Post: βp = -0.643; p < .001; R2 aj = 0.413). As for the post-assessment, this prediction takes place in all dimensions of the DERS 36, with an increase in its explanatory power, highlighting the grand total of the scale that rises from 21.6 %, in the pre-test, to 41.3 % in the post-test.
In relation to the DASS 21, it was observed that acceptance was able to explain 12.1 % of the variations in this scale’s scores for anxiety (βp = -0.348; p = .024; R2 aj= 0.121), in the pre-assessment. However, this result was no longer representative in the post-assessment. The acceptance dimension was also able to explain 14.0 % of the variations in the results in the depression dimension (βp = -0.374; p = .015; R2 aj = 0.140), in the post-intervention period, and in the initial assessment, this relationship was not evidenced. Regarding the predictive power of acceptance on the stress dimension, the results were significant both in the pre-assessment (βp = -0.400; p = .009; R2 aj = 0.139) and in the post-assessment (βp = -0.43; p = .002; R2 aj= 0.214). Therefore, there is evidence that acceptance accounts for 13.9 % of the variations in the stress dimension in the initial assessment, while, in the post-assessment, this proportion significantly increases to 21.4 %. These results are described in Table 3.
Table 3: Simple Linear Regression Models to predict the DERS 36 and the DASS 21 using the PMS, in pre and post-intervention assessments
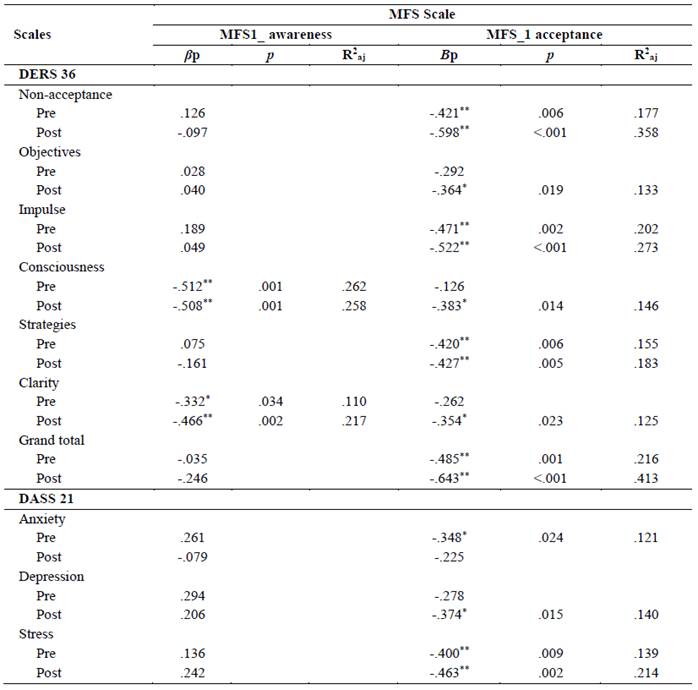
Note: βp: Standardized regression coefficient. R2aj: Determination coefficient of the regression model (meaning the % of the independent variable explanation over the dependent variable).
Discussion
This study aims to observe the correlation and explanatory power of two dimensions in the PMS (awareness and acceptance) regarding the overall result of the DERS 36 and in each of its dimensions (non-acceptance, objectives, impulse, consciousness, strategies, and clarity), as well as in the dimensions of the DASS 21 (depression, anxiety, and stress). The results demonstrate the effects on correlations and explanatory power in a pre and post-period of a Mfs-based intervention applied in the context of preparation for the OAB exam. Research seek to move forward in studies related to Mfs, both theoretical and empirical in academic populations, contributing to the expansion of knowledge on topics related both to well-being and performance (Tatton-Ramos et al., 2016).
In the present study, the relation between the acceptance dimension and the difficulties of ER stands out, especially in the general analysis, in which acceptance explains 41 % of the post-test grand total, maintaining a negative correlation and indicating that higher levels of acceptance relate to lower levels of ER difficulties. When submitted to scrutiny, the explanatory power of Acceptance in each dimension of ER difficulties, an increase is observed in all dimensions after the intervention, even in those in which this relation was not present at the initial time.
In a correlational study counting with 228 subjects, Kotsou et al. (2018) point out acceptance as a robust predictor of psychological health, suggesting that emotional acceptance (which would be contrary to ER difficulties) is a relevant concept in psychological disorders, and also a potent predictor of therapeutic outcomes. Consciousness and clarity regarding emotions are mindfulness components, and one of the goals of this kind of intervention is to focus on the progress of effective ER strategies (Goodall et al., 2012).
The individualized analysis shows that, among the dimensions of the DERS 36, the one that most substantially presents an increase in explanatory power within the acceptance dimension is non-acceptance. It is important to differentiate how acceptance is understood in the constructs considered for this analysis. For the DERS 36, it means a negative reaction to an initial negative emotion; on the Mfs scale, it is the act of not avoiding feeling or thinking through distractions (Chiodelli et al., 2018).
The relation between the awareness dimension and ER difficulties increases from 11 % to 21 % in explanatory power in the clarity dimension in the post-test. The negative correlation demonstrates that greater experiential consciousness can interfere with the reduction of difficulties in clearly understanding emotions. Such findings indicate that the intervention may have contributed to the increase in this explanatory power. It is also noteworthy that the awareness dimension kept a negative correlation and explanatory power very similar to the consciousness dimension in the pre and post-test, evidencing the relation among variables, but suggesting that the intervention itself did not interfere in this scenario.
The link between ER and Mfs levels is validated in several studies. The pilot study by Silveira (2018) with early childhood teachers found negative correlations between the capacity for mindfulness and psychological wear, and the ability to deal with ER. Chiodelli et al. (2018) examined the effects of a brief Mfs program approaching ER techniques on final-year college students. The results revealed a significant reduction in total ER difficulties with a high effect size. On the other hand, Huang et al. (2019), carried out a cross-sectional study with 409 Chinese firefighters who experienced critical accidents at work. In this case, ER was a mediator for mindfulness and post-traumatic outcomes, with emphasis given to the beneficial effects of mindfulness on the firefighter's mental health, as experiencing the moment, in the present, tends to lessen the restriction of feelings.
In the present study, results regarding depression, anxiety and stress were not correlated to the awareness dimension at any times. It can be hypothesized that being aware of the present moment did not result in alterations in the lack of correlation related to measures of depression, anxiety, and stress.
The acceptance dimension presents a weak and negative correlation in the pre-test for anxiety, which is not verified in the post-test. In its turn, the explanatory power that reached 12 % in the pre-test is also absent in the post-test. Acceptance is also related to depression, but only in the post-test, showing a weak and negative correlation and an approximate explanatory power of 14 % in the post-test. As for stress, this dimension keeps strong negative relations in the pre and post-stages. Its explanatory power in the pre-test consisted of 13 % and significant increases in the post-test to 21.4 %.
Research has shown a close relationship between Mfs levels and rates of depression, anxiety, and stress. A cross-sectional study with the participation of 118 students from a medical school indicates that higher levels of acceptance lead to less resistance to fully experiencing the present moment (Andrade & Campos, 2020).
In an almost experimental study, Justo et al. (2016) applied a brief Mfs program to 36 special education teachers. The findings indicate a reduction in depression, anxiety, and stress rates. Also in this direction, Demarzo et al. (2015) present a meta-analysis that demonstrates the relation between quality of life and reducing symptoms of these psychological disorders, with more intense Mfs practices.
In view of the results of this study, the intervention proved to be more robust in the relationship between acceptance and stress, with a significant increase in its explanatory power. The study by Carpena and Menezes (2018), which evaluated the effect of a six-week Mfs program on stress levels in undergraduate and graduate students, points to similar results. It also presents the correlation between levels of Mfs and stress, which is higher in the meditation group, concluding that this type of intervention can help reduce perceived levels of stress.
Fan et al. (2014) carried out a study on the relationship between Mfs and stress with cortisol measures in a group of 34 Chinese students who received a four-week training, and a control group. A significant reduction in basal cortisol levels in the experimental group was observed. Cortisol levels are widely used to predict stress-related health outcomes. The functionality of Mfs training is emphasized, as it produces persistent changes in endocrine function and a greater level of acute effects. Another study, by Greeson et al. (2014), also points to the importance of mindfulness training in college students and young adults. A controlled trial demonstrated improvement in perceived stress, mindfulness, self-compassion, and insomnia problems in the experimental group, supporting the program's effectiveness.
The present study presents a few methodological limitations, such as the sample size for a prediction study. This is the reason why a multiple regression analysis was not conducted. Nevertheless, the theoretical model indicates that there is a relation between Mfs levels and ER aspects, besides depression, anxiety and stress; a fact evidenced in the occasion of this intervention. Indeed, in the post-test, an increase in the explanatory power in several dimensions stands out. Further investigating these correlations can favor the development of actions targeted at emotional health, by expanding applicants' preparation when facing test situations, functioning not only as technical support but mainly as a tool for dealing with emotions. For future studies, it is suggested to analyze these relations in other contexts, in addition to expanding to outcome studies, comparing performance differences.
REFERENCES
Andrade, G. A. & Campos, G. A. L. (2020). Avaliação do nível de atenção plena dos estudantes de medicina em uma instituição de ensino superior de são josé do rio preto segundo a escala filadélfia de mindfulness (EFM). Revista Corpus Hippocraticum, 1(1). [ Links ]
Araújo, G. L. D. L. (2018). Efeitos psicofisiológicos de uma breve intervenção baseada em mindfulness em adultos jovens saudáveis (Tese doutorado). Universidade Federal do Rio Grande do Norte. [ Links ]
Bonafé, F. S. S., Carvalho, J. S., & Campos, J. A. D. B. (2016). Depressão, ansiedade e estresse e a relação com o consumo de medicamentos. Psicologia, Saúde & Doenças, 17(2), 105-119. https://dx.doi.org/10.15309/16psd170201 [ Links ]
Carpena, M. X. & Menezes, C. B. (2018). Efeito da Meditação Focada no Estresse e Mindfulness Disposicional em Universitários. Psicologia: Teoria e Pesquisa, 34, e3441. https://doi.org/10.1590/0102.3772e3441 [ Links ]
Carraça, B., Serpa, S., Rosado, A., & Palmi, J. (2018). The Mindfulness- Based Soccer Program (MBSoccerP): Effects on Elite Athletes. Cuadernos de Psicología sel Deporte, 18(3), 62-85. [ Links ]
Casari, L., Anglada, J., & Daher, C. (2014). Estrategias de aprendizaje y ansiedad ante los exámenes en estudiantes universitarios. Revista de Psicología, 32(2), 243-269. https://doi.org/80111899009 [ Links ]
Chiodelli, R., Mello, L. T. N., Jesus, S. N., & Andretta, l. (2018). Effects of a brief mindfulness-based intervention on emotional regulation and levels of mindfulness in senior students. Psicologia: Reflexão e Crítica, 31(21). https://doi.org/10.1186/s41155-018-0099-7 [ Links ]
Clark L. A., & Watson D. (1991). Tripartite model of anxiety and depression: psychometric evidence and taxonomic implication. Journal of Abnormal Psychology, 100(3), 316-336. https://doi.org/10.1037/0021-843x.100.3.316 [ Links ]
Cohen, J. (1988). Statistical power analysis for the behavioral sciences. Erlbaum. [ Links ]
Coutinho, J., Ribeiro, E., Ferreirinha, R., & Dias, P. (2010). Versão portuguesa da escala de dificuldades de regulação emocional e sua relação com sintomas psicopatológicos. Archives of Clinical Psychiatry, 37(4), 145-151. https://doi.org/10.1590/S0101-60832010000400001 [ Links ]
Demarzo, M. M., Montero-Marin, J., Cuijpers, P., Zabaleta-del-Olmo, E., Mahtani, K. R., Vellinga, A., Vicens, C., López-del-Hoyo, Y., & García-Campayo, J. (2015). The efficacy of mindfulness-based interventions in primary care: a meta-analytic review. The Annals of Family Medicine, 13(6), 573-582. https://doi.org/10.1370/afm.1863 [ Links ]
Dias, E. S. D. (2014). Ansiedade aos exames em estudantes universitários: relação com stresse académico, estratégias de coping e satisfação académica (Dissertação de mestrado). Universidade Lusófona de Humanidades e Tecnologias. [ Links ]
Fan, Y., Tang, Y., & Posner, M. I. (2014). Cortisol level modulated by integrative meditation in a dose-dependent fashion. Stress & Health: Journal of the International Society for the Investigation of Stress, 30(1), 65-70. https://doi.org/10.1002/smi.2497 [ Links ]
García-Rubio, C., Luna Jarillo, T., Castillo Gualda, R., & Rodríguez-Carvajal, R. (2016). Impacto de una intervención breve basada en mindfulness en niños: un estudio piloto. Revista Interuniversitaria de Formación del Profesorado, 30(3), 61-74. [ Links ]
Garnefski, N. & Kraaij, V. (2007). The Cognitive Emotion Regulation Questionnaire: Psychometric features and prospective relationships with depression and anxiety in adults. European Journal of Psychological Assessment, 23(3), 141-149. http://doi.org/10.1027/1015-5759.23.3.141 [ Links ]
Goodall, K., Trejnowska, A., & Darling, S. (2012). The relationship between dispositional mindfulness, attachment security and emotion regulation. Personality and Individual Differences, 52(5), 622-626. https://doi.org/10.1016/j.paid.2011.12.008 [ Links ]
Greeson, J. M., Juberg, M. K., Maytan, M., James, K., & Rogers, H. (2014). A randomized controlled trial of Koru: a mindfulness program for college students and other emerging adults. Journal of American College Health, 62(4), 222-233. https://doi.org/10.1080/07448481.2014.887571 [ Links ]
Hölzel, B. K., Lazar, S. W., Gard, T., Schuman-Olivier, Z., Vago, D. R., & Ott, U. (2011). How does mindfulness meditation work? Proposing mechanisms of action from a conceptual and neural perspective. Perspectives on Psychological Science, 6(6), 537-559. https://doi.org/10.1177/1745691611419671 [ Links ]
Huang, Q., Zhang, Q., An, Y., & Xu, W. (2019). The relationship between dispositional mindfulness and PTSD/PTG among firefighters: The mediating role of emotion regulation. Personality & Individual Differences, 151, 109492. https://doi.org/10.1016/j.paid.2019.07.002 [ Links ]
Justo, C. F., Mañas, I. M., & Martínez, E. J. (2016). Reducción de los niveles de estrés, ansiedad y depresión en docentes de educación especial a través de un programa de mindfulness. Revista de Educación Inclusiva, 2(3). [ Links ]
Kabat‐Zinn, J. (2003). Mindfulness‐based interventions in context: past, present, and future. Clinical psychology: Science and practice, 10(2), 144-156. https://doi.org/10.1093/clipsy.bpg016 [ Links ]
Kotsou, I., Leys, C., & Fossion, P. (2018). Acceptance alone is a better predictor of psychopathology and well-being than emotional competence, emotion regulation and mindfulness. Journal of Affective Disorders, 226, 142-145. https://doi.org/10.1016/j.jad.2017.09.047 [ Links ]
Leahy, R. L., Tirch, D., & Napolitano, L. A. (2013). Regulação emocional em psicoterapia: um guia para o terapeuta cognitivo-comportamental. Artmed. [ Links ]
Loricchio, T. M. B. & Leite, J. R. (2012). Estresse, ansiedade, crenças de autoeficácia e o desempenho dos bacharéis em Direito. Avaliação Psicológica, 11(1), 37-47. [ Links ]
Martins, B. G., Silva, W. R., Maroco, J., & Campos, J. A. D. B. (2019). Escala de Depressão, Ansiedade e Estresse: propriedades psicométricas e prevalência das afetividades. Jornal Brasileiro de Psiquiatria, 68(1), 32-41. https://doi.org/10.1590/0047-2085000000222 [ Links ]
Ordem dos Advogados do Brasil. (2018). Notícias/Pesquisa. https://www.oab.org.br/noticias/pesquisa?pagina=1&argumento=resultado%20exame%20de%20ordem [ Links ]
Pires, J. G., Nunes, C. H. S. D. S., Nunes, M. F. O., Demarzo, M. M. P., Bianchi, M. L., Kotzias, M. M., & Cunha, G. M. M. (2018). Evidência de validade da medida de atenção plena pela relação com outras variáveis. Psico-USF, 23, 513-526. https://doi.org/10.1590/1413-82712018230310 [ Links ]
Reis, C. F., Miranda, G. J., & Freitas, S. C. (2017). Ansiedade e desempenho acadêmico: Um estudo com alunos de Ciências Contábeis. Advances in Scientific and Applied Accounting, 10(3), 319-333. [ Links ]
Santos, T. M. G. (2019). Micro-eventos afetivos diários e o seu impacto no bem-estar e desempenho: o papel moderador da mindfulness (Dissertação de mestrado). Instituto Universitário de Lisboa. [ Links ]
Silva, A. B. (2019). Meditação mindfulness: cultivando o bem-estar e a harmonia do ser (Monografia do Curso de Especialização em Neurociências). Universidade Federal de Minas Gerais, Brasil. [ Links ]
Silveira, A.C., Castro, T.G., & Gomes, W.B. (2012). Adaptação e validação da Escala Filadélfia de Mindfulness para adultos brasileiros. Psico-USF, 17(2), 215-223. https://doi.org/10.1590/S1413-82712012000200005 [ Links ]
Silveira, R. D. R. (2018). Contribuição do Programa de Atenção Plena em professores de educação infantil de um município no litoral sul de Santa Catarina: um estudo piloto (Dissertação de mestrado). Universidade do Extremo Sul Catarinense [ Links ]
Tang, Y., Yang, L., Leve, L. D., & Harold, G. T. (2012). Improving executive function and its neurobiological mechanisms through a mindfulness-based intervention: advances within the field of developmental neuroscience. Child Development Perspectives, 6(4), 361-366. https://doi.org/10.1111/j.1750-8606.2012.00250.x [ Links ]
Tatton-Ramos, T. P., Simões, R. A. G., Niquice, F. L. A., Bizarro, L., & Russel, T. A. (2016). Mindfulness em ambientes escolares: adaptações e protocolos emergentes. Temas em Psicologia, 24(4), 1375-1388. https://doi.org/10.9788/tp2016.4-10 [ Links ]
Vignola, R. C. B. & Tucci, A. M. (2014). Adaptation and validation of the depression, anxiety and stress scale (DASS) to Brazilian Portuguese. Journal of Affective Disorders, 155, 104-109. https://doi.org/10.1016/j.jad.2013.10.031 [ Links ]
Williams, M. & Penman, D. (2015). Atenção Plena: como encontrar a paz em um mundo frenético. Sextante [ Links ]
How to cite: Lopes Menezes, S. R., Ribeiro Beneton, E., & Andretta, I. (2022). Influence of mindfulness levels on emotional regulation, depression, anxiety and stress dimensions in a Brief Intervention Program in candidates for the OAB exam. Ciencias Psicológicas, 16(2), e-2241. https://doi.org/10.22235/cp.v16i2.2241
Authors’ participation: a) Conception and design of the work; b) Data acquisition; c) Analysis and interpretation of data; d) Writing of the manuscript; e) Critical review of the manuscript. S. R. L. M. has contributed in a, b, c, d, e; E. R. B. in c, d, e; I. A. in a, c, d.
Received: August 20, 2020; Accepted: October 10, 2022
 Este é um artigo publicado em acesso aberto sob uma licença Creative Commons
Este é um artigo publicado em acesso aberto sob uma licença Creative Commons
