










Servicios Personalizados
Revista

Articulo
 texto en
texto en  Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
Links relacionados
Compartir

 Permalink
PermalinkCiencias Psicológicas
versión impresa ISSN 1688-4094versión On-line ISSN 1688-4221
Cienc. Psicol. vol.16 no.1 Montevideo 2022 Epub 01-Jun-2022
https://doi.org/10.22235/cp.v16i1.2551
Original Articles
Psychosocial risks and their relationship with occupational health in a hospital

1Universidad Arturo Prat, Chile, nelcastr@unap.cl
2 Universidad Arturo Prat, Chile
The jobs are increasingly demanding, complex and put at risk the health and well-being of people when psychosocial conditions, present in organizational contexts, are inadequate. This study aimed to relate occupational disease based with the psychosocial risks present in a hospital, study possible resources that mitigate these risks and study variables associated with well-being. The method included an observational, analytical, cross-sectional design and a total sample of 480 workers who answered the Suseso/Istas21questionnaire. Linear regression analyzes were performed, initially for the surgery unit, which had presented a case of a pathology under study related to occupational risk, and subsequently for the entire hospital. The results show that quantitative requirements, sense of work and indebtedness are major predictors of the reporting of symptoms in surgery, and that sense of work interacts with quantitative requirements attenuating its effects for the entire hospital. Well-being is associated with mental health and emotional demands. It is concluded that psychosocial risk is associated with illness, but it can be attenuated by resources as the sense of work in a hospital.
Keywords: psychosocial risks; occupational health; workload; public hospitals; sense of work
Los trabajos son cada vez más exigentes, complejos y colocan en riesgo la salud y bienestar de las personas cuando las condiciones psicosociales, presentes en los contextos organizacionales, son inadecuadas. Este estudio tuvo por objetivo relacionar la enfermedad laboral con los riesgos psicosociales presentes en un hospital, estudiar posibles recursos que atenúen estos riesgos y estudiar variables asociadas al bienestar. El método incluyó un diseño observacional, analítico, transversal y una muestra total de 480 funcionarios que respondieron el cuestionario Suseso/Istas21. Se realizaron análisis de regresión lineal, inicialmente para la unidad de cirugía, que había presentado un caso de una patología en estudio relacionada a riesgo laboral, y posteriormente para todo el hospital. Los resultados muestran que las exigencias cuantitativas, el sentido del trabajo y el endeudamiento son mayores predictores sobre el reporte de síntomas en cirugía, y que el sentido del trabajo interactúa con las exigencias cuantitativas atenuando sus efectos para todo el hospital. El bienestar está asociado a la salud mental y las exigencias emocionales. Se concluye que el riesgo psicosocial se asocia a enfermedad, pero puede ser atenuado por recursos como el sentido del trabajo en un hospital.
Palabras clave: riesgos psicosociales; salud laboral; carga de trabajo; hospitales públicos; sentido del trabajo
Os trabalhos são cada vez mais exigentes, complexos e colocam em risco a saúde e o bem-estar das pessoas quando as condições psicossociais, presentes nos contextos organizacionais, são inadequadas. O objetivo deste estudo foi relacionar a doença ocupacional com os riscos psicossociais presentes em um hospital, estudar os possíveis recursos que atenuam esses riscos e estudar as variáveis associadas ao bem-estar. O método incluiu um desenho observacional, analítico, transversal e uma amostra total de 480 funcionários que responderam ao questionário Suseso/Istas21. Foram realizadas análises de regressão linear, inicialmente para a unidade cirúrgica, que havia apresentado um caso de uma patologia em estudo relacionada ao risco ocupacional, e posteriormente para todo o hospital. Os resultados mostram que as exigências quantitativas, o sentido de trabalho e o endividamento são os maiores preditores sobre o relato de sintomas em cirurgia, e que o sentido de trabalho interage com as demandas quantitativas atenuando seus efeitos para todo o hospital. O bem-estar está associado à saúde mental e às exigências emocionais. Se conclui que o risco psicossocial está associado à doença, mas pode ser atenuado por recursos como o sentido do de trabalho em um hospital.
Palavras-chave: riscos psicossociais; saúde ocupacional; carga de trabalho; hospitais públicos; sentido do trabalho
Working conditions have an impact on health. When psychosocial work conditions have a high probability of seriously damaging the health of workers, we can speak of psychosocial risks at work (Moreno, 2011). These are, then, those characteristics of work conditions that can affect health and among which are the organization and conditions of employment, active work and skills development, psychological demands, relationships within work, double home-work presence.
Within the models that relate psychosocial conditions with stress, there are two that have sufficient empirical support to clearly relate psychosocial factors with illness: the demand-control model of Karasek, Theorell and Johnson and the effort-reward imbalance model of Siegrist (Luceño et al., 2005). The demand-control model posits that the sources of stress at work are given by the work requirements or demands and the control that one has over them, which would generate psychological tension (Karasek & Theorell, 1990). The second model added the interaction effect of social support, as greater morbidity and mortality due to this last variable were evidenced (Johnson & Hall, 1994).
A global descriptive analysis of the situation of psychosocial risk prevention in 132 countries found that 64 % have not included mandatory assessment of psychosocial risks in their occupational health and safety legislation (Chirico et al., 2019). Poor psychosocial working conditions increase the probability of morbidity and substantially limit the quality of life and the possibilities of maintaining a paid job. Lee et al. (2018) proposed a model that incorporates the variables that influence job insecurity and that determine consequences on the health and well-being of the worker, on their attitudes, their behavior and their work performance. Among these variables are organizational and individual factors, organizational and individual background and conditions of the organization's environment. High indebtedness, that is, the difficulty to pay debts from salary contributes to job insecurity and can originate from individual or organizational factors, conditions of the organization's environment or a combination of factors. A recent study of 64,934 people by Magnusson et al. (2018) and which included several countries and organizations, found that job strain is consistently related to a loss of 1.7 average years of healthy life between 50 and 75 years, this being higher in men and in lower occupational positions.
In the area of health, the psychosocial environment and stress in health workers in public centers have been studied, assessing the effect of psychosocial risks on symptoms related to perceived stress. It has been observed that high levels of cognitive, sensory and emotional psychological demands, together with low possibilities for development and lack of meaning at work, are associated with perceived stress (García et al., 2015). Research has shown that antecedent variables intervene in the sense or meaning of work; such as personal and family situation, work history and experiences, and the macro-socioeconomic environment, which influence central variables constituted by the centrality of work as a vital role, social norms about work, valued results of work, the importance of work goals and identification with the work role, which make up different patterns of meaning of work that impact on the expectations and work results of the employee and the organization (Harpaz & Fu, 1993; MOW International Research Team, 1987).
When stress becomes chronic, emotional exhaustion, depersonalization, and lack of accomplishment appear in the worker, a phenomenon called burnout syndrome, which in the Latin American health sector shows a frequency that ranges between 2.1 % and 76 %, with greater exhaustion found in areas of intensive care, oncology, emergency, surgery, internal medicine and anesthesiology; associated with conditions of overload of working hours, an excess of labor demand and the lack of preventive measures (Loya-Murguía et al., 2018).
Working in health requires certain capacities to perform the work based on the present demands, the mental and physical capacities and the state of health of the employee and at the same time that he or she can maintain a state of well-being. Efforts are currently being made in the direction of predicting illness at work from psychosocial risks. The role of emotional intelligence has been shown to have an effect on cardiovascular disease, so that men with low emotional regulation and women with low intrapersonal understanding have a higher risk of cardiovascular disease (Núñez & Castillo, 2017). It has been seen that in administrative employees, emotional and social skills such as the recognition of emotions, the identification and expression of positive emotions, perception, persuasion, assertive communication and the development of skills have a positive influence on job competencies (Duque et al. , 2017). A systematic review of nursing professionals found that high-demand working conditions and limited resources are associated with psychosocial risks such as fatigue, stress, and burnout (Canales et al., 2016). Leadership, of a transformational type, would contribute to the relationship with the health and well-being of the employee by promoting affective aspects of personal well-being and its relationship with less psychological discomfort and greater job satisfaction would be confirmed (Perilla & Gómez, 2017). In addition, it has been reported that role conflict (one of the most important psychosocial risks at work) and role ambiguity in addition to engagement are significant predictors of job satisfaction (Orgambídez et al., 2015).
The demands, such as requirements, overload, pressure, etc., and the resources available to the worker such as the sense of work, autonomy, feedback, social support, among others, have direct and indirect effects on work stress and motivation, with reciprocal relationships existing between these variables. Demands are generally the main predictors of burnout or psychosomatic problems at work, while resources predict job satisfaction, motivation and commitment. Demands and resources present interactions in which, for example, resources can cushion the impact of demands on stress and/or discomfort, mitigating their effects. Demands can also interact with work resources, amplifying their impact on motivation or commitment (Bakker & Demerouti, 2013).
In this context, the purpose of this study is to relate the disease to the psychosocial risks present in a hospital, to study possible resources that mitigate these risks, and to study variables associated with well-being. For this, operationally the report of stress symptoms is considered as illness, and indicators of vitality in the workers as well-being.
Materials and Method
The sample was probabilistic and reached 480 workers, representing 60 % of the total; of them 65 % were women and 35 % men. It was made up of workers from a medium-complexity public hospital in southern Chile, that is, with some specialties such as medicine, surgery, traumatology, among others, and who had answered the long version of the Suseso/Istas21 psychosocial risk survey in the December 2018 to January 2019 period, applied internally by the hospital through its risk prevention unit.
The instrument used in this research was the scale to measure psychosocial risks Suseso/Istas21 in its long version of 142 questions, validated and standardized in Chile by Alvarado et al. (2012) and which is based on the Copenhagen Psychosocial Questionnaire (COPSOQ) from the Danish National Institute for Occupational Safety and Health. The Suseso/Istas21 questionnaire consists of a general section of 53 questions that inquire about sociodemographic data, work and current employment, salary and indebtedness, medical licenses and absenteeism, accidents and work-related illnesses; but it also incorporates a division of questions on health and personal well-being, which contains dimensions that investigate the consequences of psychosocial risk through the scales of general health (5 items), mental health (5 items) and vitality (4 items) contained in the SF-36 questionnaire (Short Form Survey 36 items), developed by Ware and Sherbourne (1992) and a 12-item scale that measures report of stress symptoms based on the scale of Setterlind and Larsson (1995). Then comes a specific section of 89 questions that measure psychosocial risk, grouped into 5 dimensions: the psychological demands dimension, which in turn includes the 5 subdimensions quantitative psychological demands (QD), cognitive psychological demands, emotional psychological demands, demands to hide emotions and sensory psychological demands. The dimension of active work and possibilities of development that includes the 5 subdimensions of influence, control over working time, possibilities of development at work, sense of work and integration in the company. The dimension of social support in the company and quality of leadership that includes the 5 subdimensions of clarity of role, conflict of role, quality of leadership, quality of relationship with superiors and quality of relationship with co-workers. The compensation dimension that includes the 3 subdimensions of esteem, insecurity regarding the employment contract and insecurity regarding the specific characteristics of the job. The double presence dimension that includes the sub-dimension concern about housework. The items have a 1-5 Likert scale format that goes from always to never and includes some items in reverse order.
The variables of interest considered were: sex, age, dimensions and subdimensions of psychosocial risk, indicators of health and personal well-being such as general health (SG), mental health (SM), vitality (VT), report of stress symptoms (SR), aspects of work and employment.
Internal consistency analyzes of the instrument and descriptive analyzes of the variables were performed using the SPSS 25 software. Next, for each department or unit of the hospital, the presence of high psychosocial risks and whose prevalence was greater than 50 % was identified in each of the dimensions measured by the instrument; this made it possible to order the risk in the different units in a descending manner using a risk sum indicator or risk factor. Possible resources or protective factors were also identified, such as those risks of a low level and whose prevalence was greater than 50 %, deepening later in the study of the sense of work as this is a resource or protective factor present in a large part of hospital units. Subsequently, correlation analyzes were carried out, followed by multiple regression for the prediction of illness and well-being with their respective analyzes of fulfillment of assumptions. The report of stress symptoms and well-being indicators of vitality in the employees were considered operationally as disease and well-being, respectively. These regression analyzes were first performed on a unit, surgery, in which a Sentinel case or event had occurred (which is the investigation of a pathology that may be related to risk factors present in work tasks) and then the effect of these same predictor variables on the general hospital, as well as the modulating effect of the sense of work on the report of stress symptoms.
This research was approved by the respective Ethics Committee of the hospital. The application of the Suseso/Istas21 questionnaire has government regulations and a protocol for its application, which considers both informed consent and the guarantees of anonymity and confidentiality of the participating workers.
Results
The applied instrument behaves reliably in all its psychosocial risk subscales, obtaining an average Cronbach's Alpha of .83, exceeding all the value of .70, obtaining for the health subscales .72 for SG, .83 for SM, .78 for VT and .93 for SR, achieving adequate levels of reliability.
Of the participants, 39 % belonged to the professional class, 34 % administrative and 27 % technicians. The ages corresponded to 43 % in the range of 26 to 35 years, 18 % from 46 to 55 years, 7 % less than 26 years and 4 % were more than 55 years. Regarding seniority in their work, 28 % were between 5 and 10 years, 26 % more than 10 years, 19 % more than six months and up to 2 years, 18 % more than two to 5 years and 9 % less than six months. 85% worked full-time, 9 % part-time, and 6 % stated they worked without fixed hours. 65 % worked fixed daytime hours in the morning or afternoon and 35 % worked rotating morning, afternoon or night shifts. The type of contract was mainly temporary or contract with annual renewal in 69 % and only 22 % had an indefinite or permanent contract, while 9 % referred to another type of contractual relationship.
For the hospital in general and in comparison with the surgery unit, in which the Sentinel case is presented, higher means were obtained in the SG health indicators (M = 71.9, SD = 18.2 versus M = 68.3, SD = 18.8), in SM (M = 68.8, SD = 19.7 versus M = 66.2, SD = 19.4) and lower levels in SR (M = 27.5, SD = 18.4 versus M = 31.4, SD = 18.3). These differences were not significant, however, it is significant in the case of VT (M = 62.5, SD = 18.9 versus M = 55.9, SD = 16.1; t(478) = 2.08; p = .038), where the surgery unit obtains a lower level of vitality or well-being.
A total of 14 % admitted having a derived or work-related illness and 44 % presented medical license in the general hospital versus 18 % who admitted having an illness in surgery and 66 % presented medical license in this unit. 28 % presented licenses greater than 9 days.
Regarding indebtedness, 100 % in the surgery unit acknowledge having debts versus 88.2 % in the rest of the hospital who do indicate having debts, observing a significant relationship between unit and indebtedness χ2(1) = 3.870, p < .05 and a risk OR = 1.133 regarding not present debts.
Table 1 shows different hospital units together with the prevalence of high psychosocial risk (greater than 50 %) for the dimensions: psychological demands, active work and development possibilities, social support and leadership quality, compensations and double presence. It also shows the sum of these risk factors, the observed protective factors, highlighting the sense of work as the main common protective factor in the units, the report of symptoms, levels of vitality and frequency of reporting of having a disease diagnosed and/or caused by work.
Table 1: High psychosocial risks in hospital units
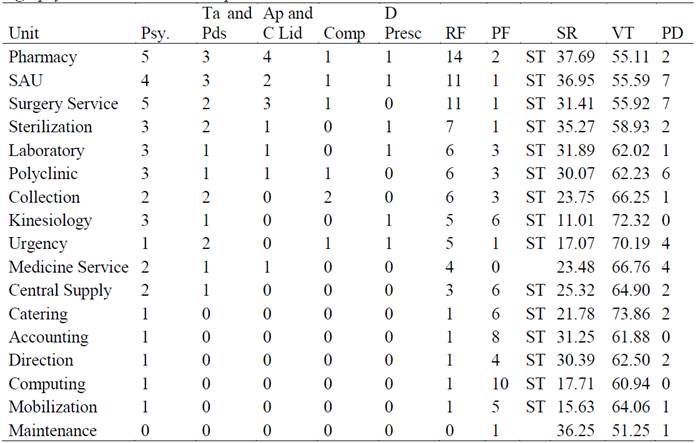
Notes: Psy.: Psychological demands; Ta and Pds: Active work and development possibilities; Ap and C Lid: Social support in the company and quality of leadership; Comp: Offsets; D Presc: Double presence; RF: Risk factor; PF: Protective factor; SR: Sympton report; VT: Vitality; PD: Professional disease; SAU: User service. Own elaboration, based on Suseso/Istas21 survey.
Among the units that presented the greatest risk factors was the pharmacy unit in which 18 % of disease reports were observed, in the user service system unit that reported disease in 37 %, in surgery with 18 % of reported illness, 26 % in polyclinic and 14 % in sterilization. As the psychosocial risk in the units decreases, the report of symptoms and illness decreases and the number of protective factors and vitality levels increases.
In order to study which are the most important variables in the prediction of disease in the Surgery unit that presented the Sentinel case, several correlation and multiple linear regression analyzes were carried out with the stepwise method. Because it was observed that the sense of work can be an important variable to study as a possible protective factor, since it was present in almost all the units, it was considered in the final solution.
In the case of illness, in the surgery unit it was observed that the report of symptoms (M = 1.3, SD = 0.7) correlated significantly with the quantitative demands in the unit (r = .66, p < .01), with the risk due to serious indebtedness (r = .476, p < .01), and with the risk derived from the lack of sense of work (r = .465, p < .01). Table 2 shows the results of the stepwise regression for the disease case.
Table 2: Stepwise multiple regression in the surgery unit (Sentinel case) for reporting symptoms or disease
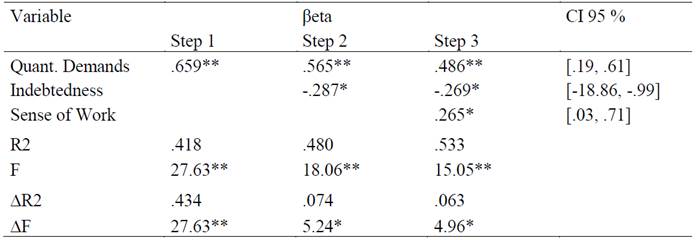
Notes: CI: Confidence interval; Quant. Demands: Quantitative demands; R2: Coefficient of determination; F: Statistical F. Own elaboration, based on Suseso/Istas21 survey. * p < .05. ** p < .01.
These variables would be contributing 53.3 % to explain the disease in this unit or department. Table 2 shows that indebtedness reappears, but in this case without difficulty in dealing with debts, as a variable that contributes negatively to the reporting of symptoms. For the case of the general hospital, shown in Table 3, these variables would only be explaining 29 % of the report of symptoms and serious indebtedness here would be contributing positively to the explanation of the disease.
Table 3: Stepwise multiple regression for hospital for symptom reporting or illness

Notes: CI: Confidence interval; R2: Coefficient of determination; F: Statistical F. Own elaboration, based on Suseso/Istas21 survey. * p < .05. ** p < .01.
To determine if the interaction between the quantitative demands and the sense of work contributes significantly to the prediction of illness, a multiple linear regression with the Introduce method was carried out. It was observed that the variable quantitative demands and sense of work (β = .314, p < .01) together with the variable severe indebtedness (β = .107, p< .01) predict the report of symptoms or illness (R 2 = .101, F = 25.81, p < .01)
The results show that the interaction variable is significant in the prediction of illness in the general case of the hospital and that, together with the variable severe indebtedness, they predict the reporting of symptoms or illness by 10 %. To study the protective effect of this interaction, Figure 1 was created, which allows us to observe the direction that this interaction takes in relation to the effect on symptom reporting.
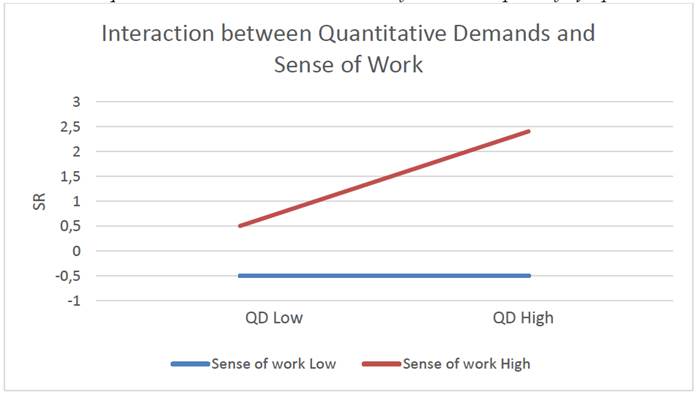
The graph shows the protective effect of the direction of work; when the quantitative demands are high and the psychosocial risk from the sense of work is high, the report of symptoms is higher than when the quantitative demands are high and the risk of the sense of work is low (protective factor).
To study the variables that best predict well-being in general in the hospital, several correlation and multiple linear regression analyzes were carried out with the stepwise method (Table 4).
Table 4: Stepwise regression for vitality or well-being in the hospital
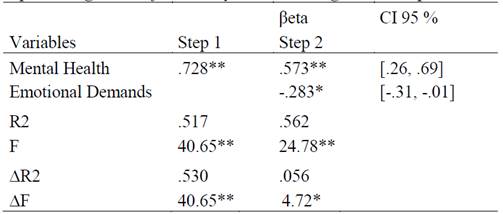
Notes: CI: Confidence interval; R2: Coefficient of determination; F: Statistical F. Own elaboration, based on Suseso/Istas21 survey. * p < .05. ** p < .01.
It can be seen that in 56.2 % the variables mental health and emotional demands explain well-being, that is, the vitality or energy available in the workers. In the case of emotional demands, its contribution is negative, since it is a variable that measures emotional psychosocial risk.
Discussion
The objective of this study was to relate the disease with the psychosocial risks present in a hospital, to study possible resources that mitigate these risks and to study variables associated with well-being. For the disease, the report of stress symptoms was operationally considered and for well-being, indicators of vitality.
The Suseso/Istas21 scale behaved reliably, showing itself to be suitable for measuring psychosocial risks in a hospital, which is consistent with its growing use for research in the health sector (García et al., 2015; Villarroel et al., 2018). Regarding participants, the results showed that the proportion of women is higher than that of men in the hospital and that the staff is under a temporary or annual fixed-term contract modality; both aspects are similar to what was found in other research in health centers (Ansoleaga, 2015; Vidal et al., 2017).
The gender perspective in health has been increasingly investigated (Schraiber & d’Oliveira, 2014). Research shows that women perceive psychosocial risk differently from men, are affected by it and deal with its effects differently (Cifre et al., 2011), somatize stress more and report more physical and pain symptoms than men (Crespo, 2014), however, there would be no differences in general labor well-being (Echevarría & Santiago, 2017). The results go in the same direction, observing that those who recognize a work-related illness are 9.7 % of men versus 16.7 % of women (OR = 1.88; 95 % CI, 1.09-3.49).
The participating staff was distributed between professionals, administrative and technical staff in almost equal parts and their ages corresponded mainly to a range of 26 to 55 years and seniority ranging from 5 to 10 years or more, most of them working full time with fixed schedule and 35 % subjected to shifts. It has been seen that these are associated with illness in the health area when the shifts imply changes in schedule that cause inconveniences in the workers (Castro, 2018).
Regarding the objective of relating the disease with the psychosocial risks present in a hospital and studying possible resources that mitigate these risks, the results showed that the psychosocial risk tends to be different in the different departments or units of a hospital and that it is associated with the number of dimensions at high risk or risk factors, with a higher report of symptoms, with lower levels of vitality or well-being, and with a higher report of work-related illnesses. According to the demand-control model and the effort-reward-imbalance model, greater illness is expected in those with high demands, low autonomy or control, and low social support. These results support both models since they show that the units or departments with higher reports of symptoms and lower vitality tend to be affected in all dimensions. Consistent with the above, among these units with higher risks is surgery, in which a sentinel case or one of occupational disease was presented and which shows a trend towards worse health indicators: more illness reporting than the hospital in general, a higher percentage of medical licenses, lower well-being or vitality.
Additionally, indebtedness appears in this study as an important variable to consider and that is significantly related to the reporting of symptoms and illness. In this regard, Espinosa (2004) shows how changes in mode and lifestyle influence the health-disease process.
In the present investigation, possible protective factors against the development of the disease were also studied, selecting the sense of work because it appears transversally in almost all the units with low risk and with a high prevalence of more than 50 % of the workers of each unit. Vidal et al. (2017) found that the dimension with the highest mean value in a hospital corresponded to intrinsic motivation over the managerial support factor and the workload factor in the evaluation of the quality of life of health personnel. The sense of work sub-dimension would be contributing to the intrinsic motivation of work in hospitals, so further study of it is very important. Evidence has shown that the sense of work is associated with well-being in health, especially through transformational leadership that influences interpretations and beliefs about the sense of work (Peiró & Rodríguez, 2008) and it has also been associated with positive emotions and happiness at work (Seligman, 2011).
The results showed that there are significant positive, moderate to strong associations between feeling overwhelmed, without mood, with poor sleep, with chest tightness, feeling irritable, short of breath, among others reported symptoms with the level of quantitative demands at work, with the risk in the sense of work and with the difficulties to face the Indebtedness. In the case of the Surgery unit, these variables would be explaining 53.3 % of the symptoms, while for the general hospital they would explain only 29 %.
For some authors (Villarroel et al., 2018) social support and the quality of leadership is central in the development of interventions in high and low complexity hospitals, aimed at lowering the risks of psychological demands (which incorporates quantitative demands), indebtedness, active work and development possibilities (which incorporates the sense of work risk).
This research shows that there are resources that cushion the impact of psychosocial risks over the disease. It can be pointed out that in this study the sense of work would be acting in the hospital as a protective factor since the interaction with the quantitative demands is significant in the prediction of the report of symptoms and the results of the interaction analysis show that with the low risk of the sense of work, the symptom reporting is lower in the hospital. These results are consistent and go in the same direction with what is predicted by the theory of demand and labor resources (Bakker & Demerouti, 2013), being able to consider the sense of work as a resource that mitigate the effect of quantitative demands, generating a lower reporting of stress symptoms.
Similarly, the low quantitative demands attenuate the symptom report when the risk due to sense of work is high, eventually behaving as a protective factor in other hospitals where the quantitative demands are lower and other risks appear higher, for example the sense of work, the quality of leadership, relationships with colleagues or contractual conditions.
Beyond the resources that scientific literature has traditionally identified as autonomy, variety of tasks, feedback, among others, to enrich work and develop motivation (Hackman & Oldham, 1976), future research could explore, in centers of health, if the high prevalence of risks with a low level of psychosocial risks, act as possible protective factors in the interaction with higher level risks, producing fewer reports of symptoms or illness.
Regarding the objective of studying variables associated with well-being, the results showed that the well-being or vitality of hospital workers is strongly explained in 56.2 % by mental health and by lower emotional demands. Thus, calmer workers, less nervous or worried, more animated, happier and less tired or emotionally worn out, will face their work with more energy and enthusiasm. A systematic review of working conditions in hospitals, especially nursing staff in Chile, shows that they operate in contexts of high labor demands, lack of materials and limited resources (Canales et al., 2016); A similar situation occurs in other countries, where these conditions also affect aspects such as images culturally associated with care associated more with women (Pereyra & Micha, 2016). This poses a challenge for hospital management so that there can be a balance between the demand and need for efficiency of services with attention to conditions, quality of work life and the social needs of health workers (Blanch, 2014) improving their mental health and well-being.
Conclusions
This research contributed to the understanding of occupational health and well-being in an Organization, knowing the risk and illness of different departments or units of a hospital, through a simple methodology, which was to consider high psychosocial risks and that at the same time had a prevalence greater than 50 % in order to observe clearer effects. Likewise, it contributed in showing how to explore potential resources within the same psychosocial risks, when those are low in a prevalence greater than 50 %, acting as possible protective factors that cushion the effect of the demands on the disease, as was the case of sense of work. It contributed to the prediction of the disease, considered as report of symptoms, and to the understanding of well-being, considered as vitality in workers at a health center. It is possible to conclude the importance of recognizing, supporting and favoring the development of the Sense of work as a resource, which probably exists in many hospitals, but which may not be receiving the required attention due to its great relevance as a stress protector.
The limitations of this study are that the sample consisted of only one hospital and that the cross-sectional quantitative methodology used does not allow causality to be concluded despite the regression analyzes carried out, since this requires an investigation with an experimental design.
REFERENCES
Alvarado, R., Pérez-Franco, J., Saavedra, N., Fuentealba, C., Alarcón, A., Marchetti, N., & Aranda, W. (2012). Validación de un cuestionario para evaluar riesgos psicosociales en el ambiente laboral en Chile. Revista Médica de Chile, 140(9), 1154-1163. https://doi.org/10.4067/S0034-98872012000900008 [ Links ]
Ansoleaga, E. (2015). Indicadores de salud mental asociados a riesgo psicosocial laboral en un hospital público. Revista Médica de Chile, 143(1), 47-55. https://doi.org/10.4067/S0034-98872015000100006 [ Links ]
Bakker, A. & Demerouti, E. (2013). La teoría de las demandas y los recursos laborales. Journal of Work and Organizational Psychology, 29(3), 107-115. https://doi.org/10.5093/tr2013a16 [ Links ]
Blanch, J. (2014). Calidad de vida laboral en hospitales y universidades mercantilizados. Papeles del Psicólogo, 35(1), 40-47. [ Links ]
Canales, M., Valenzuela, S., & Paravic, T. (2016). Condiciones de trabajo de los profesionales de enfermería en Chile. Enfermería Universitaria, 13(3), 178-186. https://doi.org/10.1016/j.reu.2016.05.004 [ Links ]
Castro, N. (2018). Riesgos psicosociales y salud laboral en centros de salud. Ciencia & Trabajo, 20(63), 155-159. https://doi.org/10.4067/S0718-24492018000300155 [ Links ]
Chirico, F., Heponiemi, T., Pavlova, M., Zaffina, S., & Magnavita, N. (2019). Psychosocial Risk Prevention in a Global Occupational Health Perspective. A Descriptive Analysis. International Journal of Environmental Research and Public Health, 16(14), 1-14. https://dx.doi.org/10.3390/ijerph16142470 [ Links ]
Cifre, E., Salanova, M., & Franco, J. (2011). Riesgos Psicosociales de hombres y mujeres en el trabajo: ¿Una cuestión de diferencias? Gestión Práctica de Riesgos Laborales, 82, 28-37. [ Links ]
Crespo, J. (2014). El bienestar laboral de los profesionales de la medicina: una comparativa iberoamericana. Revista del Centro de Estudios de Sociología del Trabajo, (6), 39-71. [ Links ]
Duque, J., García, M., & Hurtado, A. (2017). Influencia de la inteligencia emocional sobre las competencias laborales: un estudio empírico con empleados del nivel administrativo. Estudios Gerenciales, 33(144), 250-260. https://doi.org/10.1016/j.estger.2017.06.005 [ Links ]
Echevarría, K. & Santiago, R. (2017). Percepción del bienestar laboral de los empleados: estudio comparativo según su género. Revista Internacional Administración & Finanzas, 10(2), 17-27. [ Links ]
Espinosa, L. (2004). Cambios del modo y estilo de vida; su influencia en el proceso salud-enfermedad. Revista Cubana Estomatología, 41(3). [ Links ]
García, A., Gutiérrez, M., Bellón, J., Muñoz, C., & Fernández, J. (2015). Entorno psicosocial y estrés en trabajadores sanitarios de la sanidad pública: diferencias entre atención primaria y hospitalaria. Atención Primaria, 47(6), 359-366. https://doi.org/10.1016/j.aprim.2014.09.003 [ Links ]
Hackman, J. R. & Oldham, G. R. (1976). Motivation through the design of work: Test of a theory. Organizational Behavior & Human Performance, 16(2), 250-279. https://doi.org/10.1016/0030-5073(76)90016-7 [ Links ]
Harpaz, I. & Fu, X. (1993). The meaning of work at various organizational levels. International Journal of Commerce and Management, 3(3/4), 31-52 https://doi.org/10.1108/eb047280 [ Links ]
Johnson, J. V. & Hall, B. M. (1994). Social support in the work environment and cardiovascular disease. En S. Shumaler & S. Czajkowski. (Eds.), Social support and cardiovascular disease (pp. 145-166). Baywood. https://doi.org/10.1007/978-1-4899-2572-5_7 [ Links ]
Karasek, R. & Theorell, T. (1990). Healthy Work, Stress, Productivity and the Reconstruction of Working Life. Basic Books. [ Links ]
Lee, C., Huang, G., & Ashford, S. (2018). Job insecurity and the changing workplace: Recent developments and the future trends in job insecurity research. Annual Review of Organizational Psychology and Organizational Behavior, 5, 335-359. https://doi.org/10.1146/annurev-orgpsych-032117-104651 [ Links ]
Loya-Murguía, K. M., Valdez-Ramírez, J., Bacardí-Gascón, M., & Jiménez-Cruz, A. (2018). El síndrome de agotamiento en el sector salud de Latinoamérica: revisión sistemática. Journal of Negative & No Positive Results, 3(1), 40-48. https://doi.org/10.19230/jonnpr.2060 [ Links ]
Luceño, L., Martín, J., Jaén, M., & Diaz, E. (2005). Evaluación de factores psicosociales en el entorno laboral. eduPsykhé, 4(1), 19-42. [ Links ]
Magnusson, L., Westerlund, H., Chungkham, H. S., Vahtera, J., Rod, N. H., Alexanderson, K., & Head, J. (2018). Job strain and loss of healthy life years between ages 50 and 75 by sex and occupational position: analyses of 64 934 individuals from four prospective cohort studies. Occupational and Environmental Medicine, 75(7), 486-493. https://doi.org/10.1136/oemed-2017-104644 [ Links ]
Moreno, B. (2011). Factores y riesgos laborales psicosociales: conceptualización, historia y cambios actuales. Medicina y Seguridad del Trabajo, 57(1), 4-19. https://dx.doi.org/10.4321/S0465-546X2011000500002 [ Links ]
MOW International Research Team. (1987). The meaning of working. Academic Press. https://doi.org/10.1002/job.4030100109 [ Links ]
Núñez, M. & Castillo, R. (2017). El papel de la inteligencia emocional en la enfermedad cardiovascular. Gaceta Sanitaria, 33(4), 377-380. https://doi.org/10.1016/j.gaceta.2018.04.008 [ Links ]
Orgambídez, A., Pérez, P., & Borrego, Y. (2015). Estrés de rol y satisfacción laboral: examinando el papel mediador del engagement en el trabajo. Journal of Work and Organizational Psychology, 31(2), 69-77. https://doi.org/10.1016/j.rpto.2015.04.001 [ Links ]
Peiró, J. & Rodríguez, I. (2008). Estrés laboral, liderazgo y salud organizacional. Papeles del Psicólogo, 29(1), 68-82. [ Links ]
Pereyra, F. & Micha, A. (2016). La configuración de las condiciones laborales de la enfermería en el Área Metropolitana de Buenos Aires: un análisis en el cruce del orden de género y la organización del sistema de salud. Salud Colectiva, 12(2), 221-238. https://doi.org/10.18294/sc.2016.730 [ Links ]
Perilla, L. & Gómez, V. (2017). Relación del estilo de liderazgo transformacional con la salud y el bienestar del empleado: el rol mediador de la confianza en el líder. Journal of Work and Organizational Psychology, 33(2), 95-108 https://doi.org/10.1016/j.rpto.2017.02.005 [ Links ]
Schraiber, L. B. & d’Oliveira, A. F. P. L. (2014). La perspectiva de género y los profesionales de la salud: apuntes desde la salud colectiva brasileña. Salud colectiva, 10(3), 301-312. [ Links ]
Seligman, M. E. P. (2011). Flourish: A Visionary New Understanding of Happiness and Well-Being. Simon & Schuster. [ Links ]
Setterlind, S. & Larsson, G. (1995). The stress profile: a psychosocial approach to measuring stress. Stress Medicine, 11(1), 85-92. https://doi.org/10.1002/smi.2460110116 [ Links ]
Vidal, C., Palavecino, I., Moya, P., Toro, C., Huerta, I., & Hoffmeister, L. (2017). Calidad de Vida del Personal de Salud y su Relación con el Ausentismo. Ciencia y trabajo, 19(60), 188-193. https://doi.org/10.4067/S0718-24492017000300188 [ Links ]
Villarroel, C., Busco, C., Neira, B., Ensignia, A., & Durán, P. (2018). Modelo de intervención de riesgos psicosociales en la red asistencial de salud. Revista Ciencia y Trabajo, 20(62), 76-79. https:/doi.org/10.4067/S0718-24492018000200076 [ Links ]
Ware, J. E. Jr. & Sherbourne, C. D. (1992). The MOS 36-item short-form health survey (SF-36): I. Conceptual framework and item selection. Medical care, 30(6) 473-483 [ Links ]
How to cite: Castro Méndez, N. & Suárez Cretton, X. (2022). Psychosocial risks and their relationship with occupational health in a hospital. Ciencias Psicológicas, 16(1), e-2551. https://doi.org/10.22235/cp.v16i1.2551
Authors’ participation: a) Conception and design of the work; b) Data acquisition; c) Analysis and interpretation of data; d) Writing of the manuscript; e) Critical review of the manuscript. N. C. M. has contributed in a, b, c, d, e; X. S. C. in c, d, e.
Received: April 20, 2021; Accepted: February 21, 2022
 Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
