










Serviços Personalizados
Journal

Artigo
 texto em
texto em  Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
Links relacionados
Compartilhar

 Permalink
PermalinkCiencias Psicológicas
versão On-line ISSN 1688-4221
Cienc. Psicol. vol.15 no.1 Montevideo jun. 2021 Epub 01-Jun-2021
https://doi.org/10.22235/cp.v15i1.2214
Original articles
Evidence of structure and internal consistency of the Risk Inventory Suicidal Adolescent (IRISA) in Uruguay population
1
 http://orcid.org/0000-0003-0197-6083
http://orcid.org/0000-0003-0197-6083
2
http://orcid.org/0000-0003-4121-9482
2
http://orcid.org/0000-0003-1753-4693
3
http://orcid.org/0000-0003-3874-653X
1 Universidad Católica del Uruguay amachado@ucu.edu.uy
2 Universidad Nacional de Córdoba, Argentina
3 Universidad de la República, Uruguay
4 Universidad Iberoamericana Puebla, México
Suicide rates have risen by 40 % over the last 15 years in Uruguay; 17 % of people who commit suicide in Uruguay are adolescents. Acknowledging the need for appropriate instruments to assess and manage suicidal risk among adolescents, this study evaluated some psychometric properties of the Adolescent Suicide Risk Inventory (IRISA, acronym in Spanish). The IRISA and a sociodemographic questionnaire were administered to a sample of Uruguayan adolescent students of 447 individuals, aged 12 through 18 (M=15.06; SD=1.84). The confirmatory factorial analysis concurs with the reported scales of IRISA, exhibiting adequate reliability and acceptable inter-scale correlations. Findings suggest IRISA is a valid and reliable screening test for suicidal risk in Uruguayan student adolescents and its extensive use at primary care service seems promising.
Keywords: suicide risk; adolescence; IRISA; instrumental study
Uruguay ha registrado un incremento del 40 % en los suicidios durante los últimos 15 años; el 17 % de quienes cometen estas conductas son adolescentes. Ante la importancia de contar con instrumentos adecuados para valorar y manejar el riesgo suicida en esta etapa, el presente estudio analiza algunas propiedades psicométricas del Inventario de Riesgo Suicida para Adolescentes (IRISA). A una muestra de 447 estudiantes uruguayos, con un rango de edad de entre 12 y 18 años (M=15.06; DE=1.84), se les administró un cuestionario sociodemográfico y el IRISA. El análisis factorial confirmatorio corroboró la dimensionalidad de la escala, los adecuados índices de fiabilidad y las correlaciones esperables intra-subescalas. Se concluye que el IRISA muestra propiedades psicométricas adecuadas, por lo que constituye una herramienta útil para la identificación de aquellos adolescentes en riesgo suicida y su uso extensivo en los servicios de atención primaria de la salud podría resultar prometedor.
Palabras clave: riesgo suicida; adolescencia; IRISA; estudio instrumental
Nos últimos 15 anos o Uruguai registrou um aumento de 40% nos casos de suicídio. Deste número, 17% são adolescentes. Diante da importância de contar com instrumentos adequados para avaliar e prevenir o risco de suicídio nesta etapa, o presente estudo analisa algumas propriedades psicométricas do Inventário de Risco Suicida para Adolescentes (IRISA). Em uma amostra de 447 adolescentes uruguaios, com uma faixa etária entre 12 e 18 anos (M=15.06; DE=1.84), foi administrado um questionário sociodemográfico e o IRISA. A análise fatorial confirmatória corroborou as dimensões da escala, os adequados índices de confiabilidade e as correlações esperadas intra subescalas. Portanto, se conclui que o IRISA conta com propriedades psicométricas adequadas para a amostra do estudo, já que representa uma ferramenta útil para a identificação daqueles adolescentes com risco de suicídio e seu uso extensivo aos serviços de atenção primária à saúde poderia resultar promissor.
Palavras-chave: risco de suicídio; adolescência; IRISA; estudo instrumental
Suicide is currently one of the most worrying public health problems worldwide. According to data from the World Health Organization (WHO, 2014), more than 800,000 people commit suicide every year in the world, which means one death every 40 seconds. Also, annually, between 10 and 20 million people attempt suicide. It is estimated that in 2020 suicide will represent 2.4 % of the total burden of disease in the world; furthermore, the suicide rate has increased in the last 50 years by approximately 60 % (WHO, 2012).
Uruguay is among the 20 nations with the highest suicide rates globally, and is the third in America according to the Pan American Health Organization (PAHO, 2014). While in Latin America the prevalence of suicides has been established at 7.3, in Uruguay it is 20.25 (Ministerio de Salud Pública (MSP), 2018). According to the MSP (2013), over the last 15 years there has been an increase of approximately 40 % in suicides in the country, which represents the death of slightly more than one person per day (2018). In response, the Ministry has implemented substantial improvements in access to universal mental health care and a National Plan for the Prevention of Suicide during the period 2011-2015, although this has not achieved the expected impact regarding the decrease in death figures by suicide.
Adolescence is a stage in which several risk behaviors commonly occur, including self-elimination attempts and consummated suicide (Sarchiapone, D'Aulerio & Iosue, 2015). Suicide is the second leading cause of death among young people between 15 and 29 years of age (WHO, 2019), and in the last 20 years it has increased by 30 % worldwide (Miron, Yu, Wilf-Miron & Kohane, 2019). If only Hispano-America is considered, Uruguay is the second country with the highest suicide rate in adolescents (Ardiles-Irrazábal, Alfaro-Robles, Díaz-Mancilla & Martínez-Guzmán, 2018). In Uruguay, approximately 42 adolescents kill themselves each year (WHO, 2018) and it is estimated that 1 in 5 deaths between 14 and 24 years of age is due to suicide (MSP, 2013), and 1 in 10 teens has attempted suicide. For this reason, the age group is defined as high risk for various manifestations of violence, including suicide (Valdéz, 2010).
Adolescent suicide presents some peculiarities that make its study difficult, compared to the adult population (Sarchiapone et al., 2015). For example, it is estimated that the data on suicidal behavior in adolescence is below its actual occurrence, since many deaths by suicide are wrongly classified as unintentional or accidental (WHO, 2014). Additionally, although the concept of death inherent to suicidal intent requires the acquired notion of irreversibility, generally already installed in this stage, it can be experienced diffusely (MSP, United Nations Population Fund (UNFPA), 2015).
Suicidal risk is conceived as a continuum that ranges from suicidal ideation -in its different manifestations, gestures and suicidal threats-, to suicide planning, self-elimination attempts and consummated suicide (PAHO, 2014). The occurrence of any of these behaviors, either sporadically or frequently, is an indicator of high risk for the person presenting it; considering that during adolescence there is a large number of risk behaviors, some of which are associated with the desire to die, for this reason, their detection and prevention are priorities.
Suicide prevention, as a public health strategy, implies not only the detection of self-elimination attempts or psychopathology associated with suicidal behavior, but also the systematization of tools that allow the early detection of suicidal risk in adolescents. These tools should mostly be applied in everyday settings where young people carry out their main activities, such as schools or primary health care services. Despite the need for instruments to assess suicide risk in Latin American youth, tests specifically created, or adapted to achieve this objective, are scarce in Latin American contexts. Although this has been attempted to be reversed in recent years, these instruments have not demonstrated appropriate levels of reliability and validity (Quinlan-Davidson, Sanhueza, Espinosa, Escamilla-Cejudo & Maddaleno, 2014). In Uruguay, most of the instruments used in the clinical context originate from other sociocultural settings, and are later translated into Spanish, without the corresponding adaptations, which leads to significant comprehension and linguistic difficulties at the time of their use (Villacieros, Bermejo, Magaña & Fernández-Quijano, 2016).
Among the instruments for assessing suicide risk in Latin American samples are: the Inventory of Suicidal Orientations ISO-30 (King & Kowalchuk, 1994, adaptation of Fernández Liporace & Casullo, 2006); the Inventory of Reasons to Live (Echavárri et al., 2018); the Positive and Negative Suicidal Ideation Inventory (Pansi; Villalobos-Galvis, 2010); the Suicide Resilience Inventory (SRI-25; validated by Villalobos-Galvis, Arévalo & Rojas, 2012), the Columbia Suicide Severity Scale (C-SSRS, 2011; adaptation of Serrani-Azcurri, 2017), Argentina of Suicidability (Galarza, Castañeiras & Fernández, 2014); the Inventory for the Recognition of Warning Signs for Suicidal Acts (IRSA; Brás, Carmo & Neves de Jesús, 2017) and the Inventory of Suicide Risk for Adolescents IRISA in its second version (Hernández-Cervantes & Lucio, 2006). After a bibliographic search, no investigations have been identified in Uruguay that evaluate its psychometric properties in assessing suicide risk in adolescents in this country.
Most of the above-mentioned instruments have placed special emphasis on individual factors associated with adolescent suicide risk. The IRISA (Hernández-Cervantes & Lucio, 2006) is an exception, since it investigates both risk and protective factors associated to teen suicide, both individual and socio-familial; it also evaluates the different components of the adolescent suicide risk process, estimating the level of suicide risk, and proposing an appropriate therapeutic plan for interventions. Finally, the IRISA also investigates specific conditions related to the academic environment, where a large part of the development of adolescents in school takes place, who are the majority in Uruguay. The IRISA was created based on two theoretical models: that of suicide in children and adolescents proposed by Shaffer and Pfeffer (2001) and that of identification and evaluation of suicide risk by Kirk (1993) (as cited in Hernández-Cervantes & Lucio, 2010). Both perspectives highlight suicide risk as a dynamic and multifactorial phenomenon, which must consider biological, genetic, sociodemographic, family and early factors, presence of mental disorders, personality and cognitive styles, adverse or stressful life events, suicidal ideation, suicide attempts previous, plans, and means to commit suicide.
The inventory, composed of 50 items, categorizes adolescent suicide risk process considering four subscales: Suicidal Ideation and Intentionality (10 items; α = .92), Depression and Hopelessness (8 items; α = .86), Absence of Protective Circumstances (6 items; α = .82) and Psychological Distress Associated with Suicidal Risk (26 items; α =.79.), and three critical items, indicators of different risk levels: Suicidal ideation; Suicidal plan (s) and previous attempt (s). The IRISA is defined as an instrument for screening and prioritization of suicide risk in adolescents.
Regarding the subscales, Suicidal Ideation and Intentionality evaluates both the degree of intentionality among self-injuring behavior and rumination about death, in terms of frequency and situations commonly present in people with a high level of suicide planning (e.g. I have a place where I would like to die). Depression and Hopelessness refers to negative cognitions and affections about the self in adolescents, about their world and their future, considering interpersonal, familial and school environments (e.g. the perception that there are no good things in his/her life). The third sub-scale, Absence of Protective Circumstances, which is the only reverse-scored subscale, describes the adolescent´s view on the lack of positive factors in his/her life, that prevent suicide risk from progressing, such as family cohesion or significant bonding to family members or other people outside the family. Finally, the Psychological Distress Associated with Suicidal Risk subscale, groups together high-risk situations, as well as warning signs that can precede the three areas described above; it is the largest subscale in terms of number of items, and addresses difficulties in different areas relevant to youth (e.g. with teachers, sleep disturbances, eating disorders, etc.). Although such difficulties are not exclusively associated with suicide risk in youngsters, when combined with the rest of the subscales, converge to categorize the suicide risk process.
In its first version (Hernández-Cervantes & Lucio, 2003), it evaluated the Mexican adolescent population in educational contexts (n = 353), and had 75 items, which were later reduced to 50, to form the second version (2006), used in the present study. Regarding their psychometric properties, they were evaluated in Mexican school-age adolescents (n = 555) (Machado, 2006) and obtained evidence of its concurrent validity with both the Beck Suicidal Ideation Scale (EBIS; González-Macip, Díaz, Ortiz, González & González, 2000) and with the Experimental Suicide Ideation Subscale of the MMPI-A (n = 221) (Lucio, Loza & Duran, 2000). In addition, it presented a high internal consistency (α = .95) and a percentage of explained variance (57.6 %).
Regarding other replication studies that evaluate the psychometric properties of IRISA, we only found one investigation, carried out in Colombia (n = 526), with an abbreviated Version of 24 items, the results of which point to the inventory as adequate to evaluate adolescents in this context (Alarcón- Vásquez et al., 2019; Bahamón & Alarcón-Vásquez, 2018). The IRISA showed good consistency at the global level (α = .962), and in the subscales, high levels of reliability that vary in each one from .798 to .966. The confirmatory factor analysis yielded acceptable levels of fit and goodness. Convergent validity was also identified with the Bahamón and Alarcón-Vásquez (2018) Suicide Risk Assessment Scale (ERS). It has also been used in a normative Paraguayan sample (Coppari et al., 2009), and a Spanish clinic, a carrier of adjustment disorder (Ferrer & Kirchner, 2014), although in none of these studies were adaptations of the inventory made.
The present study aims to assess the content-based validity, validity based on internal structure and internal consistency of the IRISA in a sample of adolescents attending secondary schools in five departments of Uruguay.
Method
Participants
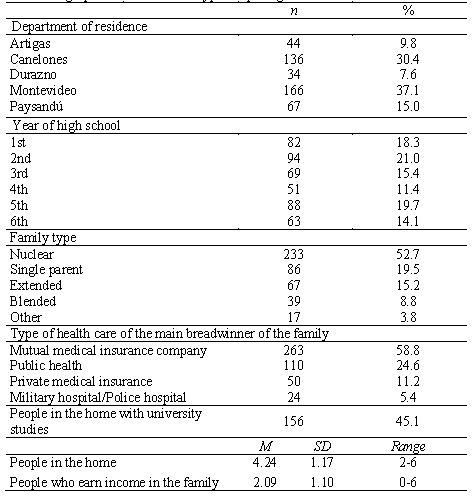
The sample consisted of 447 students (58.16 % women) between 12 and 18 years old (M=15.06, SD = 1.84), without significant differences between the sexes according to age, t (397.6) = - .432, p = .666. The distribution by courses did not show differences according to sex either, ꭕ2 (5, N = 447) = 2.02, p=.846. The adolescents belonged to educational centers corresponding to five different departments: Montevideo, Canelones, Durazno, Paysandú and Artigas. The first two departments were chosen because they have the highest concentration of population and educational centers, and the other three because they are all located in different regional areas of the country. There was an effect of sex in the distribution by departments ꭕ2 (4, N=447) = 11.56, p =.021, with a higher proportion of men than women in Montevideo (42.2 % vs 33.5 %) and Artigas (12.3 % and 8.1 %), and vice versa in the rest of the departments. Descriptive data on the characteristics of the sample are presented in Table 1.
Variables and instruments
Sociodemographic characteristics. An ad hoc sociodemographic file was used to evaluate some indicators: department of residence, year of high school, type of family, type of health care of the main breadwinner of the family, people in the home, people in the home with university studies and people who earn income in the family.
Suicidal risk: this variable was evaluated with the Suicide Risk Inventory for Adolescents (IRISA; Hernández-Cervantes & Lucio, 2006). The instrument is made up of 50 items that are answered with a five-point Likert-type response format, as 1 (Yes, all the time) to 5 (No, never). The estimated administration time is approximately 20 minutes.
As part of the present investigation, a content validity analysis of the instrument was performed in its second version, with non-quantitative methodology. For this, the original instrument was administered to a group of 12 adolescents of three age ranges: 12-13, 14-15 and 16-18 of both sexes, students from two educational centers of different socioeconomic status (high and low). In each rank, the participation of a male adolescent and a female adolescent was considered, so that together, in both secondary schools, meetings were organized with 6 adolescents, all of them in charge of psychologists. The adolescents considered that 46 of the 50 items had a high level of clarity and understanding. In the remaining 4 items, there were minor modification suggestions: in 3 of them, these were linked to the use of the terms school and teachers, which were replaced by high school and high school teachers, respectively. A single item was considered with greater difficulty to achieve a conceptual equivalence (10. The subject of death (my own death, that of others, etc.) has caught my attention) based on the suggestions made in the interviews, being modified to: 10. I have often thought about death (my own death, that of others, etc.). The final version of the cross-culturally adapted inventory consists of 46 items identical to the version used in Mexico, plus the 4 that were modified, only one of them of more relevant content, for a total of 50. The amendments were also reviewed and approved by a pair of highly trained psychologists, evaluators, experts in adolescence, with the purpose of also preserving transculturality for future research using the IRISA.
Process
The sampling was non-probabilistic, for convenience; The procedure for obtaining the sample was carried out in public and private educational institutions in Montevideo, Artigas, Canelones, Durazno and Paysandú, being made up of a total of five secondary schools. Inclusion criteria were being an adolescent and being educated in Uruguay. To carry out the administrations, authorization was requested from the directors of secondary schools, teachers and parents / guardians. Verbal informed consent was obtained from the adolescents, who voluntarily agreed to respond to the instrument. The application of the instruments was in a group setting and lasted approximately 20 minutes; was supervised by psychologists specifically trained for this task. Each participating secondary school obtained a general return of the results obtained in the risk areas evaluated by IRISA, for each class evaluated. The present study was endorsed by the Ethics Committee of the Universidad Católica del Uruguay (Resolution No. A010317).
Data analysis and design
For the descriptive analysis, tables of frequency distribution and percentages were used. Prior to the analysis of the psychometric properties of the IRISA, the mean, standard deviation, symmetry and kurtosis were calculated. For these last two indices, values between ± 1 were considered optimal, and values between ± 2 as acceptable (George & Mallery, 2016). Subsequently, the correlations between the items of each scale were analyzed in order to detect collinearity problems. Correlations lower than .85 were considered adequate (Cupani, 2012).
Internal structure. The Kaiser-Meyer-Olkin (KMO) test and Bartlett's sphericity test were performed to assess whether the data were adequate to carry out a factor analysis. In the case of the KMO test, the adequacy of the data was considered satisfactory if the values exceeded .80 and sufficient when they were between .70 and .79 (Lloret-Segura, Ferreres-Traver, Hernández-Baeza & Tomás-Marco, 2014). The Bartlett sphericity test was considered adequate if it presented a significance level of p <.05 (George & Mallery, 2016).
To evaluate the adjustment levels of the instrument, the Confirmatory Factor Analysis (CFA) was used. We chose to use the Robust Maximum Likelihood (MLR) estimation method, since it works with tetrachoric and polychoric correlations appropriate for the data that present response categories on an ordinal scale, such as those of the instrument analyzed in this study (Freiberg-Hoffmann, Stover, De la Iglesia & Fernández-Liporace, 2013). The model was specified based on the factorial structure proposed in the second version of the instrument (Hernández-Cervantes & Lucio, 2006). To evaluate the fit of the model, multiple indicators were used: the chi-square statistic (χ2), the chi-square ratio on the degrees of freedom (χ2 / gl), the comparative fit index (CFI), the Tucker-Lewis index (TLI) and the mean square error of approximation (RMSEA). The chi-square ratio on the degrees of freedom was expected to yield values less than 3.0. For the CFI and TLI indices, values between .90 and .95 were considered as indicators of an acceptable fit, and above .95 as an excellent fit. In the case of RMSEA, values between .05 and .08 were interpreted as acceptable or lower than .05 as excellent (Hair, Anderson, Tatham & Black, 2006).
Internal consistency
The internal consistency of the subscales was evaluated using two statistics: Cronbach's alpha statistic (α) and the composite reliability index (fc). Although Cronbach's alpha is one of the most used in Social Sciences (Elosua & Zumbo, 2008), it has some disadvantages when working with categorical or ordinal variables. For this reason, it was decided to use the composite reliability index in addition, which also has the advantage of considering the interrelationships of the extracted constructs when the scale is multifactorial. In both statistics used, indices above .70 are considered acceptable, while those that exceed .80 and .90 are considered good and excellent, respectively. The indices between .60 and .70 are considered moderate and it is suggested not to accept values lower than these (George & Mallery, 2016). The statistical analyzes reported were performed with the Statistical Package for the Social Sciences version 22 (SPSS) and Mplus 8 programs.
Results
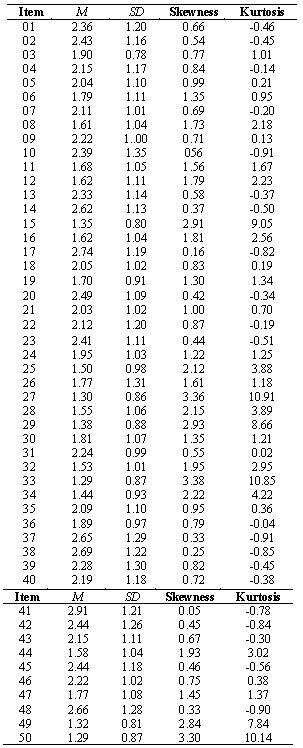
Before carrying out the confirmatory factor analysis of the instrument, the descriptive analysis of the items was carried out and the asymmetry and kurtosis indices were evaluated (see Table 2). Of the totality of items, 29 reached optimal values of symmetry (between .05 and .10), 12 showed acceptable values (between 1.22 and 1.96) and 9 showed values higher than expected (between 2.12 and 3.38) (George & Mallery, 2016). Regarding kurtosis, 29 items obtained optimal indices (between -.91 and .95), 7 reached acceptable indices (between 1.01 and 1.67) and the remaining ones showed higher indices (between 2.18 and 10.91). This did not pose a problem since the estimation method used (MLR) for the subsequent analyzes does not require compliance with the normality assumptions. The response range for all items was 1 to 5. Most items have a left response (values close to 1.5), although a significant number approaches the midpoint of the theoretical distribution (3). The IRISA correction guideline stipulates that some items must be recoded to qualify the subscales, so that higher scores in these items imply a greater risk in the adolescent.
Analysis of the factor structure
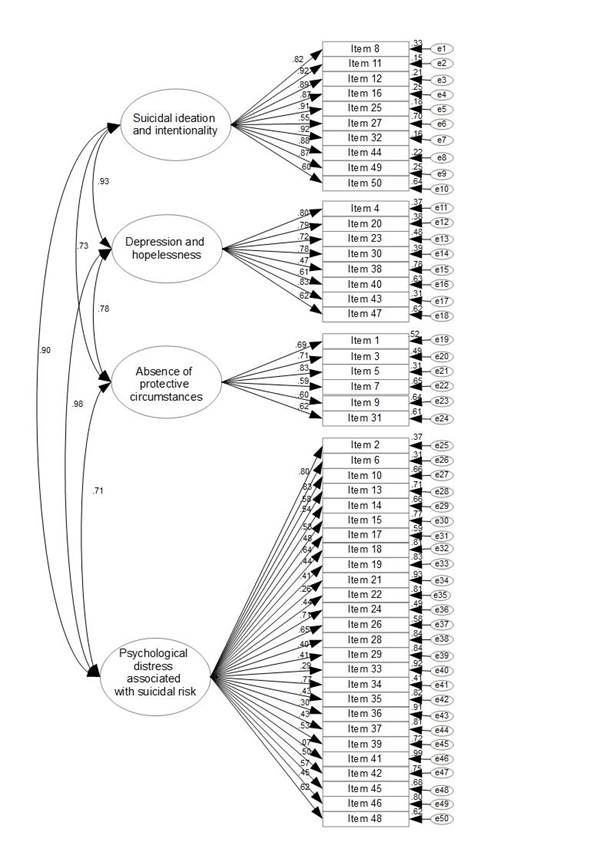
The matrix of correlations between the items indicated the absence of collinearity, since all the bivariate correlations were less than .85 (Cupani, 2012). The Bartlet sphericity indices (χ2 = 10,614.231; p <.001) and the Kaiser-Meyer-Olkin measure of sampling adequacy (KMO = .95) indicated an appropriate relationship between variables and good sample adequacy. The IRISA model presented an acceptable fit in the four indices evaluated (χ2 / gl = 2.089, CFI = .940; TLI = .937; RMSEA = .050). Regression weights were inspected, all of which were greater than .40 and significant at a level of p <.001, except for items 21, 33, 36 and 41. However, the elimination of these items did not improve the fit of the model or the reliability of the subscales, so it was decided to keep them, in order to respect the original structure of the scale and favor a cross-cultural comparison of the data obtained through it. Regarding item 41, which obtained the lowest factor load of the entire inventory, its correlation patterns with the rest of the items was analyzed, and it presented significant correlations -although low-, with 3 items of the subscale of Depression and Hopelessness subscale, 3 items of the subscale of Absence of Protective Circumstances and 11 items of subscale of Psychological Distress Associated with Suicidal Risk, to which this item belongs to. Correlations ranged between rS =. 18 and rS =. 18, being intra-subscale correlations all positive, apart from item 18.
Interfactorial correlations were statistically significant and of high magnitude, being the relationship between the subscales of Depression and hopelessness and Psychological Distress Associated with Suicidal Risk the one that showed the strongest association. In the same direction, high and moderate correlations were also identified between the IRISA factors (Figure 1 ).
Internal consistency
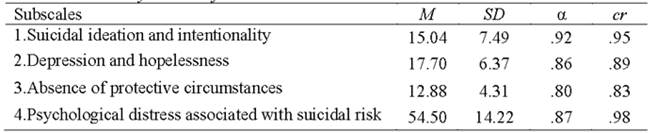
In general, the IRISA showed reliability indices between good (fc = .83) and excellent (fc =.98) for all factors (Table 3), indicating adequate general levels of internal consistency. The composite reliability indices (cr) indicated a greater internal consistency of the scale than Cronbach's alpha statistic (α = .80 - .92). The advantage of cr is to contemplate the relationships between the extracted constructs when they are correlated with each other. The correlations between the dimensions of the instrument indicate that the Suicidal Ideation and Intentionality and Depression and Hopelessness subscales show very high positive correlations. Both subscales also showed high correlations with the Psychological Distress Associated with Suicidal Risk subscale (Figure 1).
Discussion
Suicidal risk assessment constitutes a first strategic step in the detection and primary care of young people with this problem (WHO, 2018), and having validated tools for specific contexts is an essential input in this task. For this reason, the present study was oriented to analyze the psychometric properties, specifically the validity based on the content, the validity based on the internal structure and the internal consistency of the Suicidal Risk Inventory for Adolescents (IRISA; Hernández-Cervantes & Lucio, 2006) in a sample of 447 high school students from Uruguay. The IRISA is one of the few instruments specifically designed to assess suicide risk in adolescents. It has been used in samples in Mexico (Arenas-Landgrave, Lucio-Gómez & Forns, 2011; Córdova, Eguiluz & Rosales, 2011; Hernández-Cervantes & Alejandre-García, 2015; Lucio, Hernández-Cervantes & Arenas, 2012; Lucio, Plascencia-González & Zimarrón-Pérez, 2005), Colombia (Alarcón-Vásquez et al., 2019; Bahamón & Alarcón-Vásquez, 2018), Paraguay (Coppari et al., 2009) and Spain (Ferrer & Kirchner, 2014), although only two of these investigations set out to evaluate its psychometric characteristics or to carry out its adaptation / validation for other cultural contexts. The present study is the first to evaluate its psychometric properties in the Uruguayan adolescent population.
The main result of this research suggests that the IRISA (Hernández-Cervantes & Lucio, 2006) has adequate psychometric properties to evaluate the suicide risk in Uruguayan adolescents. Given that the original IRISA study in its second version (Hernández-Cervantes & Lucio, 2006) carried out an exploratory factor analysis and did not reveal the correlations between the instrument's subscales, the similarities and differences between the Colombian study and this study are discussed in detail below. (Alarcón-Vásquez et al., 2019).
Validity Based on Internal Structure: Confirmatory Factor Analysis and Relationship between Subscales
Regarding the dimensionality of the instrument, the results of the Confirmatory Factor Analysis support the original constitution of four factors obtained through an exploratory factor analysis with Mexican adolescents (Hernández-Cervantes & Lucio, 2006). In this sense, it would be aimed at confirming the hypothesis of the theoretical model that supports suicidal risk not only in indicators such as suicidal ideation, planning, and intentionality, but in their enhancers, such as depression and hopelessness (Lew et al., 2019), and the absence of protective factors (Valdivia, Silva, Sanhueza, Cova & Melipillán, 2015).
Both in the Colombian study (Alarcón-Vásquez et al., 2019) and in this study, the data indicate an appropriate level of fit to the model proposed by IRISA. While this study tested the four-factor model, according to the original instrument, the Colombian study tested a three-factor model, using a shortened version. In both studies, the review of at least one item is proposed based on the low item-subscale correlations presented. Based on the data of this study, we recommend that four items of the Psychological distress associated with suicidal risk subscale should be reviewed. We consider that one of them (21. I have difficulties with my school subjects) could be highly unspecific of suicidal risk, and present a high commonality with other prevalent difficulties in adolescence, such as school dropout or bullying (Serrano-Ruiz & Olave-Cháves, 2017). Its role as a suicide risk factor could be considered as an interesting line of future research.
The rest of reviewable items (33. If I died, I would like you to accompany me (dying with me), 36. I got rid of precious possessions for me (for example: giving away, donating, throwing away, burning) and 41. I have reconciled with people I had problems with) could be evaluating common components to the planning of the attempt, and specifically in adolescents, the fact that the results of this study show a lower desire for accompaniment / social reconciliation than what has been found for adult samples, could be emphasizing the search for autonomy so relevant throughout adolescence (Kawashima, Ito, Narishige, Saito & Okubo, 2012). Although in this study these items presented low factor loadings, and their elimination could contribute to saving administration time, we did not consider this option, giving priority to the theoretical criterion, to possible cross-cultural research aimed at comparison with other countries. We also consider that each item of the IRISA can be of practical use, since they are indicators, themselves, of emotional, cognitive, and behavioral aspects, all of them which could be integrated as focuses of the intervention plan. This highlights the clinical interest of the items, as possible main areas to include into the psychotherapy process when working with adolescents; although not all items might necessarily directly be linked to suicide risk, they might be associated with, for example, strengthening those protective factors identified by the IRISA (Hernández-Cervantes & Lucio, 2006).
Regarding the relationship between the subscales of IRISA, and as in the Colombian study (Alarcón-Vásquez et al., 2019), in this study we found the highest correlations between the subscales of Suicidal Ideation and Intentionality and Hopelessness and Depression, but the second place is invested in studies; while for the data of this study, the second closest association was between Depression and Hopelessness and Absence of Protective Circumstances, in the Colombian study, the second place was occupied by the correlation between the subscales of Suicidal Ideation and Intentionality and Absence of Protective Circumstances, although by little margin of difference.
A common striking finding is the high correlations between the subscales. This can be partially due to the estimation method used. Although the WLSMV estimator does not assume a normal distribution for the manifest variables, it can produce a moderate overestimation of correlations between factors, when the sample size is small or when latent distributions are moderately abnormal (Li, 2016). On the other hand, as proposed by Alarcón-Vásquez et al. (2019), the high correlation between factors could be explained by the existence of a more global latent or second-order construct, which raises the possibility that the subscales, primarily the Suicidal Ideation and Intentionality and Depression and Hopelessness on the one hand, and the Absence of Protective Circumstances and Psychological Distress Associated with Suicidal Risk on the other hand, are assessing very similar edges of suicide risk. The fact that the Depression / Hopelessness and Suicidal Ideation / Intentionality subscales are possibly overlapping in terms of the construct they intend to evaluate is a phenomenon described in other research on suicide risk and associated risk factors (Silva et al., 2017). This can be explained considering that most of the depression scales include items referring to the spectrum of suicidal behavior, which would end up redounding in the contribution that suicidal ideation/intentionality themselves have in the continuum that leads to suicide attempt (Beck, Kovacs & Weismann, 1976). For example, in the IRISA, the items: 30. I think or feel that the people around me would be better off without me, 23. I feel angry / frustrated, and 4. I think or feel that I am a failure, which belong to the Depression and Hopelessness subscale, point to well-documented aspects of suicidal risk, such as handicap, feelings of non-achievement, and negative emotionality (World Federation for Mental Health, 2010). Contrasting a second-order factor model would require justification, deeper theoretical discussions, and new statistical analysis. Carrying this out exceeds the objectives of this paper. Future studies may deepen on this and generate contributions in this regard.
It is worth thinking, at this point, about the semantic weight in the formulation of the items, and its clinical correlate. Following the example, the word failure does not necessarily have a unique interpretation in young people. These results should require more detailed investigations regarding the contribution of each of these adolescent suicide risk factors. Future studies could analyze its convergent validity with instruments validated also in the Uruguayan population that, for example, specifically evaluate suicidal ideation, or depression / hopelessness, such as the Beck Hopelessness Scale (Beck, Weissman, Lester & Trexler, 1974) or the Beck's Suicidal Ideation Scale (Beck, Kovacs & Weissman, 1979), considering some antecedents of its use in this context and for adolescent samples (Larrobla, Canetti, Hein, Novoa & Durán, 2012).
IRISA internal consistency: Reliability
In relation to reliability, all IRISA subscales showed high internal consistency and homogeneity, which denotes highly satisfactory reliability. The reliability of this study was tested by evaluating both Cronbach's alpha and composite reliability indices, while both in the study of the first version of IRISA (Hernández-Cervantes & Lucio, 2003), and in the Colombian study (Alarcón -Vásquez et al., 2019) exclusively analyzed Cronbach's alpha index. Both the study presented here and these two support the Suicidal Ideation and Intentionality subscale as the most consistent, considering Cronbach's alpha statistic. When considering the composite reliability statistic, the most consistent subscale was the Psychological distress associated with suicidal risk. The high indexes of internal consistency of this subscale could be due to the high number of items that compose it. Studies have shown that coefficients above 0.90 can be observed regularly on scales with more than 20 items, since the coefficient is directly affected by the number of items that make up the scale, that is, when the number of items is so high, the coefficient is overestimated (Campo-Arias & Oviedo, 2008).
One suggestion that future studies might consider is the reduction of potentially redundant items on the subscale. For these purposes, an analysis based on the Item Response Theory (IRT) would be very useful to identify those indicators with greater sensitivity in the assessment of suicide risk, and thus prevent researchers/clinicians from administering unnecessary items of the scale. It is important to consider that the inventory is constituted a screening instrument, which should aim to keep, for practical purposes, the number of items to the minimum necessary. Although the elimination of items limits the amount of information collected, having an alternative abbreviated version could be useful for contexts where saving time and resources is desirable, as in primary health care. The World Health Organization, together with the Pan American Health Organization, the Junta Nacional de Drogas and the Ministerio de Salud Pública, propose, in the II World Survey of Adolescent Health (2012), for example, the possibility of evaluating suicide risk in said population through few indicators: one referring to whether the adolescent seriously considered the possibility of taking their own life, another about whether they made a plan on how they would do it, and a last one about the number of attempts previous self-elimination in the last 12 months.
Limitations and future studies
The study has some limitations to consider. In the first place, only adolescents enrolled in school have been included as part of the sample, which would affect its representation, and therefore, the extrapolation of the conclusions to other adolescents disconnected from the educational system. It is possible that adolescents in highly vulnerable situations are overrepresented among out-of-school groups. In fact, previous geographically close studies show that approximately half of adolescents admitted to juvenile justice systems did not attend school prior to admission (Bobbio, 2019). Likewise, suicidal behavior in this population has been shown to be significantly higher than that of adolescents from the general population (Gallagher & Dobrin, 2006). Therefore, future studies in this population of institutionalized adolescents would be of great interest by providing evidence that allows improving the detection of suicide risk in this population.
Second, we consider it advisable to carefully analyze the results, since the sample was obtained for convenience and is not representative of all Uruguayan adolescents. Finally, social desirability was not evaluated, so its effects on the responses provided by the participants cannot be ruled out.
Future studies could make an important contribution by contrasting the validity of the instrument in other populations that may present an increased risk of suicidal behavior, such as clinical (Barros et al., 2016) and forensic populations (Ford, Hartman & Chapman, 2008). Concurrent validity studies, with other measures empirically associated with suicide risk, such as depression or hopelessness or other brief suicide risk scales, are pending for a future study. In turn, future studies should delve into the discriminant capacity of each subscale, as well as review in more detail the behavior of the items that had little contribution to their subscales. Furthermore, to carry out comparative studies with Mexican and Colombian samples, attention should be paid not only to the contrast of the scores obtained in the instrument, but to the prevalent suicide rate in each country. In other words, it would be expected that in countries with higher baseline rates of this behavior, the scores in the general population would be higher.
Finally, it would be advisable to include other variables of proven interest in suicidal behavior, such as age (early, middle and late teens) and/or sex. In addition, , it would be advisable to carry out clinical interviews with part of the sample, to identify true positives for suicide risk, by trained clinicians and add to the predictive validity of the instrument.
Research implications
Despite its limitations, the study shows solidity in some psychometric characteristics evaluated by the IRISA, which should be further studied and consolidated through future research. This will allow for comparative studies with other countries, for example between Mexican, Colombian and Uruguayan samples, considering that the inventory behaves in a similar way in the three cultural contexts. In addition, this represents one of the first works to study suicide risk in adolescents in Uruguay and the only one that has had as its objective the adaptation of a valid and reliable instrument for the evaluation of the phenomenon.
Regarding the theoretical implications, this study points out that both depressive disorders and hopelessness are consistently and more prevalently associated with adolescent suicidal risk. Depression is more strongly associated with adolescent suicide risk than with adult suicide (Gould, Greenberg, Velting & Shaffer, 2003), so its evaluation as an independent dimension of suicide risk itself is likely to be difficult. Regarding other relevant indicators in adolescent suicidal risk, specifically those that obtained the lowest weight in this study, it could be thought that they evaluate a risk dimension associated with the social sphere (desire to be accompanied in the suicidal act, or reconciliation with people important prior to suicide); adolescent suicide occurs mainly in the context of the search for autonomy and social conflicts (family and peer), so it could be seen as a search for bond break/distancing (Kawashima et al., 2012). Furthermore, the suicidal planning investigated in the indicators of lower weight in this study points to a highly elaborated level of anticipation; in adolescents, suicide risk has been commonly linked to impulsivity, compared to what occurs in adults (Reyna & Farley, 2006).
Regarding the practical implications, we highlight the importance of having a specific suicide risk assessment instrument for the adolescent population, both in primary health care services and in educational contexts. The IRISA has been proposed as a screening inventory, and as such it should have the advantage of being short, easy to understand, and quick to apply. The findings of this study suggest the possibility of abbreviating the technique even further, as has already been done in other research (Alarcón-Vásquez et al., 2019); that is, we propose the possibility of administering it as a screening technique to assess adolescent suicidal risk in contexts with a large flow of casuistry and that require rapid evaluations, such as primary health care services, and the full version in clinical care contexts specific to this problem, and to be complemented with other measures of variables of interest (such as personality, self-regulation, impulsivity, risk behaviors, etc.).
Conclusions
The present research allows us to conclude that in Uruguayan adolescents the Suicide Risk Inventory has a good internal structure and high consistency, and, therefore, the results of this study provide evidence on some of its psychometric properties and its adequacy in the detection of suicidal risk in this population. However, future studies that delve into other psychometric characteristics of the instrument, such as its concurrent and predictive validity, as well as the possibility of having a more abbreviated version of it, would be very beneficial, both for its application in the field of research. as in the clinical context.
REFERENCES
Alarcón-Vásquez, Y., Bahamón, M., Trejos-Herrera, A. M., González-Gutiérrez, O., Rubio-Castro, R., Hernández-Cervantes, Q. et al. (2019). Análisis de las Propiedades Psicométricas del Inventario de Riesgo Suicida (IRISA) para Adolescentes Colombianos. Revista Iberoamericana de Diagnóstico y Evaluación - e Avaliação Psicológica, 51(2), 87-98. [ Links ]
Ardiles-Irarrázabal, R. A., Alfaro-Robles, P. A., Díaz-Mancilla, I. E. & Martínez-Guzmán, V. V. (2018). Riesgo de suicidio adolescente en localidades urbanas y rurales por género, región de Coquimbo, Chile. Aquichan, 18(2), 160-170. [ Links ]
Arenas-Landgrave, P., Lucio-Gómez, E. & Forns, M. (2011). Indicadores diferenciales de personalidad frente al riesgo de suicidio en adolescentes. RIDEP, 2(32), 79- Bahamón 104. [ Links ]
Bahamón, M. J. & Alarcón-Vásquez, Y. (2018). Diseño y validación de una escala para evaluar el Riesgo Suicida (ERS) en adolescentes colombianos. Universitas Psychologica, 17(4), 1-15. [ Links ]
Barros, J., Morales, S., Echávarri, O., García, A., Ortega, J., Asahi, T., et al. (2016). Suicide detection in Chile: proposing a predictive model for suicide risk in a clinical sample of patients with mood disorders. Brazilian Journal of Psychiatry, 39(1), 1-11. [ Links ]
Beck, A. T., Kovacs, M. & Weissman, A. (1976). Hopelessness and suicidal behavior, JAMA, 234, 1146-1149. [ Links ]
Beck, A. T., Kovacs, M. & Weissman, A. (1979). Assessment of suicidal ideation. The scale for Suicide Ideation. Journal of Consulting Clinical Psychology, 47(2), 343-352. [ Links ]
Beck, A. T., Weissman, A., Lester, D. & Trexler, L. (1974). The measurement of pessimism: The Hopelessness Scale. Journal of Consulting and Clinical Psychology, 42(6), 861-865. [ Links ]
Bobbio, A. (2019). Conducta antisocial adolescente: Un contraste empírico de teorías criminológicas. (Disertación doctoral). Universidad Nacional de Córdoba, Argentina. [ Links ]
Brás, M., Carmo, C. & Neves de Jesus, S. (2017). Estudo das propriedades psicométricas do Inventário de Reconhecimento de Sinais de Alerta para Atos Suicidas. Revista Iberoamericana de Diagnóstico y Evaluación - e Avaliação Psicológica, 1(43), 89-105. [ Links ]
Campo-Arias, A. & Oviedo, H. C. (2008). Propiedades psicométricas de una escala: la consistencia interna. Revista de salud pública, 10, 831-839. [ Links ]
Coppari, N., Alonso, R., Fernández, E., Iturry, V., Kriskovich, R. & Mernes, R. (2009). Adolescencia prevenida: diferencias en indicadores de riesgo en adolescentes chaqueños medidas a través del IRIS. Eureka, 6(1), 58-75. [ Links ]
Córdova, M., Eguiluz, L. & Rosales, J. (2011). Pensamientos suicidas en estudiantes universitarios del estado de Tlaxcala (México). Enseñanza e investigación en psicología, 16(1), 155-164. [ Links ]
Cupani, M. (2012). Análisis de ecuaciones estructurales: Conceptos, etapas de desarrollo y un ejemplo de aplicación. Revista Tesis, 1, 186-199. [ Links ]
Echávarri, O., Morales, S., Barros, J., Armijo, I., Larraza, D., Longo, A., et al. (2018). Validación de la Escala Razones Para Vivir en Consultantes a Salud Mental de la Región Metropolitana de Chile. Psykhe, 27(2), 1-17. [ Links ]
Elosua, P. & Zumbo, B. D. (2008). Coeficientes de fiabilidad para escalas de respuesta categórica ordenada. Psichothema, 20(4), 896-901. [ Links ]
Federación Mundial de la Salud Mental. (2010). Enfermedad mental y suicidio. Guía para la familia para encarar y reducir riesgos. Woodbridge, VA: World Federation for Mental Health. [ Links ]
Fernández-Liporace, M. & Casullo, M. M. (2006). Validación factorial de una escala para evaluar riesgo suicida. Revista Iberoamericana de Diagnóstico y Evaluación Psicológica, 21(1), 9-22. [ Links ]
Ferrer, L. & Kirchner, T. (2014). Suicidal tendency in a sample of adolescent outpatients with Adjustment Disorder: Gender differences. Comprehensive Psychiatry, 55, 1342-1349. [ Links ]
Ford, J. D., Hartman, J. K., Hawke, J. & Chapman, J. F. (2008). Traumatic victimization, posttraumatic stress disorder, suicidal ideation, and substance abuse risk among juvenile justice-involved youth. Journal of Child & Adolescent Trauma, 1(1), 75-92. [ Links ]
Freiberg-Hoffmann, A., Stover, J. B., de la Iglesia, G. & Fernández-Liporace, M. (2013). Correlaciones policóricas y tetracóricas en estudios factoriales exploratorios y confirmatorios. Ciencias Psicológicas, 7(2), 151-164. [ Links ]
Galarza, A., Castañeiras, C. & Fernández, M. (2014). Construcción y estudio de calidad psicométrica de la Escala Argentina de Suicidabilidad para Adolescentes (EASA). Anuario de Proyectos e Informes de Becarios de Investigación, 11, 1009-1016. [ Links ]
Gallagher, C. A. & Dobrin, A. (2006). Deaths in juvenile justice residential facilities. Journal of Adolescent Health, 38(6), 662-668. [ Links ]
George, D. & Mallery, P. (2016). IBM SPSS statistics 23 step by step: A simple guide and reference. Recuperado de https://books.google.co.kr/books?hl=en&lr= &id=vKLOCwAAQBAJ&oi=fnd&pg=PP1&dq=D.+George,+P.+Mallery,+IBM+SPSS+ Statistics+23+Step+by+Step:+A+Simple+Guide+and+Reference,+Routledge,+ [ Links ]
González-Macip, S., Díaz, A., Ortiz, S., González, C. & González, J. J. (2000). Características psicométricas de la Escala de Ideación Suicida de Beck (ISB) en estudiantes universitarios de la ciudad de México, Salud Mental, 23(2), 21-30. [ Links ]
Gould, M. S., Greenberg, T., Velting, D. M. & Shaffer, D. (2003). Youth suicide risk and preventive interventions: a review of the past 10 years. Journal of the American Academy of Child & Adolescent Psychiatry, 42(4), 386-405. [ Links ]
Hair, J. F., Anderson, R. E., Tatham, R. L. & Black, W. (2006). Análisis multivariante (6a. ed.). Madrid, España: Pearson Education. [ Links ]
Hernández-Cervantes, Q. & Alejandre-García, J. (2015). Relación entre riesgo suicida y uso de tabaco o alcohol en una muestra de universitarios. Acta universitaria, 25(2), 47-51. [ Links ]
Hernández-Cervantes, Q. & Lucio, E. (2003). Inventario de riesgo suicida para adolescentes IRIS, primera versión. Reporte del examen de postulación al doctorado, Facultad de Psicología, Universidad Nacional Autónoma de México, México. [ Links ]
Hernández-Cervantes, Q. & Lucio, E. (2006). Evaluación del riesgo suicida y estrés asociado en adolescentes estudiantes mexicanos. Revista Mexicana de Psicología, 23(1), 45-52. [ Links ]
Hernández-Cervantes, Q. & Lucio, E. (2010). Modelo de evaluación del riesgo suicida adolescente basado en la exposición a eventos estresantes y configuraciones de personalidad. Recuperado de https://www.researchgate.net/publication/291523665 [ Links ]
Kawashima, Y., Ito, T., Narishige, R., Saito, T. & Okubo, Y. (2012). The characteristics of serious suicide attempters in Japanese adolescents - comparison study between adolescents and adults. BMC Psychiatry, 12, 191-198. [ Links ]
King, J. D. & Kowalchuk, B. (1994). ISO-30. Adolescent Inventory of Suicide Orientation-30. Minneapolis: National Computer Systems. [ Links ]
Larrobla, C., Canetti, A., Hein, P., Novoa, G. & Durán, M. (2012). Prevención de la conducta suicida en adolescentes: Guía para los sectores Educación y Salud. Montevideo: Udelar-CSIC. [ Links ]
Lew, B., Huen, J., Yu, P., Yuan, L., Wang, D.F., Ping, F., et al. (2019). Associations between depression, anxiety, stress, hopelessness, subjective well-being, coping styles and suicide in Chinese university students. PLoS ONE, 14(7), 1-10. [ Links ]
Li, CH. (2016). Confirmatory factor analysis with ordinal data: Comparing robust maximum likelihood and diagonally weighted least squares. Behav Res Methods, 48(3), 936-49. doi: https://doi.org/10.3758/s13428-015-0619-7. [ Links ]
Lloret-Segura, S., Ferreres-Traver, A., Hernández-Baeza, A. & Tomás-Marco, I. (2014). El análisis factorial exploratorio de los ítems: Una guía práctica, revisada y actualizada. Anales de Psicología, 30(3), 1151-1169. doi: https://doi.org/10.6018/analesps.30.3.199361 [ Links ]
Lucio, E., Hernández-Cervantes, Q. & Arenas, P. (2012). Modelo de tamizaje para uso de sustancias y riesgo suicida en estudiantes de bachillerato: resultados preliminares. En L. M. Reidl, Desarrollo de nuevos modelos para la prevención y el tratamiento de conductas adictivas. Seminarios académicos (pp.133-146). México DF: Porrúa / UNAM. [ Links ]
Lucio, E., Loza, C. G. & Durán, P. C. (2000). Los sucesos de vida estresantes y la personalidad de los adolescentes con intento suicida. Revista de Psicología Contemporánea, 7(2), 58-65. [ Links ]
Lucio, E., Plascencia-González, M. & Zamarrón-Pérez, G. (2005). Detección del riesgo suicida y otros problemas emocionales en una muestra de adolescentes de Aguascalientes. Investigación y Ciencia, 13(32), 29-36. [ Links ]
Machado, A. I. (2006). Detección de riesgo suicida en una secundaria pública del Distrito Federal. (Tesis de licenciatura inédita). Facultad de Psicología, Universidad Nacional Autónoma de México, México . [ Links ]
Ministerio de Salud Pública, Fondo de Población de Naciones Unidas. (2015). Aportes para el abordaje de la salud de adolescentes en el Primer Nivel. Recuperado de http://www.msp.gub.uy/sites/default/files/archivos_adjuntos/Publicacion%20Adolescentes.pdf [ Links ]
Ministerio de Salud Pública. (2013, julio). Suicidio en adolescentes y jóvenes de 10 a 24 años en Uruguay, 2009. Programa Nacional de Salud Mental, Programa Nacional de Salud de Adolescencia y Juventud. Documento presentado en el Día Nacional de Prevención del Suicidio, Montevideo, Uruguay. [ Links ]
Ministerio de Salud Pública. (2018). Índice de suicidios se mantuvo estable en 2018, 20,25 por cada 100.000 habitantes. Recuperado de https://www.gub.uy/ministerio-salud-publica/comunicacion/noticias/indice-suicidios-se-mantuvo-estable-2018-2025-cada-100000-habitantes [ Links ]
Miron, O., Yu, K. H., Wilf-Miron, R. & Kohane, I. S. (2019). Suicide rates among adolescents and young adults in the United States, 2000-1017. JAMA, 321(23), 2362-2364. [ Links ]
Organización Mundial de la Salud. (2012). Prevención de suicidio. Recuperado de http://www.who.int/ mediacentre/news/releases. [ Links ]
Organización Mundial de la Salud. (2014). Primer informe de la OMS sobre prevención del Suicidio. Recuperado de https://www.who.int/mediacentre/news/releases/2014/suicide-prevention-report/es/ [ Links ]
Organización Mundial de la Salud. (2018). Suicide rate estimates, age-standardized: Estimates by country. Recuperado de https://apps.who.int/gho/data/node.main.MHSUICIDEASDR?lang=en [ Links ]
Organización Mundial de la Salud. (2018). Suicidio. Recuperado de https://www.who.int/es/news-room/fact-sheets/detail/suicide [ Links ]
Organización Mundial de la Salud. (2019). Suicidio: datos y cifras. Recuperado de https://www.who.int/es/news-room/fact-sheets/detail/suicide [ Links ]
Organización Panamericana de la Salud, Organización Mundial de la Salud, Junta Nacional de Drogas, Ministerio de Salud Pública & Ministerio de Desarrollo Social. (2012). Adolescencias, un mundo de preguntas - II Encuesta Mundial de Salud Adolescente GSHS 2012. Montevideo: OPS, JND, MSP y Mides. [ Links ]
Organización Panamericana de la Salud. (2014). Mortalidad por suicidio en las Américas: Informe regional. Washington DC: OPS. [ Links ]
Quinlan-Davidson, M., Sanhueza, A., Espinosa, I., Escamilla-Cejudo, J.A. & Maddaleno, M. (2014). Suicide among young people in the Americas. Journal of Adolescent Health, 54(3), 262-268. [ Links ]
Reyna, V. & Farley, F. (2006). Risk and rationality in adolescent decision-making: implications for theory, practice, and public policy. Psychological Science in the Public Interest, 7(1), 1-44. [ Links ]
Sarchiapone, M., D’Aulerio, M. & Iosue, M. (2015). Suicidal ideation, suicide attempts and completed suicide in adolescents: Neuro-biological aspects. Biological Aspects of Suicidal Behavior, 30, 11-20. [ Links ]
Serrani-Azcurri, D. (2017). Psychometric validation of the Columbia-Suicide Severity rating scale in Spanish-speaking adolescents. Colombia Médica, 48(4), 174-182. [ Links ]
Serrano-Ruiz, C. & Olave-Cháves, J. (2017). Factores de riesgo asociados con la aparición de conductas suicidas en adolescentes. Med UNAB, 20(2), 139-147. [ Links ]
Shaffer, D. & Pfeffer, C. R. (2001). Practice parameter for the assessment and treatment of children and adolescents with suicidal behavior. Journal of the American Academy of Child & Adolescent Psychiatry, 40(Supl. 7), 24S-51S. [ Links ]
Silva, D., Valdivia, M., Vicente, B., Arévalo, E., Dapelo, R. & Soto, C. (2017). Intento de suicidio y factores de riesgo en una muestra de adolescentes escolarizados en Chile. Revista de Psicopatología y Psicología Clínica, 22, 33-42. [ Links ]
Valdéz, L. (2010). Prestaciones Psicoterapéuticas, Adultos y niños, adolescentes y jóvenes. Uruguay: MSP, PNSM. [ Links ]
Valdivia, M., Silva, D., Sanhueza, F., Cova, F. & Melipillán, F. (2015). Prevalencia de intento de suicidio adolescente y factores de riesgo asociados en una comuna rural de la provincia de Concepción. Revista Médica de Chile, 143(3), 320-328. [ Links ]
Villacieros, M., Bermejo, J., Magaña, M. & Fernández-Quijano, I. (2016). Psychometric properties of the Attitudinal Beliefs Questionnaire about suicidal behavior (CCCS-18). The Spanish Journal of Psychology, 19, E68. doi: doi.org/10.10 17/sjp.2016.68 [ Links ]
Villalobos-Galvis, F. H. (2010). Validez y fiabilidad del Inventario de Ideación Suicida Positiva y Negativa-PANSI, en estudiantes colombianos. Universitas Psychologica, 9(2), 509-520. [ Links ]
Villalobos-Galvis, F. H., Arévalo Ojeda, C. & Rojas Rivera, F. D. (2012). Adaptación del Inventario de Resiliencia ante el Suicidio (SRI-25) en adolescentes y jóvenes de Colombia. Revista Panamericana de Salud Pública, 31(3), 233-239. [ Links ]
Funding: This research was carried out thanks to the funding of National Postgraduate Scholarships projects from the National Research and Innovation Agency (ANII).
Correspondencia: Ana Inés Machado. Departamento de Psicología Clínica y de la Salud, Facultad de Ciencias de la Salud, Universidad Católica del Uruguay. E-mail: amachado@ucu.edu.uy
How to cite: Machado, A. I., Bobbio, A., Arbach, K., Parra, A., Riestra, C. & Hernández-Cervantes, Q. (2021). Evidence of structure and internal consistency of the Risk Inventory Suicidal Adolescent (IRISA) in Uruguay population. Ciencias Psicológicas, 15(1), e-2214. doi: https://doi.org/10.22235/cp.v15i1.2214
Authors' participation: a) Concepción y diseño del trabajo; b) Adquisición de datos; c) Análisis e interpretación de datos; d) Redacción del manuscrito; e) revisión crítica del manuscrito. A. I. M. has contributed in a, b, c, d, e; A. B. has contributed in c, d, e; K. A. has contributed in c, d, e; A. P. has contributed in b, c, d, e; C. R. has contributed in d, e; Q. H. C. has contributed in d, e.
Received: July 14, 2020; Accepted: March 22, 2021
 Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
