










Servicios Personalizados
Revista

Articulo
 texto en
texto en  Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
Links relacionados
Compartir

 Permalink
PermalinkCiencias Psicológicas
versión impresa ISSN 1688-4094versión On-line ISSN 1688-4221
Cienc. Psicol. vol.14 no.2 Montevideo 2020 Epub 16-Ago-2020
https://doi.org/10.22235/cp.v14i2.2263
Original artícles
Personal and contextual developmental assets predictors of health perception in adolescence

1 Faculdade de Psicologia e de Ciências da Educação, Universidade do Porto. Portugal
2 Universidade Fernando Pessoa, Porto. Portugal
Self-Rated Health is the product of the interaction between personal characteristics and contextual conditions. It reflects the resources of the person, and it consists in a dynamic evaluation, i.e., a personal judgment that reflects both a point-in-time status and a developmental process. The Developmental Assets® framework provides a holistic approach in to the understanding of development, which focuses on resources that can be explored both at individual and contextual levels, in order to foster a healthy development. The purpose of this research is to explore the relationship between adolescents’ Perception of Health and their experience of Developmental Assets. A convenience sample of 503 Portuguese students was evaluated, mean age of 16 years (SD = 1.2), 63% of female gender. Results indicate that better Health Perception is associated with greater experience of Developmental Assets. Results suggest the impact of a subset of Developmental Assets on Health prediction, with Internal Assets being the strongest predictors. Results suggest the theoretical and practical utility of the Developmental Assets® framework for the understanding of Health Perception in adolescents.
Keywords: Self-Rated Health; Developmental Assets; Positive Youth Development; Healthy Development
A Perceção de Saúde é o produto da interação entre características pessoais e condições contextuais. Esta reflete os recursos da pessoa, assim como consiste numa avaliação dinâmica, um julgamento que reflete estado e processo de desenvolvimento. O Modelo de Recursos do Desenvolvimento - Developmental Assets® - proporciona uma abordagem holística na compreensão do desenvolvimento, foco em Recursos que podem ser explorados quer ao nível individual, quer contextual de modo a propiciar aos adolescentes um desenvolvimento saudável. O objetivo do presente estudo consiste em explorar a relação entre a Perceção de Saúde e a experiência de Recursos do Desenvolvimento. Foi avaliada uma amostra de conveniência constituída por 503 estudantes portugueses, com idades compreendidas entre os 13 e 19 anos (M = 16; DP = 1,2), maioritariamente do género feminino (63%). Os resultados indicam que melhor Perceção de Saúde está associada a maior experiência de Recursos do Desenvolvimento. Os dados sugerem o impacto de um subconjunto de Recursos na predição de Saúde, constituindo os Recursos Internos os preditores mais fortes. Sugere-se a utilidade teórica e prática da utilização do Modelo de Recursos do Desenvolvimento para a compreensão da Perceção de Saúde em adolescentes.
Palavras-chave: Perceção de Saúde; Recursos do Desenvolvimento; Perspetiva do Desenvolvimento Positivo na Adolescência; Desenvolvimento Saudável
La Percepción de Salud es el producto de la interacción entre características personales y condiciones contextuales. Esto refleja los recursos de la persona, así como consiste en una evaluación dinámica, un juicio que refleja el estado y el proceso de desarrollo. El Modelo de Recursos del Desarrollo - Developmental Assets® - proporciona un enfoque holístico en la comprensión del desarrollo, foco en Recursos que pueden ser explorados tanto a nivel individual, como contextual para propiciar a los adolescentes un desarrollo saludable. El objetivo del presente estudio consiste en explorar la relación entre la Percepción de Salud y la experiencia de Recursos del Desarrollo. Se evaluó una muestra de conveniencia constituida por 503 estudiantes portugueses, con edades comprendidas entre los 13 y 19 años (M = 16, DE = 1.2), mayoritariamente del género femenino (63%). Los resultados indican que la mejor percepción de la salud está asociada a la mayor experiencia de recursos del desarrollo. Los datos sugieren el impacto de un subconjunto de Recursos en la predicción de Salud, constituyendo los Recursos Internos los predictores más fuertes. Se sugiere la utilidad teórica y práctica de la utilización del Modelo de Recursos del Desarrollo para la comprensión de la Percepción de Salud en adolescentes.
Palabras clave: Percepción de Salud; Recursos del Desarrollo; Perspectiva del Desarrollo Positivo en la Adolescencia; Desarrollo Saludable
In general, how would you rate your health? - poor, fair, very good or excellent? This simple question frequently labelled Perceived Health, is also commonly named Self-Rated Health, Subjective Health, or Self-Assessed Health (Benyamini, 2011a, 2011b), being used in numerous studies. It is, for example, used in Eurostat to assess the health of Europeans (Eurostat, 2020).
People’s subjective perceptions of health capture physical, psychological, and social factors, in line with the holistic view of health conceptualized in the biopsychosocial model, as well as the WHO (1948) definition of health as a state of complete physical, mental, and social well-being and not merely the absence of disease or infirmity (Benyamini, 2008, 2011a; Pais-Ribeiro, 2005). In adolescents, subjective perceptions of health capture this holistic view of health (Joffer, Jerdén, Öhman, & Flacking, 2016). Research indicates that subjective perceptions of global health seem to go beyond a medical model of health conceived as the absence of disease, thus covering the entire illness-wellness continuum (Bishop & Yardley, 2010), and they also provide comprehensive summaries of the sets of factors that people view as part of their own concept of health (Benyamini, 2008; 2011a; Pais-Ribeiro, 2005).
Research has shown that Self-Rated Health (henceforth, SRH) is associated with diseases and symptoms, functional ability, health care utilization, medication use, mental health, social support and socioeconomic factors, suggesting that they are strongly affected by positive affect and not only by disease, disability, and negative affect (Benyamini, 2008; Benyamini, Idler, Leventhal, & Leventhal, 2000; Pais-Ribeiro, 2005; Pinquart, 2001). Research also indicates that subjective perception of health is not only related to several health measures, but it is also a better predictor of longevity than medical records or disease descriptions (Benyamini & Idler, 1999; Doiron, Fiebig, Johar, & Suziedelyte, 2015; Idler & Benyamini,1997; Jylhä, 2009). Such research results in the investigation indicate the validity of subjective perceptions of health, which makes them to be considered currently as a “proxy” measure for health, instead of more detailed health measures (Benyamini, 2008). In sum, as Benyamini (2011a, p. 305) explains, regarding perceptions of health, “the subjective is the objective”.
Benyamini (2011b, p.1410) emphasizes that the validity of SRH as a predictor of future health outcomes is based on four explanations: 1) it is more inclusive than the covariates used in many studies; 2) it is a dynamic evaluation, which reflects the judgment regarding the trajectory of health and not only current health, that is, at a defined point in time - also called “trajectory hypothesis”; 3) it influences behaviors that subsequently affect health status; and 4) it reflects the person’s resources that reflect or even affect the ability to cope with health threats.
Thus, investigation indicates that SRH reflects the person’s resources and is related both to external resources, such as social support, as well as internal resources, such as optimism, and perceived restraint (Benyamini, 2011a, 2011b; Benyamini, Blumstein, Murad, & Lerner-Geva, 2011). The inclusion of these resources often reduces the contribution of SRH for the prediction of future health, although it is difficult to tell whether this happens, because such resources, particularly the internal ones, reflect health status or because they have a causal effect on future health (Benyamini, 2011b). Benyamini (2011b) explains that personal resources, external and internal, constitute factors that can lead to different trajectories of future health.
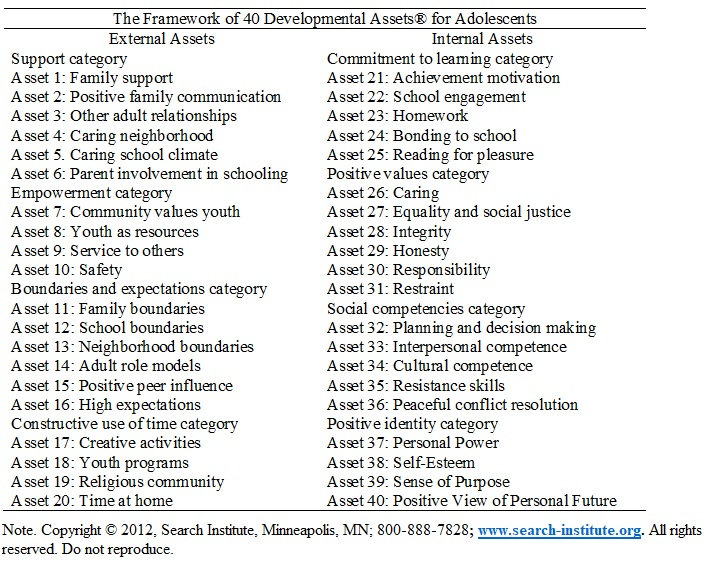
Perceptions of health and illness are embedded within personal and cultural contexts, so they are part of the socialization process, being, therefore, the product of an interaction between personal characteristics, intentional actions of social agents such as family, peers and educational system, as well as exposure to various conditions of the social context in which the person is immersed (Benjamin, 2011a). In this vein, within the framework of the Positive Youth Development Perspective, the concept of “Developmental Assets”® is developed by the Search Institute (Benson, 2006), with the aim of describing youth needs for a successful development (Benson, Scales, & Syvertsen, 2011). The model associates characteristics, competences, skills and personal qualities (Internal Assets) with positive ecological characteristics (External Assets®), by assuming that they are dynamically intertwined (Benson et al., 2006), which, combined, besides preventing behaviors that compromise health outcomes (Benson & Scales, 2009), favor an optimal, successful development in adolescence (Benson et al., 2006; Scales, Benson, Leffert, & Blyth, 2000; Scales et al., 2006). The Developmental Assets Model is introduced in a synthetical way in Table 1.
As it is based on Systemic Theories of Development, which involve a relational metatheory which proposes, an integral approach to human development (Ford & Lerner, 1992; Gottlieb, 1997, Gottlieb, Wahlsten, & Lickluter, 2006; Lerner & Steinberg, 2009; Overton, 2006, 2013; Overton & Müller, 2012). At the core of the Developmental Asset Model we find a potential ontogenetic plasticity that acknowledges the existence of relationships based on reciprocal interdependence among biological, individual and contextual levels of organization. The acknowledgment that the regulation of development involves person ←→ context mutually influential relations among all levels indicates, consequently, the potential of systematic change, i.e, of plasticity and diversity. This presupposes that positive human development can be promoted through the articulation of the characteristics of persons and ecologies (Benson et al., 2006), which constitutes, according to the Model, “the fusion of external (i.e., ecological) assets and internal assets” (Benson, 2007, p. 38).
From the theoretical formulations within the domain of Systemic Theories of Development, the main assumption underlying the Assets Model emerges in the following formulation: “the more assets, the better” (Benson et al., 2007, p.38). This refers to the Asset Building approach, which suggests that the larger the number of positive experiences the adolescent discloses, the greater the probability of a successful development (Benson et al., 2006; 2011). Benson et al. (2011, p.204) explain that “a Developmental Asset is an agent or characteristic of the individual or his/her developmental ecologies (…) that is related to the increased probability of positive outcomes”, which “increase additively or exponentially as the number of developmental assets increases”.
Given that SHR reflects the assets of a person, and it consists in a dynamic assessment that involves a judgment related not merely to the current health status, but a judgment that reflects the health trajectory, thus, it is an important result to be explored during adolescent development. A literature review shows that few studies explore the relation between SHR and Developmental Assets in the context of Positive Youth Development Approach (Soares et al., 2018b). Therefore, it becomes relevant to understand how each one of these important areas relates to the other, on account of its implications for the promotion of a positive development in adolescence.
It is also noteworthy that the majority of studies on the SHR was carried out by adults, highlighting that to understand health perception in specific subpopulations, namely in adolescence, is useful for the planning of interventions that aim at enhancing the knowledge related to health and to the engagement in health behaviors (Benyamini, 2011a). Besides age, interventions that aim at improving general health can be more effective if they are integrated to gender issues and to specific actions in this domain (Benyamini, 2011a; Benyamini, Leventhal, & Leventhal, 2000; Craig et al., 2018; Jerdén et al., 2011; Potrebny, 2019; Sokol et al. 2017; Vingilis et al., 2002)
The aim of the present study consists in exploring the relation between SHR and the experience of Developmental Assets; and specifically, to analyze which Internal and External Assets included in the model constitute predictors of health in adolescence.
Method
Participants
We evaluated a convenience sample that consisted of 503 students who regularly attended the educational system from 9th to 12th grade of a public school, in the northern region of Portugal, whose ages ranged from 13 to 19 (M = 16; SD = 1.2), most of them female (63%).
Health Perception
Assessed with the item General Health Perception included in the SF-36 survey (first item of the questionnaire), developed by Ware, Snow, Kosinski e Gandek (1993) and validated for Portugal by Ferreira e Santana, (2003), which inquires: “In general, how would you say your health is?”, with a five position Likert scale answer option that ranges from “1= excellent” to “5 = poor”. Low scores indicate better health perception. There are various reasons for considering the use of a single item for general health perception: the main one, in line with the research carried out by Benyamini (2008, 2011a, 2011b). Its usefulness is apparent insofar as the subjective perceptions of individuals about their own health capture physical, psychological and social factors, in accordance with a holistic view of health, besides providing comprehensive outlines of the set of factors that people consider as being part of their own health concept. Global health assessment is a measure that is broadly accepted in epidemiology (Benyamini, 2008; 2011a; 2011b; Idler & Benyamini, 1997). Since the end of the last century, European and world statistics use this indicator (Eurostat, 2020). It is also an indicator that has been integrated to health assessment questionnaires for specific diseases such as, for cancer - QLQ-C30 (Aaronson et al., 1993), for Multiple Sclerosis - MSQOL 54 (Vickrey et al., 1995), for epilepsy - ESI 55 (Vickrey et al., 1992).
Developmental Assets
Profile of Student Life: Attitudes and Behaviors ® (A&B) - Questionnaire developed by the Search Institute (Benson et al., 1998; Leffert et al., 1998; Search Institute, 2019) and validated for European-Portuguese by Soares, Pais-Ribeiro and Silva (2018a; 2018c). It is addressed to adolescents whose ages range from 12 to 18 years in the school context, or, more specifically, to adolescents who are currently attending to the 2nd and 3rd cycle of basic education, to secondary education in the Portuguese education system (in the original, middle school-high school, corresponding to the educational system in the United States of America) (Leffert et al., 1998).
The assessment of the experience of the 40 individual assets comprehends 92 items, mainly consisting of statements in relation to which the answer options correspond to a five position Likert scale that range from, for instance, 1 = strongly agree” to 5 = strongly disagree, 1 = not important to 5 = extremely important, 1 = not at all like me to 5 = very much like me.
There are two approaches to describe the experience of Assets: 1) Data can be analyzed assuming that it is a Likert scale, thus the value obtained for each of the assets is interpreted as follows: the higher the score, the greater the experience of the Asset; 2) On the other hand, for communicational purposes, the score for each Asset can be used as a dichotomous variable, i. e, the adolescent has or doesn’t have the Asset. This score corresponding to each 40 Assets yields an Index for which the punctuation ranges from 0-40 Assets, which describes the average number of Assets that each adolescent has. This approach also affords the analysis of the concept of Asset Levels, which reflects the broader continuum of healthy development and defines four Asset Levels based on the Asset Index experienced by the adolescent. It represents a developmental continuum ranging from “At-risk” to “Optimal”, as well as the Asset Building axiom “the more assets, the better”: Level 1 - At-risk Development: 0 to 10 Assets; Level 2 - Vulnerable Development: 11 to 20 Assets; Level 3 - Adequate Development: 21 to 30 Assets; and Level 4 - Optimal Development: 31 to 40 Assets (Benson et al., 1998; Leffert et al., 1998).
The Portuguese version of the A&B questionnaire has similar validity characteristics to the original version (Soares et al., 2018c). Twenty-one of the 40 Assets are measured by at least 3 items. Most of them show internal consistency values that are considered acceptable, ranging from .60 to .80 (Cronbach, 1951). Thirteen Assets are measured using individual items, therefore such an evaluation cannot be applied. The evaluation of internal consistency of Categories: Support α = .81; Empowerment α = .76; Limits an Expectations α = .65; Constructive use of time α = .39 (multidimensional category); Commitment to Learning α = .67; Positive Values α = .78; Social Competences is α = .72; Positive Identity α = .83. Dimensional Analysis of: External Assets α = .84; Internal Assets α = .84.
Procedure
To carry out this research, consent was obtained from the Directorate-General for Education. This study was conducted in accordance with the regulations of professional ethics, as per the declarations of the Order of Portuguese Psychologists (2016). The National Commission for the Protection of Data confirmed the anonymity of the participants during data collection by giving a favorable review. For data collection, authorizations were requested to the General Council and the Director of School Grouping, and Professors. The parents/legal guardians of all students who participated in the study signed the free and informed consent form for data collection, use and publication of results. Data collection was carried out in classrooms with standardized instructions. The students who obtained parental/legal guardian consent for participation were invited to respond to the questionnaires and to put them in an envelope. Anonymity and confidentiality were assured, as well as the use of the data for research purposes exclusively.
Results
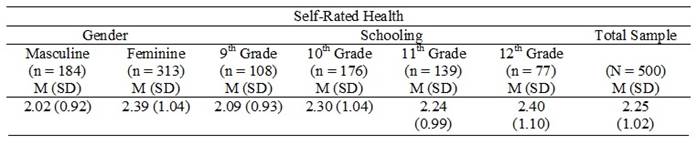
Health Perception
Table 2 shows mean scores (and standard deviations between brackets) of SRH by gender, age, years of schooling, and total sample. Data indicate that adolescents’ mean score for Self-rated Health is 2.25 (SD = 1.02). Taking gender into consideration, we observed statistically significant differences in mean scores, which indicate that boys (M= 2.02; SD = 0.92) report a better Health Perception in comparison with girls (M = 2.39; SD = 1.04), t (495) = 3.96, p < .0001. It was confirmed that there tends to be no statistically significant correlation between age and Health Perception, r (501) = .07, p = .13. Results also suggest there is no statistically significant difference in mean scores of SRH among the years of schooling, F (3.496) = 1.57, p = .19.
Results from this study indicate that the highest percentage of adolescents (88% of them) report that their Health Perception ranks between Good, Very Good and Excellent: 28.7% (n = 144) report their Health Perception as being Excellent; 29.8% (n = 150) report Very Good; 29.4% (n = 148) report Good. The rest, 10.9% (n = 55), report their Health Perception as begin Fair and 0.8% (n = 4) report Poor.
Effects of Cumulative Experience of Developmental Assets in Health Perception
Table 3 shows mean scores (and standard deviations between brackets) of SRH of the total sample of adolescents and by the Asset Level that the adolescents report - i. e, the four Levels of Assets defined as 0-10, 11-20, 21-30 and 31-40 Assets. In order to analyze the cumulative impact of the experience of developmental assets in SRH, an analysis of variance was conducted (one-way ANOVA, Post-Hoc Bonferroni). Results point to the existence of statistically significant differences according to the number of assets experienced by adolescents in different groups, F (3.463) = 15.78, p < .0001 (Post-Hoc Bonferroni test indicates that all groups differ significantly among each other). It is possible to observe that adolescents with higher asset levels, i. e, who experience a greater number of assets, tend to report a better SRH.

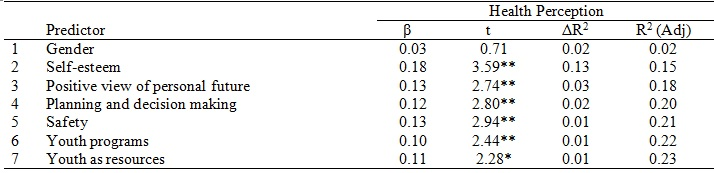
Developmental Assets Predictors of Health
In order to determine which developmental assets and which demographic variables produce results in SRH, a stepwise multiple regression analysis (Table 4). Two sets of predictive variables were included. The first one included demographic measures as predictive variables (gender, age and schooling of the adolescent) and the second, in addition, the 40 developmental assets. Results suggest that gender (masculine) is an independent significant predictor of SRH in adolescents; this factor represents 3% of the variance in the results. An addition of the asset variables revealed that Self-esteem Internal Asset contributed the most in the prediction of SRH, and that Positive view of Personal Future Asset, Planning and Decision Making, experience of Safety, participation in Youth Programs and the experience of Youth as Resources also produced significant predictability. The final model accounted for 23% of the variance in the results for SRH of the adolescents: R2=0.24; R2(Adj.) = 0.23, F (7.462) = 20.5, p < .0001.
Discussion
The results of this study indicate that the largest percentage of adolescents (88% of the adolescents) state that their Health Perception is located within the positive interval, i.e., between Good, Very good and excellent. It can be observed that the adolescents’ SRH is within the interval corresponding to Very Good. Following the studies’ estimates, the results indicate that a better SRH is associated to a greater experience of Developmental Assets. These suggest that the higher the number of Developmental Assets the adolescent reports to experience, the larger the probability of their also disclosing a better SRH, therefore these data support the assumption of the additive nature of Assets in relation to their impact on positive developmental outcomes for adolescents, thus expanding the specific knowledge to the results in relation to SRH. In turn, these results are in line with Benyamini’s (2011a) the suggestion that SRH results reflect the resources of a person.
If we consider demographic variables, the data from the present study suggest that only the gender variable contributes to the variance of results in SRH. Previous studies with adults suggest the existence of gender differences in SRH, which in comparison becomes a stronger health predictor among men than among women (Benyamini et al., 2000). Research on gender and age differences in adolescents’ SRH led to non-consensual results. On the one hand, in line with the present study results, most studies indicate that, boys rate their health at comparatively higher levels (Benyamini, 2009; Benyamini et al., 2000; Craig et al., 2018; Currie et al., 2012; Jardén et al., 2011; Vingilis et al., 2002), even though some studies indicate that the causal effect decreases with the inclusion of other personal and contextual factors (Breidablik, Meland, & Lydersen, 2009; Vingilis et al., 2002). On the other hand, no significant differences were found in relation to age and schooling. We also found that the age variable did not contribute to the variance of results for SRH. These results could suggest theoretically that this study focused on a homogenous group of adolescents that were exposed to a context that involves similar experiences.
Previous studies reports are inconsistent regarding the trajectories of SRH considering gender and age through adolescence. Jardén et al. (2011) observed that during adolescence, girls described their health and reported lower levels than boys, and that this gender difference increased over the years. In turn, in a study conducted by Potrebny et al. (2019), a lower proportion of girls, in comparison with boys, classified their health as excellent, however, it was observed that, as time went by, the number of boys that evaluated their health as being excellent decreased, while the evaluations carried out by girls improved. In a similar vein, in a study by Sokol et al. (2017) conducted with the aim of observing SRH trajectories from 13 to 31 years of age, results indicated that men obtained better initial SRH results, in comparison to women, however, they also experience larger declines in SRH over time. The authors suggested that this could be attributed to the emergences of hegemonic masculinity ideas, associated in previous studies to risk health-related behaviours (Heath et al., 2017; Kreager & Staff, 2009; Wells et al., 2014). Theoretically, this construal of gender corresponds to a constructionist approach, according to which, gender-based demands create different kinds of femininity and masculinity conceptions (Connell, 2014).
Breidablik et al. (2009) observed that over 4 years’ time girls reported a deterioration of their SRH with higher frequency than boys, nevertheless, this difference among genders, as well as the differences among age groups, became non-significant in multivariate models, leading the authors to conclude that SRH is a relative stable construct during adolescence, and that it deteriorates steadily when there is a lack of general wellbeing and of the frequency of healthcare services, disability, and lifestyle factors that compromise health.
Biological and social differences between women and men, as well as their interaction, lead to gender differences in the perception of health and disease. These factors can also interact, in such a way that different symptoms or diseases, experienced in different social contexts, which generate gender-based expectations, can lead to larger differences than those observed in relation to biological and social factors separately (Benyamini, 2011a).
Thus, the results of this study suggest that interventions aimed at improving adolescents’ general health can be more effective, if gender specific actions are considered. In turn, we emphasize that the effect of gender and age on SRH can depend on the specific sociocultural context itself (Benyamini, 2011a; Potrebny et al., 2019), and the need of conducting further investigations in order to better analyze this issue is suggested. From the perspective of public health, it is also important to acknowledge possible macro-level influences in health, and to foster public policies that promote health. As Benyamin (2011a) explains, is seems impossible to understand SRH without taking into consideration the cultural context within which they are formulated.
In turn, data suggest the impact of a subset of Developmental Assets on adolescent health prediction, which indicates that both, Internal and External Assets, would contribute to the variance in the results, with Internal Assets being the stronger predictors. Self-esteem Internal Asset, which belongs to the category of Positive Identity, constitutes the stronger predictor of SRH. These results are congruent with a research that suggests that the most important component of health/disease perception is identity (Benyamini, 2011a; Rees, Fry, Cull, & Sutton, 2004). Additionally, Positive View of Personal Future, also belonging to the category of Positive Identity, which indicates to what extent an adolescent is optimistic in relation to his/her personal future, also contributed to health prediction. Benyamini et al. (2011) argue that health perception is expected to be related to worldview and generalized expectations for the future, since they involve perceptions and expectations for the present and the future that are specific to health conditions. Also related to internal resources, the results highlight the important of Social Competences involving the personal capacity for Planning and Decision Making, which points to the adolescent’s ability to plan in advance and to make choices related to the prediction of health. In line with these results, Benyamini et al. (2011) suggest that the preservation of a sense of mastery and control, even in spite of very poor health, could constitute an indicator or a causal factor for survival. Likewise, External Assets, which provide contextual or environmental support conditions to optimize health, also could produce significant predictability. Results highlight the importance of the experience of Safety, i. e, of adolescents feeling safe at home, in school, in their neighborhood and their communities. Adolescents who express feelings of safety have a larger probability of feeling healthy than those who perceive their safety as being threatened (Benson, 2006; Simonsen et al., 2017). The experience of participating in Youth Programs, related to the category of Constructive Use of Time, which conveys the importance of the participation in sports, clubs and school/community events, also produced significant predictability. These results match previous studies that suggest that physical activity is an important factor that produces changes in the perception of health and predicts lower mortality rates (Benyamini et al., 2011). In turn, in line with previous studies (Simonsen et al., 2017) results also highlight the experience of Youth as Resources, which focuses on the capacity of the community to provide opportunities that allow adolescents to contribute significantly to society, and they also indicate to what extent the community encourages youth undertaking an active role, which is also an important predictor of health.
This study’s results should be interpreted by taking into consideration the following limitations we now describe. On account of the transversal design of the study, causal relations cannot be inferred between SRH results and the experience of Developmental Assets. The development of longitudinal studies is needed to determine whether SRH results are a consequence or a determinant of the experience of Developmental Assets.
Conclusion
Self-Related Health perceptions, as Benyamini (2011a, p. 305) explains, organize our health-related knowledge and experience into meaningful structures that we use to interpret new experiences and determine how to cope with them, an activity which constitutes the main and central component of the dynamic self-regulatory process of health. SRH is, as noted above, the product of the interaction between personal characteristics and actions of social agents, such as families, educational system and contextual conditions. This study suggests the utility of the Developmental Assets® framework for the understanding of the dynamics of the self-regulatory process of internal (self-system) and external (sociocultural system) effects. It is also noteworthy, that health perceptions reflect personal resources, which reflect or even affect the ability to cope with health threats (Benyamini, 2011b). Thereby, the Developmental Assets model furnishes a holistic approach to the understanding of adolescents’ positive development, as it introduces a conceptual and methodological framework that posits a conception of the adolescent that is based on his/her strengths, with special attention to the factor that favor the optimal development of adolescents, i.e., focused on resources that can be explored either at an individual level or at the level of developmental contexts (such as family, school, community), in order to foster a positive development in adolescence (Benson, 2006; Benson et al., 2006; Benson & Scales, 2011; Benson et al., 2011). It should be noticed that these Assets were selected for their being constitutive of positive experiences, relations, abilities, which can be promoted by those persons who are close to the adolescents, namely, parents, professors, other significant adults, independently from of macro-level influences on health. Adults are in a crucial position to intervene by creating environments that allow for adolescents to encounter positive experiences. It is important to highlight that, such personal resources, be they external or internal, thereby constitute factors that can lead to different future health trajectories (Benyamini, 2011b).
This research suggests the applicability and usefulness of the Developmental Asset framework for the understanding of Self-Rated Health in adolescents, as well as of the Asset Building strategy, not only to attempt to build all the 40 Assets in the life of adolescents, but also to promote specific Assets with the purpose of fostering or achieving an optimal status and developmental process in adolescence.
REFERENCES
Aaronson, N., Ahmedzai, S., Bergman, B., Bullinger Cull, A., Duez, N. ... Takeda, F. (1993). The European Organization for Research and Treatment of Cancer QLQ-C30: A quality of life instrument for use in international clinical trials in oncology. Journal of the National Cancer Institute, 85(5), 365-375. doi: 10.1093/jnci/85.5.365 [ Links ]
Benson, P. L. (2006). All kids are our kids: What communities must do to raise caring and responsible children and adolescents (2nd ed.). San Francisco, CA: Jossey-Bass. [ Links ]
Benson, P. L. (2007). Developmental Assets: An overview of theory, research, and practice. In R. K. Silbereisen & R. M. Lerner (Eds.), Approaches to Positive Youth Development (pp. 33-58). Thousand Oaks, CA: Sage Publications Ltd. doi: 10.4135/9781446213803.n2 [ Links ]
Benson, P. L., Leffert, N., Scales, P. C., & Blyth, D. A. (1998). Beyond the “village” rhetoric: Creating healthy communities for children and adolescents. Applied Developmental Science, 2, 138-59. doi: 10.1207/s1532480xads0203_3 [ Links ]
Benson, P. L., & Scales, P. C. (2009). Positive youth development and the prevention of youth aggression and violence. International Journal of Developmental Science, 3, 218-234. doi: 10.3233/DEV-2009-3302 [ Links ]
Benson, P. L., Scales, P. C., Hamilton, S. F., & Sesm Jr., A. (2006). Positive youth development: Theory, research and applications. In W. Damon, & R. M. Lerner (Eds.), Handbook of child psychology. Theoretical models of human development (6th ed.), (pp. 894-941). New York, NY: John Wiley. doi: 10.1002/9780470147658.chpsy0116. [ Links ]
Benyamini, Y. (2008). Self-ratings of health and longevity: A health psychologist's viewpoint on epidemiological findings. European Health Psychologist, 10, 10-12. [ Links ]
Benyamini, Y. (2009). Stress and Coping with Women’s Health Issues: A Review from a Self-Regulation Perspective. European Psychologist, 14, 63-71. doi: 10.1027/1016-9040.14.1.63 [ Links ]
Benyamini, Y. (2011a). Perceptions of health and illness. In H.S. Friedman (Ed.), The Oxford handbook of health psychology (pp. 285-318). New York, NY: Oxford University Press. [ Links ]
Benyamini, Y. (2011b). Why does self-rated health predict mortality? An update on current knowledge and a research agenda for psychologists. Psychology & Health, 26 (11), 1407-1413. doi: 10.1080/08870446.2011.621703 [ Links ]
Benyamini, Y., Blumstein, T., Murad, H., & Lerner-Geva, L. (2011). Changes over time from baseline poor self-rated health: For whom does poor self-rated health NOT predict mortality? Psychology and Health, 26, 1446-1462. doi: 10.1080/08870446.2011.559231 [ Links ]
Benyamini, Y., & Idler, E.L. (1999). Community studies reporting association between self-rated health and mortality: Additional studies, 1995-1998. Research on Aging, 21, 392-401. doi: 10.1177/0164027599213002 [ Links ]
Benyamini, Y., Idler, E. L., Leventhal, H., & Leventhal, E. A. (2000). Positive affect and function as influences on self-assessments of health: Expanding our view beyond illness and disability. The Journals of Gerontology Series B: Psychological Sciences and Social Sciences, 55, 107-116. doi: 10.1093/geronb/55.2.P107 [ Links ]
Benyamini, Y., Leventhal, E. A., & Leventhal, H. (2000). Gender differences in processing information for making self-assessments of health. Psychosomatic Medicine, 62, 354-364. doi: 10.1097/00006842-200005000-00009 [ Links ]
Bishop, F., & Yardley, L. (2010). The development and initial validation of a new measure of lay definitions of health: The wellness beliefs scale. Psychology and Health, 25, 271-287. [ Links ]
Breidablik, H. J., Meland, E., & Lydersen, S. (2009). Self-rated health during adolescence: stability and predictors of change (Young-HUNT study, Norway). The European Journal of Public Health, 19(1), 73-78. doi: 10.1093/eurpub/ckn111 [ Links ]
Connell, R. W. (2014). Gender and power: Society, the person and sexual politics. Oxford: John Wiley & Sons. [ Links ]
Craig, B. A., Morton, D. P., Morey, P. J., Kent, L. M., Gane, A. B., Butler, T. L., ... & Price, K. R. (2018). The association between self-rated health and social environments, health behaviors and health outcomes: a structural equation analysis. BMC Public Health, 18, 440. doi: 10.1186/s12889-018-5323-y [ Links ]
Cronbach, L. J. (1951). Coefficient alpha and the internal structure of tests. Psychometrika, 16, 297-334. doi: 10.1007/BF02310555 [ Links ]
Currie, C., Zanotti, C., Morgan, A., Currie, D., De Looze, M., Roberts, C., ... & Barnekow, V. (2012). Social determinants of health and well-being among young people. Health Behaviour in School-aged Children (HBSC) study: international report from the 2009/2010 survey. Copenhagen: WHO Regional Office for Europe, Health Policy for Children and Adolescents. [ Links ]
Doiron, D., Fiebig, D. G., Johar, M., & Suziedelyte, A. (2015). Does self-assessed health measure health? Applied Economics, 47, 180-194. doi: 10.1080/00036846.2014.967382 [ Links ]
Eurostat (2020). Eurostat statistics explained. Retrieved from:https://ec.europa.eu/eurostat/statistics-explained/index.php?title=Glossary:Self-perceived_health [ Links ]
Ferreira, P., & Santana, P. (2003). Percepção do estado de saúde e de qualidade de vida da população activa: Contributo para a definição de normas portuguesas. Revista Portuguesa de Saúde Pública, 21, 15-30. [ Links ]
Ford, D. H., & Lerner, R. M. (1992). Developmental systems theory: An integrative approach. Newbury Park, CA: Sage Publications. [ Links ]
Gottlieb, G. (1997). Synthesizing nature-nurture: Prenatal roots of instinctive behavior. Mahwah, NJ: Lawrence Erlbaum. [ Links ]
Gottlieb, G., Wahlsten, D. & Lickluter, R. (2006). The significance of biology for human development: A developmental psychobiological systems perspective. In R. M. Lerner (Ed.) Theoretical models of human development: Handbook of Child Psychology (6th ed.) (vol.1, pp. 210-257). Hoboken, NJ: Wiley. [ Links ]
Heath, P. J., Brenner, R. E., Vogel, D. L., Lannin, D. G., & Strass, H. A. (2017). Masculinity and barriers to seeking counseling: The buffering role of self-compassion. Journal of Counseling Psychology, 64 (1), 94-103. doi: 10.1037/cou0000185 [ Links ]
Idler, E. L., & Benyamini, Y. (1997). Self-rated health and mortality: a review of twenty-seven community studies. Journal of health and social behavior, 38, 21-37. doi: 10.2307/2955359 [ Links ]
Jerdén, L., Burell, G., Stenlund, H., Weinehall, L., & Bergström, E. (2011). Gender differences and predictors of self-rated health development among Swedish adolescents. Journal of Adolescent Health, 48, 143-150. doi: 10.1016/j.jadohealth.2010.06.005 [ Links ]
Joffer, J., Jerdén, L., Öhman, A., & Flacking, R. (2016). Exploring self-rated health among adolescents: a think-aloud study. BMC Public Health , 16, 156. doi: 10.1186/s12889-016-2837-z [ Links ]
Jylhä, M. (2009). What is self-rated health and why does it predict mortality? Towards a unified conceptual model. Social, Science Medicine, 69, 307-316. doi: 10.1016/j.socscimed.2009.05.013. [ Links ]
Kreager, D.A., & Staff, J. (2009). The sexual double standard and adolescent peer acceptance. Social Psychology Quarterly, 72(2), 143-164. doi: 10.1177/019027250907200205 [ Links ]
Lerner, R.M., & Steinberg, L. (2009). The scientific study of adolescent development. In R. M.., Lerner & L. Steinberg (Eds.), Handbook of adolescent psychology (3rd ed.), (Vol. 1, pp. 3-14). New Jersey, NJ: John Wiley & Sons, Inc. doi: 10.1002/9780470479193.adlpsy001002 [ Links ]
Ordem dos Psicólogos Portugueses (2016). Código Deontológico da Ordem dos Psicólogos Portugueses. Retrieved from https://www.ordemdospsicologos.pt/ficheiros/documentos/web_cod_deontologico_pt_revisao_2016.pdf [ Links ]
Overton, W.F. (2006). Developmental psychology: Philosophy, concepts, and methodology. In W. Damon & R. M. Lerner (Eds.), Theoretical Models of Human Development. Handbook of child psychology (5th ed.), (Vol. 1, pp.107-188). Hoboken, NJ: Wiley . [ Links ]
Overton, W.F. (2013). A new paradigm for developmental science: Relationism and relational-developmental systems. Applied Developmental Science , 17, 94-107. doi: 10.1080/10888691.2013.778717 [ Links ]
Overton, W.F., & Müller, U. (2012). Metatheories, Theories, and Concepts in the Study of Development. In Irving B. Weiner (Ed.), Handbook of Psychology (2nd ed), (Vol. 6, pp. 19-58). Hoboken, NJ: John Wiley & Sons, Inc. doi: 10.1002/9781118133880.hop206002 [ Links ]
Pais-Ribeiro, J.L. (2005). O importante é a Saúde: Estudo de adaptação de uma técnica da perceção do Estado de Saúde. Lisboa: Fundação Merck Sharp & Dohme. [ Links ]
Pinquart, M. (2001). Correlates of subjective health in older adults: A meta-analysis. Psychology and Aging, 16, 414-426. doi: 10.1037/0882-7974.16.3.414 [ Links ]
Potrebny, T., Torsheim, T., Due, P., Välimaa, R., Suominen, S., & Eriksson, C. (2019). Trends in excellent self-rated health among adolescents: A comparative Nordic study. Nordisk välfärdsforskning| Nordic Welfare Research, 4(02), 67-76. doi: 10.18261/issn.2464-4161-2019-02-04 [ Links ]
Rees, G., Fry, A., Cull, A., & Sutton, S. (2004). Illness perceptions and distress in women at increased risk of breast cancer. Psychology & Health, 19, 749-765. doi: 10.1080/08870440412331279764 [ Links ]
Scales, P.C., Benson, P. L., Leffert, N., & Blyth, D.A. (2000). Contribution of developmental assets to the prediction of thriving among adolescents. Applied Developmental Science, 4, 27-46. doi: 10.1207/S1532480XADS0401_3 [ Links ]
Scales, P.C., Benson, P.L., Roehlkepartain, E.C., Sesma, A., & van Dulmen, M. (2006). The role of developmental assets in predicting academic achievement: A longitudinal study. Journal of Adolescence, 29, 691-708. doi: 10.1016/j.adolescence.2005.09.001 [ Links ]
Search Institute (2019). User guide for the Attitudes & Behaviors survey. Retrieved from http://www.search-institute.org/sites/default/files/a/A&B-Survey-User-Guide.pdf [ Links ]
Simonsen, N., Ylönen, A., Suominen, S., Roos, E., Välimaa, R., Tynjälä, J., & Kannas, L. (2017). Associations between empowerment-enabling environments and self-rated health among adolescents. European Journal of Public Health, 27(3), ckx187.728. doi: 10.1093/eurpub/ckx187.728 [ Links ]
Soares, A.S., Pais-Ribeiro, J.L., & Silva, I. (2018a). Recursos do desenvolvimento na adolescência: Revisão integrativa. Ciências Psicológicas, 12, 45-57. doi: 10.22235/cp. v12i1.1594 [ Links ]
Soares, A.S., Pais-Ribeiro, J.L., & Silva, I. (2018b). Adaptação portuguesa do questionário Profile of Student Life: Attitudes and Behaviors (A&B). Manuscript submitted for publication. [ Links ]
Sokol, R., Ennett, S., Gottfredson, N., & Halpern, C. (2017). Variability in self-rated health trajectories from adolescence to young adulthood by demographic factors. Preventive Medicine, 105, 73-76. doi: 10.1016/j.ypmed.2017.08.015. [ Links ]
Vickrey, B.G., Hays, R.D-, Graber, J., Rausch, R., Engel, J. Jr, Brook, R.H. (1992). A health-related quality of life instrument for patients evaluated for epilepsy surgery. Medical Care, 30, 299-319. doi: 10.1097/00005650-199204000-00002. [ Links ]
Vickrey, B.G., Hays, R.D., Harooni, R., Myers, L.W., & Ellison, G.W. (1995). A health-related quality of life measure for multiple sclerosis. Quality of Life Research, 4, 187-206. doi: 10.1007/BF02260859 [ Links ]
Vingilis, E. R., Wade, T. J., & Seeley, J. S. (2002). Predictors of adolescent self-rated health: analysis of the National Population Health Survey. Canadian Journal of Public Health/Revue Canadienne de Santé Publique, 93, 193-197. [ Links ]
Wells, S., Flynn, A., Tremblay, P. F., Dumas, T., Miller, P., & Graham, K. (2014). Linking masculinity to negative drinking consequences: The mediating roles of heavy episodic drinking and alcohol expectancies. Journal of Studies on Alcohol and Drugs, 75(3), 510-519. doi: 10.15288/jsad.2014.75.510 [ Links ]
Ware, J. E., Snow, K. K., Kosinski, M., & Gandek, B. (1993). SF-36® health survey manual and interpretation guide. Boston, MA: New England Medical Center, the Health Institute. [ Links ]
How to cite: Soares, A., Pais-Ribeiro, J. L., & Silva, I. (2020). Personal and contextual developmental assets predictors of health perception in adolescence. Ciencias Psicológicas, 14(2), e2263. doi: https://doi.org/10.22235/cp.v14i2.2263
Correspondence: Ana Soares, Faculdade de Psicologia e de Ciências da Educação da Universidade do Porto. Correspondencia: Avenida Joaquim Ferreira Araújo, nº11, 4730-280, Marrancos, Vila Verde. E-mail: anasofiabsoares@gmail.com. José L. Pais-Ribeiro, Faculdade de Psicologia e de Ciências da Educação da Universidade do Porto. E-mail: jlpr@fpce.up.pt. Isabel Silva, Universidade Fernando Pessoa, Porto. E-mail: isabels@ufp.edu.pt
Authors' participation: a) Conception and design of the work; b) Data acquisition;c) Analysis and interpretation of data; d) Writing of the manuscript; e) Critical review of the manuscript. A.S. has contributed in a,b,c,d,e; J.L.P-R in a,b,c,d,e; ; I.S in ,b,c,d,e.
Received: February 12, 2019; Accepted: August 16, 2020
 Este é um artigo publicado em acesso aberto sob uma licença Creative Commons
Este é um artigo publicado em acesso aberto sob uma licença Creative Commons
