











 texto en
texto en  Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo

 Permalink
PermalinkIntroduction
The positive dimension of health has been highlighted by OMS (2016) as “a state of complete physical, mental and social well-being, and not only the absence of affections or diseases”, a concept that over the years has incorporated constructs ranging from the medical model of presence or absence of disease, to highlighting the capabilities and potential of the human being as tools for personal growth, which according to Barrera and Flores (2015) have resulted in an expansion of the vision towards greater complexity around the conceptualization and the theoretical approach.
Traditionally, research in the field of psychology has been focused on mental health problems, but we now know that this approach does not provide a complete assessment of an individual’s mental health. Thus in recent years there has been a growth in interest in the general functioning of the human being and mental health in particular (Kokko, Korkalainen, & Lyyra, 2013). In addition, studies have shown that positive functioning in mental health is associated with psychological well-being and social well-being, the advantages of its study can be seen throughout the life cycle, besides the research on positive psychology and well-being have been strengthened by this type of studies (Keyes, 2005).
The study of well-being in the area of psychology begins in two broad lines, hedonic and eudamonic (Keyes, Corey, Shmotkin, & Ryff, 2002). The first one represented by research focused on the study of subjective well-being, an indicator of people’s appreciation of satisfaction with life, happiness and positive affective capacities, and the second one oriented towards psychological well-being, a concept that includes social, subjective and psychological dimensions, as well as behaviors related to health in general that respond to the positive functioning of the human being. These authors indicate that subjective and psychological well-being are related, and although their dimensions differ in certain aspects, there is apparently a certain overlap between some constructs, such as: self-acceptance corresponding to the subjective well-being model, and domain of the environment that would belong to the psychological well-being model and that reffers to the ability of people to create or choose environments that favor the satisfaction of their needs and desires (Blanco & Diaz, 2005), the two dimentions can overlap or hide the one in the other when trying to observe them.
We can see that the theories complement each other, and although each theory defends the fact that the dimensions are unique, we consider important that in addition to the two traditional lines of study it is necessary to register the human being in a social setting (Blanco & Diaz, 2005). This is why the proposal of studying welbeing from the multidimensional model by Keyes (2007) is usefull because these models integrates theories and components from both the hedonic and eudaimonic perspectives (Huppert & So, 2013 Keyes, 2007). The model emphasizes that positive mental health integrates emotional well-being: constituted of affections, positive- high and negative - low, psychological well-being, composed by self-acceptance, personal growth, purpose in life, mastery of the environment, personal autonomy and positive relations with others and social welfare constituted by the social acceptance perceived by the subject, social updating (where the healthy subject relies on the future of society, its potential for growth and development and its capacity to produce welfare), social contribution, social cohesion and social integration.
This theory was the basis to develop the Mental Health Continuum Long Form, MHC-LF scale, which in first instance consisted of 40 items and was a self-registration questionnaire. (Keyes, 2002; 2005; 2007). Subsequently a shorter version was developed with the Mental Health Continuum Short Form (MHC-SF) (Keyes, 2009) with 14 items. This version was quickly popularized because of its brief application retaining its self-registration quality.
MHC-SF has been translated into different languages and validated through various cultural contexts (Carvalho, Salgado, Marquéz, & Marocó, 2016; Joshanloo, Wissing, Khumalo, & Lamers, 2013; Karaś, Cieciuch, & Keyes, 2014; Petrillo, Capone, Caso, & Keyes, 2015), confirming the tri factor structure in most studies, although in the Serbia and South Africa adaptations the model does not replicate and appears as a bifactorial model (du Plessis & de Bruin, 2015; Jovanović, 2015) which is explained as a reasonable solution for multidimensional scales such as the MCH-SF (Chen, West, Sousa, 2006).
As for the reliability of the original version of the MHC-SF, the scale has shown an internal consistency measured by the Cronbach’s alpha always higher than 80. in adolescents (ages 12-18) and adults in the United States, Netherlands and South Africa (Keyes, 2005; 2009; Lamers, Glas, Westerhof, & Bolemeijer, 2011). The reliability test re-test of the MHC-SF over three successive periods of 3 months averaged .68 and the 9-month test re-test average was .65 (Lamers et al., 2011). The factorial structure was conserved in the two forms of the scale (long and short) with its model of three factors: emotional, psychological and social well-being.
To examine the divergent validity of the test, the results of the Brief Symptom Inventory have been correlated with the MHC-SF resulting in correlations of -.34 (Lamers et al.2011). In addition, the MHC-SF was analyzed in conjunction with the Positive and Negative Affect Schedule, (PANAS PN), General Health Questionnaire (GHQ), with a negative correlation in the sub scales of negative affect in a moderate range between -.33 and -.45 (Petrillo, Capone, Caso, & Keyes, 2015).
Several studies of adaptation and validation of the MHC-SF scale have been performed demonstrating good adjustment levels in general. In China, a study was carried out to verify the internal reliability, dimensional structure and invariance between groups and the presence of ceiling and floor effects that was applied to a sample of 5,399 people. This study involved the translation of the questionnaire thruogh a Chinese research group who used the traslation - retro translation method applied in a pilot study with a sample of 285 students, using confirmatory factor analysis the three factors suggested in the original scale were confirmed and the reliability indicated a Cronbach alpha of .80 indicating good consistency, and that ceiling and floor effects were insignificant (Guo et al., 2015).
The scale has also been adapted in several cultural contexts such as Italy (Petrillo, Capone, Caso, & Keyes, 2015), Poland (Karaś, Cieciuch, & Keyes, 2014), Portugal (Carvalho, Salgado, Marquéz, & Maroco, 2016), Holland, Iran, and South Africa in which Cronbach’s alpha values have oscillated between .86 and.95, most of them reiterating the three-dimensionality of the model and fitting adjustments in the factorial model (Joshanloo, Wissing, Khumalo, & Lamers , 2013). As for Latin American countries, the MHC-SF was translated into Spanish and applied to a sample of 3,335 adults in Chile, through factor analysis they tested the three- and two-factor models and although they obtained an appropriate adjustment in the two factor model, the three factor model showed a higher fit. The Cronbach alpha obtained was .94 showing high reliability (Echeverria, Torres, Pedrals, Padilla, Rigotti, & Bitran, 2017). In Argentina the psychometric properties of the scale were studied in a sample of 1,300 adults through confirmatory factor analysis, cross validation, factor invariance and correlations with external criteria, analysis in wich the results indicated an adequate fit to the three-factor model proposed by Keyes (2005; 2007; 2009) and results didn´t invariate in relation to sex and age, the internal consis- tence obtained was .89 with Cronbach’s alpha, results that support the model of the mental health continuum (Lupano Perugini, de la Iglesia, Castro Solano, & Keyes, 2017).
To confirm construct validity, several scales have been used: quality of life (MMQL) and depression (HADS), (Guo et al., 2015), Schedule of Positive Affection PANAS (Petrillo, Capone, Caso, & Keyes, 2015 ), and Life Satisfaction Scale (SWLS) (Joshanloo, Wissing, Khumalo, & Lamers, 2013).
Even though there are currently Spanish versions of the MHC-SF scale it is important to consider that in Ecuador there are no instruments that evaluate positive mental health; this is why it is necessary to adapt the instrument to our local environment because the Spanish language possesses idiomatic peculiarities associated with the different countries and regions in which it is spoken. The objective of the present study was to perform the psychometric adaptation and to provide data of convergent and discriminant validity and reliability of the Spanish version for the Ecuadorian context of the scale mental health continuum (MHC-SF). The main contribution of this study is to have the necessary tools adapted to the context to obtain reliable data in the assessment of positive mental health facilitating the accumulation of valid knowledge in an increasingly important field of psychology.
Method
Instruments
Sociodemographic questionnaire: it was elaborated by the research team and it collects data about age, sex, educational level, current occupation and income. The same questionnaire was applied in both studies.
Mental Health Continuum Short Form: A Spanish version of the scale was developed. The general translation and test adaptation rules (Guillemin, Bombardier, & Beaton, 1993) were followed, including the retro-translation (Brislin, Lonner, & Thorndike, 1973), considering that, at the time of writing, there were not published studies of adaptation or validation of the scale in Spanish.
Piloting stage was performed and the instrument was then applied to a second sample for the analysis of its psychometric properties. The short form continuum includes 14 items that of a Likert scale which ranges from one to six points, being 1 never and 6 every day, theoretically three items belong to the dimension of emotional well-being, five to social well-being, and 6 dimensions to psychological well-being (Keyes , 2009).
Perma Profiler by Buttler and Kern (2016): adapted Spanish version (Lima-Castro et al., 2017). This scale is composed of 23 items, 15 of them evaluate well-being, and three independent factors that are health, negative emotions and solitude. This 11-point Likert scale has values ranging from 0 (never) to 10 (always) or 0 (nothing) to 10 (completely). This scale reports adequate psychometric properties and was used only in the second study.
Sample 1
In the pilot phase, the sample included 100 people, 49% were male (n = 49), and 51% were female (n = 51) aged between 20 and 86 years, mean age of participants was 43.88 years and the standard deviation was 16.52 years). The sample belongs to the urban area of the city of Cuenca.
Procedure
The sample of this first part of the study was collected by home visit, using the method of convenience between May and June of 2016. Informed consent was requested. In addition to the questionnaire, a survey of sociodemographic factors was applied. Each participant was asked for information on the difficulties they encountered in answering each of the questions.
Results
In the piloting phase, it was observed that 38% of the population (n = 46) had difficulties in item number 7. (“People are basically good”), because it was not understood. Due to this reason, we checked the original version in English for a retro translation, and it is decided to restructure it as “People are good”. It should be emphasized that the modification was justified by the participants and the cultural characteristics of the population. The layout was also modified in the design of the test, to avoid confusion. Considering that the questions used a Likert scale, the numbers were placed under each question instead of the right side.
Sample 2
The sample was taken for convenience considering a universe of 315,839 people whose ages comprised between 19 and 89 years belonging to the city of Cuenca, considering the different sociodemographic characteristics of the population, and involved the participation of 562 people (M Edad = 42.31years, DE Edad = 4.26), of which 27.4% were men (n = 154) and 72.6.2% were women (n = 408), all Ecuadorians, residents of the city of Cuenca. With regard to the educational level of the participants, 1.4% (n = 8) marked without instruction; 8.4% (n = 47) marked less than high school level; 22.1% (n = 124) have a high school diploma; 67.6% (n = 380) have university studies. Finally, 3% (n = 3) do not answer the question. Regarding to the marital status, single 5.2% (n = 282), married 32.4% (n = 182), free union 1.8% (n = 10), separated 0.9% (n = 5), divorced 6.8% (n = 38) and widowed 7.3% (n = 41), did not answer.7% (n = 4).
The questionnaires were carried out from between August and September of 2016 and there was voluntary participation of people belonging to the University of Azuay, Cuenca, physical rehabilitation unit of the center of attention to retirees and relatives of patients, and the care center for the elderly of the Social Security Ecuadorian Institute (IESS). Participants answered the Perma Profile and a sociodemographic survey, after the signing an informed consent.
Procedure
The scale and the survey were administered by the authors of this paper. The respective permits of the institutions that participated in the investigation were obtained before the participants started filling the questionnaires. As part of the participants’ preparation process, the objectives of the study were reported, and the adults were instructed on how the questionnaire needed to be carried out. A survey to collect sociodemographic data was carried out at the same time. Participation was voluntary, the of the self-report scale was maintained with proper guidance and support to participants to answer all questions if possible. Each person took about 20 minutes to complete the questionnaire. At the end, a gift was given as an incentive to each of the participants.
Data Analysis
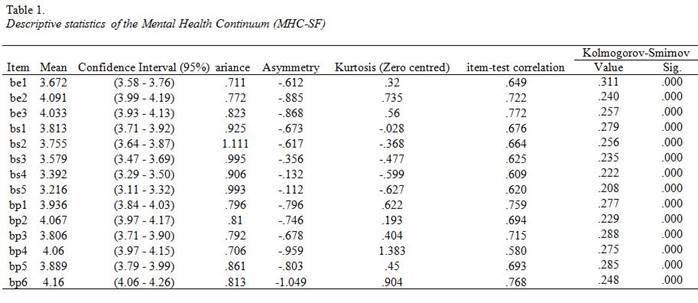
Descriptive statistics of the variables of the scale are evaluated, mainly asymmetry, kurtosis, item-test correlations and the distribution of items. 12 observations are eliminated since, despite the orientation of the interviewers, they were partially completed.
An exploratory factorial analysis (EFA) is performed to determine the number of dimensions to be considered and then to proceed with a confirmatory factor analysis (CFA).
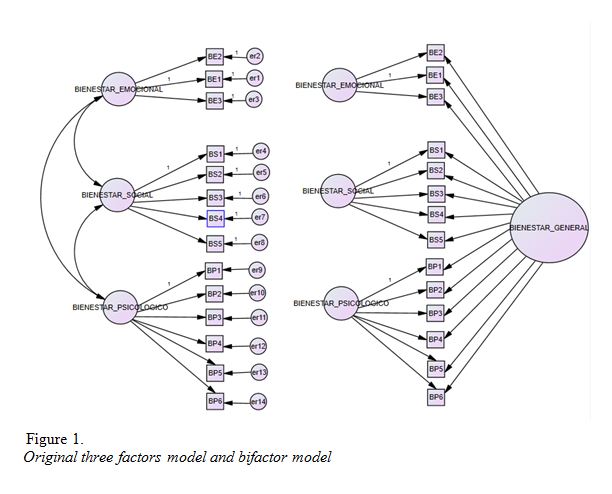
To evaluate the factorial structure of the scale is based on a model of structural equations with polychoric correlation matrices with a robust DWLS (Diagonally Weighted Least Squares) estimator which is the recommended method for small or medium samples (Rhemtulla, Brosseau-Liard, and Savalei, 2012 ). Along with previous studies, this paper hypothesises that the scale has three latent factors correlated with each other. Additionally, we evaluate a bifactorial model with three specific dimensions and a general one.
Several adjustment indices were used to evaluate the results, such as chi-square; CFI, and TLI [Tucker & Lewis index] whose values between .90 to .95 indicate acceptable model fit while values higher than .96 indicate good fit (Hu & Bentler, 1999). Also, RMSEA is used, whose value is considered acceptable when it is less than .08 and good when it is less than .05 (Steiger & Lind, 1980). The models described above are evaluated using the software FACTOR
In addition to the factorial validity, we evaluated the reliability of the scale using the Cronbach ‘s alpha and the McDonald’ s omega, considering that in the case of the first the values from .70 to .80 are considered acceptable, and above. 80 is considered to be highly reliable (Cicchetti, 1994). On the other hand, It is important to note that McDonald’s omega is useful when samples are large, preferably greater than 1000 observations (Ten Berge & Socan, 2004).
After confirming the factorial structure of the original scale, with qualitative modifications made in the pilot phase, we compared the sociodemographic variables to evaluate the results and differences between the categories of the variables. Spearman correlation tests, Kolmogorov-Smirnov normality tests, Wilcoxon rank sum test, Kruskal-Wallis test and the corresponding Dunn post hoc test were performed.
Results
Factorial validity
The descriptive statistics of the scale variables show that the data do not follow a normal distribution, which is initially observed by asymmetry and kurtosis and is later corroborated by the Kolmogorov-Smirnov test. The item-test correlations are positive and with moderate or vigorous magnitude. The data are shown in table 1.
Regarding the adequacy of the correlation matrix, a Barlett statistic of 3747.4 (df = 91; p = .000) was obtained while the Kaiser-Meyer-Olkin test showed a value of .9395 considered to be very good. These two values indicate that the matrix is factorizable.
The exploratory factor analysis suggests the presence of one factor. Consequently, in addition to the original three dimensions, we considered evaluating a bifactorial model with three specific dimensions and one general dimension as explained in figure 1.
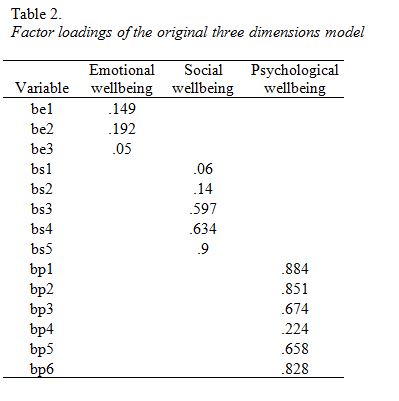
The confirmatory factor analysis (CFA) for the scale with the three factors proposed by the original author (Keyes, 2002) shows an adequate general adjustment by using the DWLS method and using polychoric correlation matrices. We obtained RMSEA = .045, CFI = .996, χ2 (52) Robust Mean and Variance-Adjusted Chi-Square = 109.048 (p = .000), GFI = .997, TLI = 0.993 The factor loadings are shown in table 2.
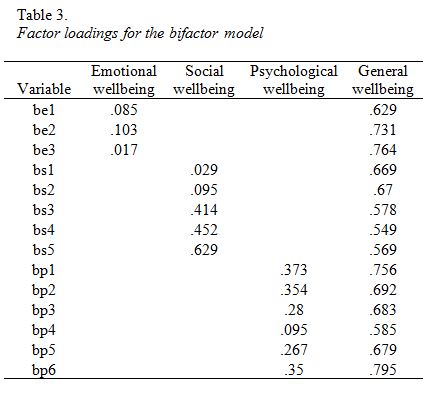
In addition, a confirmatory factor analysis (CFA) of the bifactorial model reported in another study (Echeverría et al, 2017) shows values of RMSEA = .042, CFI = .996, χ2 (52) robust with mean and variance adjusted = 103.040 (p = .000), GFI = .997, TLI = 0.993.
The factor loading matrix is presented in Table 3.
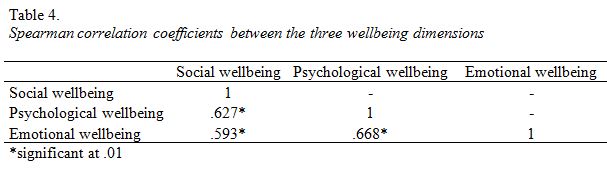
The Spearman correlation coefficient is calculated between the three dimensions of well-being whose results are presented in table 4.
Reliability
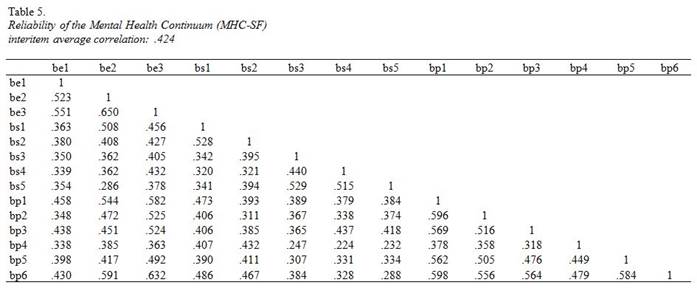
As for the reliability of the model as proposed by Keyes (2009), Cronbach’s alpha presents an overall value indicating high internal consistency for the total MHC-SF scale (α = .91). The coefficient of internal consistency for the Emotional Well-being sub-scale (α = .80) is valued as high, being the most representative item “I have felt satisfied with life”. The Social wellbeing sub-scale shows a moderate value (α = .72), its most representative item is “I have felt that I belong to a community, group, school or neighborhood”; Finally, the psychological well-being sub-scale presents an alpha considered high (α = .85), whose most representative item is “I have felt certain to express my own ideas and opinions”. The average inter-item correlations are presented in table 5. McDonald’s omega reaches a value of .933 although it is recommended to use it in samples of at least 1000 observations (ten Berge & Socan, 2004).
Also, the Pearson correlation coefficient is calculated with the Negative Emotions sub-scale of the Perma Profiler scale of Buttler and Kern (2016), adapted to Spanish version (Lima-Castro et al., 2017). The coefficient shows a moderate correlation (r = .30; p = .01) suggesting that the higher the positive mental health, the lower the degree of negative emotions.
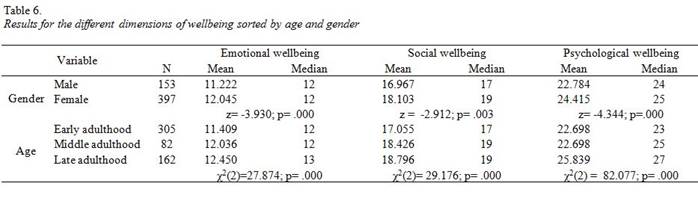
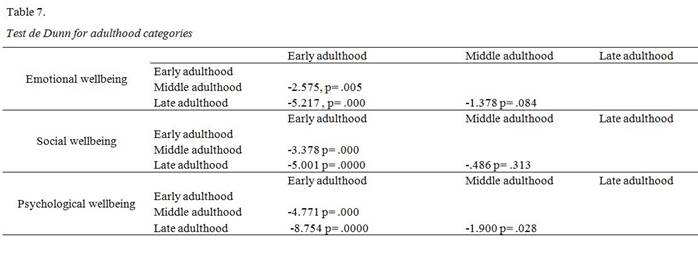
The Wilcoxon rank sum test (U of Mann-Whitney) is performed for two samples comparing the emotional, social and psychological well-being of men and women. Also, the Kruskal-Wallis test is performed for more than two groups and the subsequent post hoc Dunn test. Descriptive statistics and hypothesis test results are presented in tables 6 and 7.
Discussion
The present study evaluated the psychometric characteristics of Keyes Mental Health Continuum-Short Form (MHC-SF) (2009) which is a self-report questionnaire designed to measure positive mental health with three wellbeing sub-scales: emotional, psychological and social. It is composed of 14 items and was applied in the first instance to a convenience population of 100 people for a pilot to assess content validity. As a result, language level changes were made in the questionnaire. In the second stage, the questionnaire is applied to a population of 550 participants in a sample of convenience. The two samples were taken in the city of Cuenca in Ecuador. The validity of the structure was tested using the exploratory factorial analysis (AFE), which suggests the presence of one factor, which is why we considered the evaluation of a bifactorial model with three specific dimensions and a general one. Later, using confirmatory factorial analysis (AFC) using the DWLS method and polychoric correlation matrices, we can observe the multidimensional factorial structure proposed by the original author (Keyes, 2009) of three factors and the structural validity of the model as done in other studies carried out in Polish contexts (Karaś et al., 2014), Chinese (Guo et al., 2015), Italian (Petrillo et al., 2015) etc. Also, this study performs confirmatory factor analysis (CFA) factors such as those presented in the study by Echeverría et al. (2007), observing that the bifactorial model presents good adjustment indicators.
The correlation between the three dimensions (social, emotional and psychological), is significant, empirically demonstrating Keyes’s theoretical proposal (2007) in his multidimensional vision of positive mental health or general wellbeing as it has been called in the study of Echeverria et al. (2007). The concept of positive mental health or general well-being includes, emotional well-being constituted of affections, positive high and negative low, psychological well-being, composed by self-acceptance, personal growth, purpose in life, mastery of the environment, personal autonomy and positive relations with others, and social welfare constituted by the social acceptance perceived by the subject, social updating (where the healthy subject relies on the future of society, in its potential growth of development and its capacity to produce welfare), social contribution, social cohesion and social integration.
In this research reliability models concerning Cronbach’s alpha and McDonald’s omega reach high values of internal consistency which coincides, at least regarding to Cronbach´s alpha, with most of investigations about the adaptation and validation of psychological questionnaires performed in different countries where the model is adequately adjusted (Guo et al., 2015). These results guarantee the use of this tool as part of the diagnostic and research evaluation in the Ecuadorian context.
At higher the mental health, the higher the well-being, and the higher mental health, the lower the negative emotions using the Negative Emotions sub-scale of the Perma Profiler scale of Buttler and Kern (2016), which coincides with results found in other research where mental illness and positive mental health are opposed (Petrillo et al., 2015).
The three factors do not follow a normal distribution according to the tests performed but an asymmetric negative distribution. The correlations between the welfare, social, emotional and psychological factors are significant for all combinations of the three factors, as Keyes points out in their multidimensional model of well-being (Keyes, 2002).
In the comparison of the individuals about sex with the three factors, it was found that the differences between men and women are significant, with women having higher values for the three dimensions. Other research on women’s well-being has also reported that women score higher in enhancing their abilities and personal development (Yañez & Cárdenas, 2010).
When analysing the results of individuals classified by age (early adulthood, middle adulthood and late adulthood) for each dimension of well-being, it is observed that the population in late adulthood has higher average values. The Kruskal-Wallis test shows that in all three dimensions of well-being there is a statistically significant difference between at least one pair of categories. The Dunn test shows that regarding emotional well-being, the difference in the median values between the late adulthood group and early adulthood; and late adulthood and middle adulthood is statistically significant, but the difference between early adulthood and middle adulthood is not. The same results are observed in the section on social welfare while in psychological well-being it is observed that all differences among all categories are statistically significant.
The elderly report higher mean and median scores on all wellbeing studied dimensions. On the one hand, it has been shown that older adults accumulate wisdom and focus on pleasurable events, friendships and experiences, although they must confront events such as death of loved ones, loss of active status associated with retirement, and health and income reduction (Lockenhoff & Carstensen, 2004). Also, middle-aged adults are motivated to earn income even at the expense of their well-being to achieve economic stability and well-being later in life (Steptoe, Deaton, & Stone, 2015). It is important to note that several elderly adults that participated in this study are also involved in various social service programs where active or successful ageing is promoted. The active aging model is based on the concept of life cycle with its gains, stability, and losses in middle age that are assumed in an adaptive way, and in the case of the elderly will be focused on the restructuring of free time, reinforce the feeling of being a useful part of society and, above all, to find new sources of social support (Jiménez, Lafuente, Hernández et al., 1999). The impact assessment of such social assistance programs is beyond the scope of this study.
This work attempts to overcome the methodological pitfalls of previous research by proposing models of exploratory, confirmatory factorial analysis, and the use of polychoric correlation matrixes since the adaptation and validation are substantial, and there is an increasing number of researchers that emphasise the importance of the valuation of the psychometric aspects of the instruments.
It is important to note that the total number of observations with which factor analyzes were performed (n = 550) may be the source of a sample bias (Ten Berge & Socan, 2004).
In conclusion, the Spanish version of MHC-SF (Keyes, 2009) is an appropriate tool to measure mental health and can be used in the Ecuadorian context for the evaluation of positive mental health according to the reliability and validity obtained in this studio.

