











 texto en
texto en  Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo

 Permalink
PermalinkIntroduction
In recent years Mexico has undergone diverse population changes marked by the increasing elderly population, which is expected to rise from 3.5 to 4.3% between 2000 and 2018. Population growth is projected to decline from 1.3 to 0.7% in the same period. In addition, the average life expectancy of Mexicans doubled during the second half of the twentieth century, from an average of 36 years in 1950 to an average of 74 years in 2000 [Alzheimer’s Disease International, 2009; Instituto Nacional de las Personas Adultas Mayores (INAPAM), 2011; Instituto Nacional de Estadística y Geografía (INEGI), 2014; Sistema Nacional de Vigilancia Epidemiológica (SNVE), 2011]
The growth in the elderly population has generated various health concerns, mainly because while most older adults in Mexico live in urban areas (approximately 54.8%), a significant proportion (45.2%) of the population live in mixed or rural locations, which may lead to greater difficulty accessing medical care. Furthermore, the elderly are increasingly living alone. Consequently, there is a lack of diagnosis and increased depression among the elderly (Alzheimer’s Disease International, 2009; INAPAM, 2011; INEGI, 2014; SNVE, 2011).
One of the consequences of the increasing elderly population in Mexico is increasing neurocognitive disorders such as Alzheimer’s Disease (AD). There are currently more than 350,000 cases throughout the country, with an annual incidence of 25.000 cases, and a mortality rate of 2.000 older adults each year. AD is characterized by premature and rapid death of neurons in specific brain areas, accompanied by behavioral and psychological changes, and a high probability of biological morbidities (INAPAM, 2011; INEGI, 2014; SNVE, 2011).
Depression has a prevalence of 51.7% in neurocognitive disorders in clinical samples, and 38.1% in community samples. It should be noted that depression, when associated with mild cognitive impairment (MCI), can enhance memory loss, and in turn may be associated with orientation, learning, and recognition difficulties, among others. In addition to severely affecting the capacity of the patient to perform basic activities of daily life, thus reducing their own and their caregiver’s quality of life and well-being (Aalten, De-Vugt, Lousberg, Korten, Jaspers, Senden, Jolles, & Verhey, 2003; Rothi, Raymer, & Heilman, 1997; Snyder, Jackson, Petersen, Khachaturian, Kaye, Albert, & Weintraub, 2011; Terrera, Brayne, & Matthews, 2010; Vidovich & Almeida, 2011).
Previous studies have shown that changes in short-term memory could explain 6.6% of the negative emotional states of anxiety and suffering; 3.4% of insincerity or inability to help others, and 1.9% of the inability to maintain values and unconventional ideas; changes in ability to focus could explain 3.4% of the experience of negative emotional states. Major personality changes include neuroticism, kindness, and openness to experience, from the Big Five Factor Theory (Rodrigues, 2015; Rodrigues, Castro, & Cruz Roja Española, 2014; Rodrigues, Castro, & Gruart, 2014).
Considering the data referred to above, we should note that these values do not indicate a cause and effect relationship, because we could reverse the positions and say that neuroticism explains 6.6% of short-term memory, but we also know that there is an undeniable relationship between these factors. Therefore, the objective of this work is to identify the level of relationship between depression and the cognitive functions of early-stage Alzheimer’s patients, considering that our hypothesis is based on the fact that the depression can increase the cognitive alterations in these patients (Rodrigues, 2015; Rodrigues, Castro & Cruz Roja Española, 2014; Rodrigues, Castro & Gruart, 2014).
Method
Participants
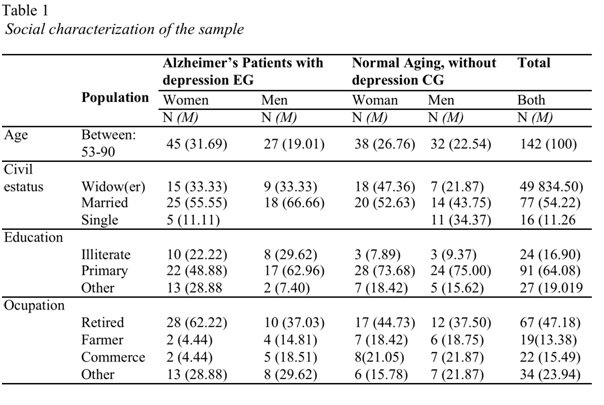
A total of 142 Mexican outpatients participated in this study. The sample was divided into two groups, the experimental group (EG) with 72 adults (27 men and 45 women) with a neurological clinical diagnosis of early-stage Alzheimer’s and a psychiatric diagnosis of depression. The control group (CG) included 70 adults (32 men and 38 women) experiencing normal aging and without psychiatric diagnosis of depression.
As inclusion criteria, for the EG the participants had to present a clinical diagnosis of Alzheimer’s endorsed for a neurologist and a clinical diagnosis of depression endorsed by a psychiatric. For the CG, the only inclusion criterion they had to present was that they did no suffer from any chronic severe, cognitive or depression illness, clinical endorsed by a family doctor. All patients had to be 50 years or older to participate in the research (table 1).
Questionnaires
Participants were evaluated individually through the application of the Beck Depression Inventory-II (BDI-II) and the Folstein Mini-Mental State Examination (MMSE), for cognition. The questionnaires were properly validated and were applied in accordance with their manuals (Beck, Steer, & Brown, 1996; Beck, Ward, Mendelson, & Erbaugh, 1961; Carmen, Freyre, & Hernández-Guzmán, 2012; Folstein, Folstein, & McHugh, 1975).
Procedure
Participants were evaluated at two different public health institutions in the city of Leon, Guanajuato. Evaluations were conducted in sessions of 50 minutes each, in a total of 142 sessions between February and June 2016. Participants were informed about the research, their participation was voluntary and corresponded to the ethical standards of confidentiality and anonymity, as well as the methodological criteria published by the American Psychological Association (APA), and the general law regarding health in Mexico.
Statistical analysis was performed with the Statistical Package for the Social Sciences (SPSS), version 13.3 for Windows, working with a level of significance calculated for values of p<.05.
Results
In the analysis of the multiple comparisons made between depression, as independent variable, and cognition in general, and cognitive factors of attention and immediate memory in particular, as dependent variables, the statistical test of Scheffé was applied in a Post Hoc analysis using a 95% confidence interval.
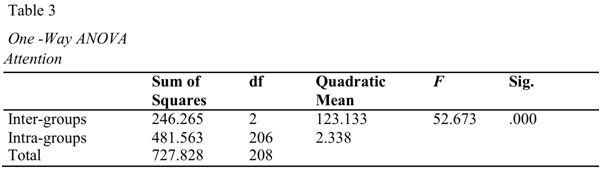
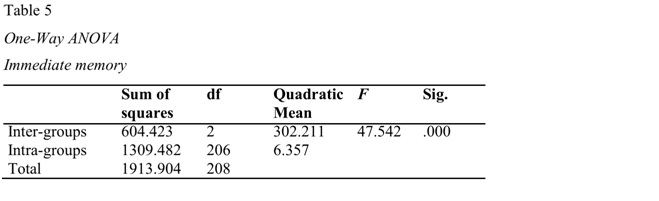
Whereas, for cognitive factors of attention and immediate memory, the one-way ANOVA variance analysis was applied, in order to know if measures of cognitive factors of attention and immediate memory were different between levels of depression.
For a more objective analysis of the results we decided to analyze the MMSE from its factorial division, respecting the dimensions of its theoretical construct: spatial orientation, temporal orientation, immediate memory, attention, calculation, delayed memory, visoconstructive capacity, and language (table 2).
Table 2: Relationship between depression and cognition, using cognition as a dependent variable Scheffé
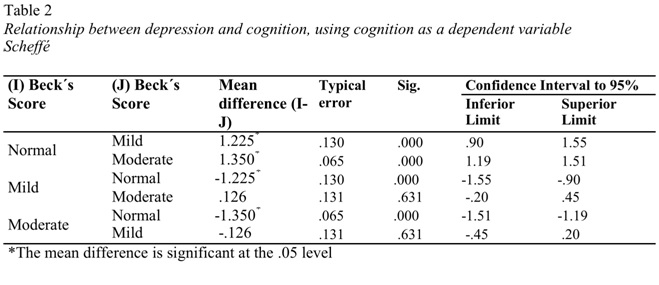
In the Post Hoc analysis, significant differences were obtained for the groups of mild-normal depression and normal-moderate depression, with the scores obtained in the category of Mini Mental cognition, that is to say that the two variables are related. It is seen that p> 0.05 in the mild-moderate depression group, this means that there are no significant differences in the diagnostic category scores of cognition relative to the group with mild-moderate depression.
Thus, overall scores between the Beck Depression Inventory values and the Mini Mental scores have 2 statistically significant values. Immediate memory and attention are exhibited as a casual factor that accounts for 23.4% of the depressive state. Cognition presented significant changes supporting cognitive limitations when associated with depressive comorbidity.
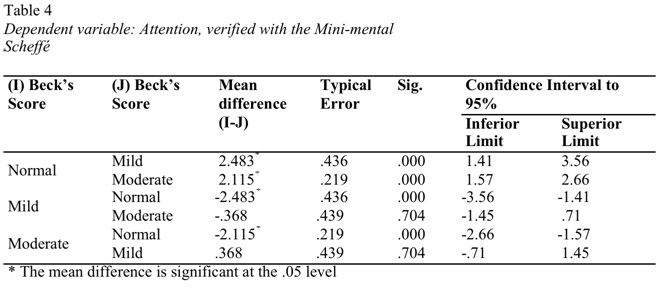
With the Post Hoc analysis of ANOVA, statistically significant differences were found in the attention scores p <.05, between the normal- mild to moderate and moderate-to-moderate groups, whose score is p=.000. The scores F=52.673, gl =2 and p=.000 (tables 3 and 4).
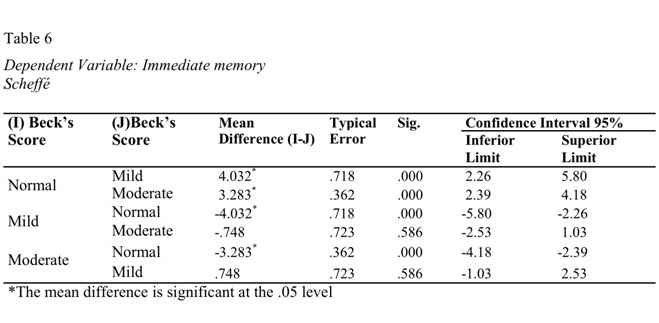
In the case of immediate memory, a significant difference was found between the groups of mild - normal depression, p=.000, normal - moderate, p=.000, but there were no significant differences Among the mild-moderate groups, p=.586. The coefficient F=47.542, gl=2 and p=.000 (tables 5 and 6).
Discussion
We initially referred to some studies with Alzheimer patients showing changes at the cognitive level where immediate memory and attention account for 6.6% and 3.4%, respectively, of the experiences of negative emotional states of anxiety. In this research, when we associate the depression to cognitive changes, we found that depression explained 23.4% of the experiences of negative emotional states through alterations in short-term memory and focus. A significant increase in itself. However, in previous research, the barometer of measurement has been the personality traits of the Big Five Factors (Rodrigues, 2015; Rodrigues, Castro, & Cruz Roja Española, 2014; Rodrigues, Castro, & Gruart, 2014).
In this study, we found that 23% of cognitive change is caused by depression, which can be categorized into three different structures, not considering the use of personality traits, instead applying an internal subcategorization of the Beck depression inventory. We grouped depression into its specific factors: nine cognitive-affective factors and two somatic factors that explain 23,4% of short-term memory; six cognitive-affective factors and one somatic factor that explained the same 23,4% of attention (Rodrigues, 2015; Rodrigues, Castro, & Cruz Roja Española, 2014; Rodrigues, Castro, & Gruart, 2014).
It is important to verify the direction of the relationship in the work conducted on personality thresholds, this relationship could be bilateral, i.e., short-term memory could explain the experience of negative feelings, but negative feelings may also explain the changes of short-term memory. Thus, we verify that the direction, at least with depression, is unilateral. Depression explains the cognitive changes of short-term memory, not the reverse (Rodrigues, 2015; Rodrigues, Castro, & Cruz Roja Española, 2014; Rodrigues, Castro, & Gruart, 2014).
There are, in our view, three major conclusions. First, depression generates changes in cognition to a quite significant degree, at least in terms of short-term memory and focus. Second, that the depression/cognition relationship is bilateral, which means that depression can cause cognitive changes, but that cognitive disorders can also cause depression. And third, that changes in short-term memory and focus can be confused with personality changes, as well as increasing dementia.
In any case, this work reinforces the most important principle of intervention with older adults: the need for an excellent evaluation, to be able to apply the most appropriate intervention program possible to the limitations presented by the elderly with early-stage AD. It should be noted that the two factors evaluated can be associated: depression and personality changes in AD, which can further enhance the changes to the level of short-term memory and focus.
Finally, although aging may be the result of genetic programming, normal biological processes necessary for life, or even the outcome of key determinants of longevity genes, in many cases there is comorbidity of aging with depression. However, Geriatric Depression may also be associated with other comorbidities such as myocardial infarction, diabetes, degenerative dementia, and cerebral vascular disease, or different symptoms such as anxiety.
The findings lead us to place to greater emphasis on psychological evaluation, considering that each elderly individual will experience a unique aging process, which cannot be generalized or easily compared to any other individual. Similarly, when aging is accompanied by AD, in addition to being a degenerative disease, its development is random, turning the symptomatologic tables into chaos.

