











 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo

 Permalink
Permalink
The United Nations 2030 Agenda reinforces the importance of healthy work environments and worker well-being for productivity and public health (United Nations, 2020). Well-being is a central focus of Positive Psychology (Seligman, 2012), which seeks to understand happiness and to broaden the concept of health, adaptation, creativity, and emotional fulfillment (Faria, 2020). According to the World Health Organization (WHO, 2010, 2020), employee well-being is essential for organizational competitiveness. Organizations that prioritize well-being experience greater employee retention, productivity, and sustainability, with positive impacts on performance, communities, and the global economy. It is estimated that 160 million workers develop occupational illnesses annually, and that 8% of depression cases are related to occupational hazards (WHO, 2010).
Teams are the strategic foundation of organizations (Souza et al., 2015). For teams to act effectively, it is essential that they are healthy and motivated. Among the strategies for empowering teams, Psychological Capital (PsyCap) stands out as a Positive Psychology resource that enhances motivation, resilience, and goal achievement (Luthans et al., 2007). Luthans et al. (2015) define PsyCap as a psychological state composed of self-efficacy to overcome challenges, optimism regarding present and future success, hope to pursue goals and adjust pathways when necessary, and resilience to withstand adversity and achieve success. These resources interact synergistically, influencing cognitive, affective, and behavioral functioning. Their common underlying factor is the cognitive capacity to positively evaluate situations and sustain motivated effort (Youssef-Morgan & Luthans, 2011). PsyCap is therefore considered a key resource for helping workers overcome challenges and achieve goals, offering a competitive advantage to organizations (Luthans et al., 2004; Rodrigues, 2022).
PsyCap is associated with improved performance, life satisfaction, and psychological well-being (Darvishmotevali & Ali, 2020; Kim & Yoo, 2018); and it also contributes to the creation of healthy work environments and positive workplace relationships (Caza et al., 2009). Haleem et al. (2017) highlight its relevance in professions involving direct contact with the public, as it supports the management of adversity and the adoption of behaviors that reduce stress and exhaustion. Importantly, PsyCap can be developed through targeted interventions (Luthans et al., 2006), and is recognized as a key resource for healthcare organizations seeking to promote a culture of excellence and sustainability (Caza et al., 2009).
Since its introduction, several PsyCap development interventions have been proposed. The first, the Psychological Capital Intervention (PCI), was developed by Luthans et al. (2006) and later refined by Luthans et al. (2010). Its effectiveness was subsequently confirmed in different contexts (Russo & Stoykova, 2015). Later studies further reinforced the effectiveness of PsyCap interventions, showing that PsyCap development increases positive psychological states, reduces negative states, improves well-being, and strengthens work-related coping skills (Demerouti et al., 2011; Luthans et al., 2006; Luthans et al., 2010; Luthans et al., 2014).
Despite advances in the development of PsyCap interventions, important gaps in implementation and reporting practices remain. The review conducted by Ruiz et al. (2025) identified substantial variability in intervention contexts, formats, and durations, often tailored to participants’ and organizations’ needs, and reported consistent benefits for well-being and performance, particularly in emotionally demanding contexts. However, the authors highlighted a common limitation: the lack of clear and standardized descriptions of session content, which hampers replication and standardization across programs. Converging evidence was reported by Salanova and Ortega-Maldonado (2019), whose integrative review showed that PsyCap interventions generally increase PsyCap and improve outcomes such as performance, work attitudes, and well-being, with effects sustained over time. Nevertheless, recurring weaknesses were identified, including methodological limitations, wide variability in follow-up periods, and the predominance of studies conducted in Western contexts, underscoring the need for more rigorously structured and transparently reported interventions.
To address these gaps, the present study proposes the PsyCap Promotion Intervention Program (PIPP), an intervention grounded in validated theoretical models and empirically supported techniques, offering a clearly defined and structured approach to the systematic development of PsyCap. In their review, Ruiz et al. (2025) further highlighted that Youssef-Morgan and Sundermann (2014) defined four essential criteria for effective PsyCap interventions: (1) generate outcomes attributable to the intervention, (2) modify adaptive characteristics, (3) outperform conventional programs, and (4) ensure a positive return on investment. The review found that only the first two criteria were met, underscoring the need for interventions that fulfill all four criteria (Ruiz et al., 2025). The general objective of this study was to describe the PIPP development methodology, as well as to present a theoretical and practical synthesis of its structure. The specific objectives of this study are to: (1) describe the objectives and target audience of the PIPP, (2) outline the pedagogical and operational guidelines for trainers, (3) describe the program’s ethical considerations and potential risks, (4) describe the content delivery methods, (5) present the theoretical model underpinning the PIPP, (6) describe the program structure and sessions, and (7) outline the program’s implementation and evaluation plan.
This manuscript reports the development and description of an intervention, presenting its conceptual framework, design, and implementation protocol, without reporting results from its implementation, which will be examined in a subsequent empirical study. The reporting of the intervention development was guided by the Guidance for Reporting Intervention Development Studies (GUIDED) checklist (Duncan et al., 2020).
PIPP Development Methodology
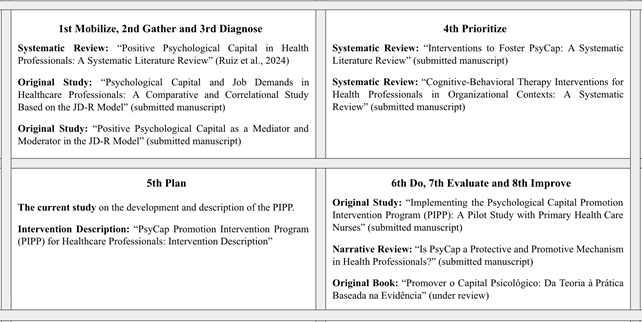
The development of the PIPP was evidence- and theory-based and guided by the World Health Organization Healthy Workplace Model, which provides a comprehensive and adaptable framework for planning, implementing, and evaluating workplace interventions, with an emphasis on continuous improvement. This model comprises eight sequential steps: mobilize, gather, diagnose, prioritize, plan, implement, evaluate, and improve (WHO, 2010). The execution of these steps resulted in a structured program of research, including three systematic reviews and two empirical studies that informed the theoretical, empirical, and methodological foundations of the PIPP. As illustrated in Figure 1, this process not only supported the planning and development of the intervention described in the present study but also gave rise to subsequent research outputs, situating the PIPP within a coherent and cumulative research framework.
Description of the Intervention
Objective and Target Audience
The PIPP aims to promote and develop the PsyCap of health professionals in public and private organizations by enhancing self-efficacy, optimism, hope, and resilience. Furthermore, the program was designed with a structure that includes: (1) three distinct points of effectiveness evaluation, (2) cost-benefit analysis, including return on investment (ROI) and cost indicators such as presenteeism, and (3) a systematized methodology that ensures replicability across different contexts.
This program is based on the premise that strengthening individual PsyCap may contribute to the development of group PsyCap, which reflects the shared psychological state of teams and emerges from interaction and communication among members. The greater the interaction, the stronger the group’s psychological components (Santos, 2021). Bogler and Somech (2019) reinforce this view by stating that teams operating in shared contexts tend to develop shared mental models. Nunes’ perspective (Nunes, 2017) was also considered, which emphasizes that health work contexts are privileged spaces for continuous training. Thus, the PIPP aims not only to develop PsyCap but also to facilitate the practical application of the knowledge acquired in professionals’ daily work routines.
When implementing the PIPP for different professional groups, it is recommended to separate participants according to their professions, considering distinct responsibilities and challenges (Yang et al., 2020). This personalization enhances the relevance, effectiveness, and perceived benefits of the PIPP for participants.
Theoretical and Conceptual Framework: JD-R and Psychological Capital in Healthcare Organizations
The JD-R model, proposed by Demerouti et al. (2001), has become one of the leading frameworks in occupational health psychology and human resource management. It is widely applied across organizations and supported by extensive empirical evidence (Ahmed et al., 2021; Bakker & Demerouti, 2017). Its main contribution lies in its comprehensive approach, integrating job demands and job resources rather than focusing exclusively on risk and stress. Initially developed to explain emotional exhaustion, the model has evolved into a flexible framework that accounts for employee well-being, work engagement, and performance (Bakker & Demerouti, 2007, 2014; Bakker et al., 2023). Over time, this model has been consolidated as a theory through a set of core theoretical assumptions, currently comprising nine premises: flexibility, dual processes, job demands-job resources interactions, personal resources, resources moderation, job crafting, gain cycles, self-undermining, and loss cycles (Bakker et al., 2023). Within this framework, PsyCap is embedded in the fourth premise, which conceptualizes personal resources as positive self-beliefs or self-evaluations linked to individuals’ perceived control over, and impact on, their work environment (Bakker et al., 2023).
The JD-R theory not only explains occupational well-being processes but also informs the development of evidence-based workplace interventions. Grounded in the assumption that employees play an active role in shaping their work environment and that organizations should invest in their development to strengthen personal resources, the JD-R framework emphasizes interventions that support adaptation to job demands and foster professional growth (Bakker & Demerouti, 2014). Accordingly, PsyCap represents a particularly suitable construct for operationalizing the JD-R resource-based intervention pathway at the psychological level. JD-R-based interventions are typically grouped into four main categories-job redesign, job crafting, training, and strengths-based approaches-differing in level (individual vs. organizational) and intervention target (work conditions vs. personal resources; Bakker & Demerouti, 2014). Within this framework, the PIPP fits as an intervention aimed at strengthening personal resources, combining strengths-based approaches at the individual level with training at the organizational level (Bakker et al., 2023). Although not originally defined as a distinct JD-R intervention category, the PIPP can be understood as a practical application of the JD-R model, particularly in promoting personal resources.
Considering the framework proposed by the JD-R model, strengthening individual psychological resources within organizational contexts plays a central role in work adaptation and the protection of mental health, particularly when such contexts are characterized by high demands and structural changes over which employees have little control (Almeida, 2014; Chintalapti, 2021). Healthcare professionals operate in organizational contexts marked by high emotional demands, time pressure, ethical responsibility, and continuous exposure to human suffering-factors that significantly increase vulnerability to stress, emotional exhaustion, and other psychosocial risks (Almeida et al., 2020; Izdebski et al., 2023). These risks stem from organizational, managerial, and psychosocial working conditions and negatively affect both the physical and mental health of professionals, as well as the functioning and productivity of healthcare organizations (Almeida et al., 2020; Claudino et al., 2024). Evidence indicates that work environments characterized by high workloads and adverse conditions are associated with poorer performance, lower work engagement, higher turnover, increased absenteeism, and compromised quality of care, thereby threatening the sustainability of healthcare systems (Secosan et al., 2021).
Within this context, the PsyCap, composed of four core psychological capacities-hope, efficacy, resilience, and optimism-commonly referred to by the acronym HERO, stands out as a trainable psychological resource that goes beyond individuals’ current functioning, also reflecting their potential for development (Luthans et al., 2006). Professionals with higher levels of PsyCap tend to interpret job demands more positively, perceive greater control over situations, and respond more effectively to challenging environments, thereby reducing the risk of stress and emotional exhaustion (An et al., 2020; Santos et al., 2019). In the healthcare sector, higher levels of PsyCap have been associated with greater work engagement, better performance, enhanced well-being, and stronger intentions to remain in the organization, contributing to healthier and more sustainable work environments (Lupșa et al., 2020; Secosan et al., 2021; Viseu, 2017). Therefore, interventions aimed at developing PsyCap are particularly suitable for healthcare organizational contexts, especially when implemented in a structured manner, with organizational support and under conditions that foster participation, psychological reflection, and the practical application of the skills developed.
Theoretical Model of the PIPP and Associated Theories
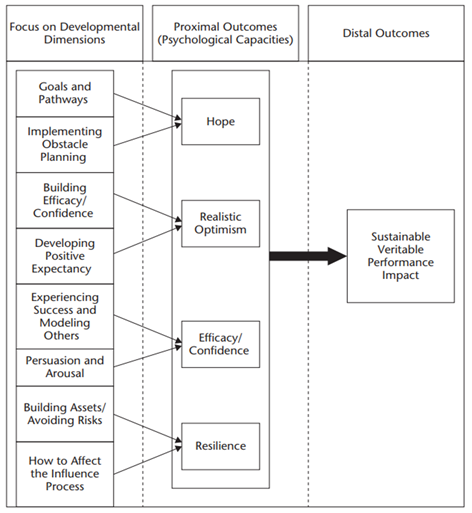
The development of the PIPP followed the guidelines of the Portuguese Order of Psychologists (OPP), adapting recommendations for preventive interventions to a skills development program. These guidelines recommend that programs be grounded in empirically validated theoretical models, ensuring consistency between objectives, processes, and outcomes (Matos, 2017). The theoretical model underlying the PIPP is based on the definition of PsyCap proposed by Luthans et al. (2015) and on the PCI framework (Luthans et al., 2006; Figure 2).
The PCI was developed in 2006 as an online micro-intervention consisting of two-hour workshops. The authors administered the Psychological Capital Questionnaire (PCQ-24; Luthans et al., 2007) and found a significant increase in PsyCap. In 2010, the intervention was replicated, yielding similarly positive effects (Luthans et al., 2010). The intervention guidelines were based on the PsyCap dimensions and grounded in clinical psychology (hope and resilience), attribution and expectancy theories (optimism), and Bandura’s theory (self-efficacy; Bandura, 1997). Each dimension was developed through specific exercises: (1) hope: goal focus and a proactive mindset, (2) self-efficacy: goal setting and positive feedback, (3) resilience: anticipating obstacles, and (4) optimism: reframing negative thoughts. These exercises were followed by writing, reflection, and group discussion activities, as well as the formulation of personal goals and strategies to overcome potential barriers. The results confirmed that developing PsyCap provides a competitive advantage and improves job performance (Luthans et al., 2006; Luthans et al., 2010).
This theoretical grounding in the PCI was corroborated by the review conducted by Ruiz et al. (2025), which found that 81.81 % of the analyzed articles used it as a theoretical anchor. Within this model, each PsyCap component is supported by specific theories: hope, by Snyder et al.’s Theory of Hope (Snyder et al., 1991); self-efficacy, by Bandura’s social cognitive theory; resilience, by Ann Masten’s work in positive psychology; and optimism, as conceptualized by Youssef-Morgan and Luthans (2011) within the field of positive psychology. The theoretical definitions of each resource were used to structure the practical activities.
Russo and Stoykova (2015) followed the PCI guidelines and implemented an intervention consisting of four exercises: (1) defining Specific, Measurable, Attainable, Relevant and Time-bounded (SMART) goals (hope), (2) identifying realistic goals and obstacles (hope and self-efficacy), (3) establishing subgoals (resilience), and (4) recognizing individual and contextual resources (resilience). In addition, the intervention included a constructive feedback activity and small-group brainstorming sessions (four to five participants) focused on positive thinking (self-efficacy and optimism). The PCQ-24 (Luthans et al., 2007) was administered at three time points: before the intervention, immediately after, and one month later.
As with the PCI, the PIPP sessions were structured to develop each PsyCap component separately. The selected activities are empirically supported, drawing on evidence from the PCI, the study by (Russo & Stoykova, 2015), and the review by Ruiz et al. (2025), which identified effective content delivery methods such as structured reading materials, positive feedback techniques, goal setting and achievement, PowerPoint presentations, videos, mindfulness, and practical exercises. The review also considered specific empirical studies, including Gon et al. (2023), conducted with nurses, and Zeng et al. (2023), which incorporated mindfulness and reported benefits for self-efficacy, hope, and resilience.
Consistent with its theoretical foundations, the PIPP adopts a content delivery approach that integrates theoretical exposition (oral presentations) with participatory techniques, such as role-playing, to promote active interaction between trainers and participants (Matos, 2017; Nunes, 2017). In line with PsyCap development principles, the program also incorporates experience-based learning strategies, including guided reflection on lived experiences (Bonvalot, 1991) and vicarious learning through observation and group exchange (Russo & Stoykova, 2015).
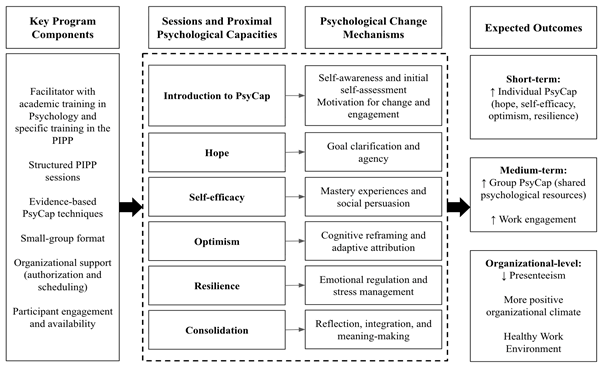
In addition, the activities were informed by Cognitive Behavioral Therapy (CBT) techniques selected according to the theoretical foundations of each PsyCap resource and drawn from the book 101 CBT Techniques (Conceição & Bueno, 2020). In total, eight techniques were selected: Wheel of Life (Sachweh & Conceição, 2020), Making Decisions (Nepomuceno & Conceição, 2020), Rational-Emotional Role-Play (Rudey & Conceição, 2020), Relaxation (Karvat & Conceição, 2020), One Minute Meditation (Rodrigues & Conceição, 2020), Reformulation of Mental Images (Paulitisky & Conceição, 2020), Gratitude Box (Conceição, 2020), and Criticism Circle (Hiera & Conceição, 2020). To integrate the theoretical foundations of PsyCap with the structure and objectives of the PIPP, a logic model was developed (Figure 3).
Theoretical Anchoring and Session Description
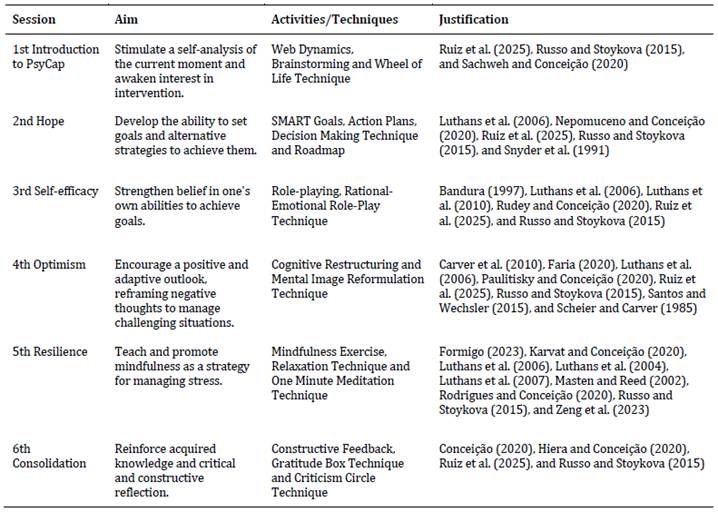
Based on the PCI and the review by Ruiz et al. (2025), it was found that PsyCap components can be addressed in individual sessions. The review identified an average of five sessions; however, the PIPP was structured into six sessions by including an introductory session and a consolidation session (Table 1). The review also indicated that sessions lasted an average of 77 minutes and that the intervention spanned a total of six weeks (Ruiz et al., 2025).
In the PIPP, sessions are planned to occur weekly, with a duration of 60 to 90 minutes, and are designed to be delivered in a mixed method format. Intervention sessions are conducted in person, whereas assessment procedures and session summaries are delivered online. Each session is held in small groups (four to five participants), encouraging attention and active listening (Russo & Stoykova, 2015). The program targets health professionals working in public or private healthcare organizations. Inclusion criteria include active professional practice in a healthcare setting and availability to attend the scheduled sessions. Exclusion criteria are limited to professionals not currently working in healthcare contexts or individuals unable to participate in group-based activities at the time of implementation.
Sessions are delivered in small groups to promote interaction, social support, experience sharing, and vicarious learning, while also being time- and cost-efficient. However, this format presents challenges, such as managing time to accommodate all groups and respond to individual needs (Nunes, 2017), making the presence of psychologists essential.
Guiding Guidelines for Trainers
We recommend carefully reading the book Promover o Capital Psicológico: Da Teoria à Prática Baseada na Evidência, which details the step-by-step implementation of the PIPP. The book includes a participant manual divided into six sections corresponding to the program sessions. It will be available for purchase and can also be requested via email (manualpipp@gmail.com). The implementation of the PIPP should follow the structure presented in the book, ensuring that all program components are systematically addressed. This approach maximizes the program’s impact and facilitates the monitoring and evaluation of outcomes. Moreover, this structured framework reinforces transparency and the responsibility of each trainer to deliver the program as intended.
This book was developed considering several factors that influence the effectiveness of the PIPP, including participant individuality (motivation, skills, and prior knowledge), program structure (methods, environment, and duration), and trainer profile (competence, experience, and mastery of content). To address these factors, detailed support materials are provided to guide and prepare trainers, ensuring an efficient and well-organized implementation. This emphasis is particularly important, as a well-prepared trainer can significantly enhance participant engagement (Nunes, 2017).
Ethical Considerations and Potential Risks
Ethics are fundamental in intervention programs. Although there is no specific ethical code governing this type of intervention, Nunes (2017) highlights a set of guidelines whose application depends largely on the trainer. Accordingly, trainers must hold a degree in Psychology (given the theoretical foundations of the PIPP), adopt an ethical stance, and clearly present their qualifications and the program’s objectives without making promises regarding outcomes. Although the PIPP is implemented in a group format and employs psychological techniques, it does not constitute a clinical group therapy intervention, nor does it aim to treat psychological disorders or mental pathologies. The PIPP was designed as a structured preventive and developmental intervention focused on the promotion of individual competencies and the strengthening of trainable positive psychological capacities. Rather than functioning as a therapeutic setting, it serves as a space for sharing and developing skills, free from judgment or imposed change (Nunes, 2017).
If the program evaluation is conducted as a research project, it is essential to adhere to additional ethical principles, namely compliance with the Declaration of Helsinki. The implementation of the PIPP is expected to lead to a more productive and positive work environment; however, challenges may arise, such as initial resistance and variability in effectiveness among participants. These differences may depend on factors such as openness to the change process, pre-existing stress levels, and the dynamics of the groups in which the program is implemented.
Program Application (Evaluation Phases and Moments)
The PIPP was structured to be applied in three distinct phases (Table 2).
Table 2: PIPP Application Phases
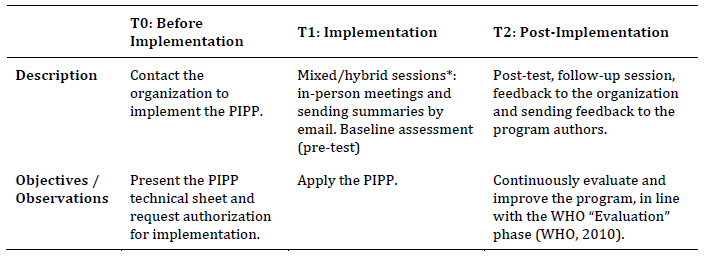
Note: *According to Carter and Youssef-Morgan (2022), there are no clear advantages to fully online interventions, which justifies the choice of a hybrid/mixed approach to increase the effectiveness of the intervention.
PIPP assessments involve the application of the same protocol across three distinct phases (pre-test, post-test, and follow-up), using validated instruments to psychometrically measure the variables under study. Trainers are responsible for authorizing and purchasing the questionnaires. Assessments should be conducted online using platforms such as Google Forms or EuSurvey, except in cases where participants experience difficulties accessing the online protocol. From an evaluation design perspective, the PIPP is conceived as a structured intervention that can be assessed using a pre-test-post-test design with follow-up measurements. Depending on the objectives, context, and resources of each implementation, evaluation designs may range from single-group longitudinal assessments to quasi-experimental or experimental designs that include control groups and randomization. When feasible, the inclusion of comparison or control groups is recommended to strengthen causal inference. Statistical analyses may include within-group comparisons across assessment time points (pre-test, post-test, and follow-up), as well as between-group analyses in designs involving experimental and control groups. Decisions regarding randomization, sample allocation, and longitudinal follow-up should be aligned with the specific research or practice goals of each implementation, as well as with ethical and organizational constraints.
Each assessment point is designed to capture different aspects of change across the intervention process and involves specific procedures and measurement instruments. Pre-testing is essential for identifying baseline PsyCap levels (and other variables) prior to the intervention and is administered during the first session. The recommended instrument is the PCQ-24 (Luthans et al., 2007), using the validated version appropriate to the country in which the program is implemented. This instrument was adopted in 80 % of the studies in Ruiz et al. (2025) due to its validity, reliability, and internal consistency (α = .89 to .93; Ruiz et al., 2024), as well as reverse scoring that reduces common method bias (Sharp, 2019). The assessment may be complemented with additional instruments, such as the Utrecht Work Engagement Scale (UWES-9; Schaufeli & Bakker, 2003).
It should be noted that extensive assessment protocols may lead to participant fatigue. Therefore, when additional questionnaires are included, the use of twelve-item versions is recommended, such as the Compound Psychological Capital Scale (CPC-12; Lorenz et al., 2016); or the revised Compound PsyCap Scale (CPC-12-R; Dudasova et al., 2021). The application of a PsyCap measurement instrument is mandatory, as without an adequate baseline assessment it is not possible to accurately evaluate the effectiveness of the intervention (Matos, 2017). Data analysis must be conducted rigorously, ensuring participant confidentiality and the ethical use of information to assess the program’s impact.
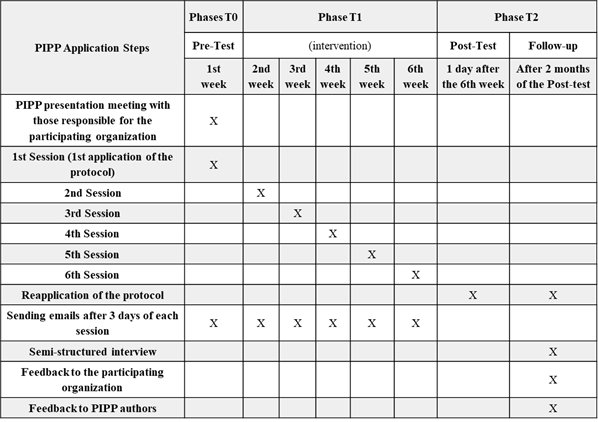
The post-test should be conducted during the sixth session or on the following day, using the same assessment protocol to measure the program’s immediate impact. Follow-up assessment should take place between 15 and 60 days after the sixth session, depending on organizational availability. This phase includes a reapplication of the protocol and a semi-structured interview, conducted either in person or online. The interview questions are provided in the PIPP book. This reassessment interval aims to capture longer-term behavioral and psychological changes and is consistent with the findings reported by Ruiz et al. (2025), who identified an average follow-up period of approximately seven weeks after the post-test. It also aligns with recommendations from Lally et al. (2010), and Stratman and Youssef-Morgan (2019), which suggest that a period of 21 to 66 days is appropriate for observing meaningful behavioral change.
These assessment points are essential for verifying the first three criteria proposed by Youssef-Morgan and Sundermann (2014). The fourth criterion can be addressed through the analysis of presenteeism and/or the calculation of return on investment (ROI; Martin et al., 2009; Read, 2024). Presenteeism can be assessed using different methods, including validated instruments such as the Stanford Presenteeism Scale (SPS-6; Koopman et al., 2002), by comparing scores across assessment periods. ROI assessment requires the identification of all relevant costs (e.g., development, training, operation, and maintenance) and the analysis of associated benefits. ROI is calculated using a standard formula and expressed as a percentage, where positive values indicate a net benefit and negative values indicate a loss. In the context of the PIPP, costs may correspond to the number of hours professionals are absent from work during program participation. When the trainer is internal and no confidentiality conflicts exist, it is also recommended to include absenteeism as a cost indicator. Figure 4 presents the planned timeline for the PIPP.
Final Considerations
The development of structured intervention programs aimed at healthcare professionals has the potential to generate meaningful benefits at both individual and organizational levels. The PIPP was designed to promote positive psychological development by strengthening core components of PsyCap, namely self-efficacy, hope, optimism, and resilience. Through the integrated development of these psychological resources, the program is expected to support adaptive cognitive, emotional, and behavioral functioning, particularly in demanding and high-pressure work contexts.
Beyond its promotive focus, the PIPP is conceptually aligned with preventive approaches to occupational stress and emotional exhaustion. By enhancing PsyCap, healthcare professionals may become better equipped to proactively manage work-related demands and psychological strain, thereby potentially reducing vulnerability to mental health problems. At the managerial level, higher PsyCap may contribute to more adaptive coping and leadership behaviors, as well as to the fostering of a more positive organizational climate, which in turn can support engagement, well-being, and sustainable work performance. However, these expected outcomes should be interpreted as theoretically grounded projections rather than empirically confirmed causal effects.
Importantly, the effectiveness of the PIPP depends on participants’ active engagement and the consistent application of the strategies and techniques developed during the sessions. Without the integration of these skills into daily professional practice, sustained gains in PsyCap are unlikely. Moreover, the program may be less effective under certain conditions, such as extreme workloads, insufficient organizational support, misalignment with organizational culture, or limited managerial endorsement. These contextual and organizational factors should be carefully considered when planning and implementing the intervention.
A key limitation of the present work is that the PIPP was not evaluated in this article through controlled effectiveness studies. However, it is important to note that the development of this intervention led to its implementation in a real-world context, carried out as part of an effectiveness study conducted with primary healthcare professionals in Portugal, the results of which will be reported in a future publication. Beyond this study, further effectiveness and implementation research is recommended, to be conducted by other authors across different organizational and cultural contexts. Such studies will allow the examination of the generalizability of the PIPP’s effects and the comparison of outcomes across contexts, populations, and implementation strategies, contributing to its refinement and external validation. Future research should examine within-group changes over time and between-group differences, as well as identify mechanisms of change and contextual moderators. Hybrid effectiveness-implementation studies may be particularly useful to understand not only whether the PIPP is effective, but also how, for whom, and under which organizational conditions it produces the best outcomes.
Overall, the PIPP represents a theoretically grounded and structured intervention proposal for the development of PsyCap in healthcare contexts. Its adaptability allows for application across different professional groups and organizational settings, provided that its core structure, session sequence, and objectives are preserved. Empirical evaluation therefore represents the next critical step to substantiate its proposed benefits and inform future refinements of the program.

