











 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Curriculum ScienTI
Curriculum ScienTI
 Permalink
Permalink
People of all ages, genders, ethnicities, socioeconomic backgrounds, and nationalities consume alcohol, and consumption patterns vary for a range of reasons (Ilhan & Yapar, 2020). Among those who consume alcohol, young people are often considered more vulnerable to harmful use, particularly binge drinking, which is defined as consuming four or more drinks on a single occasion for women and five or more for men (Waddell et al., 2021).
In Brazil, estimates from 2021 indicate that young people - particularly those aged 18 to 34 - were the most affected by hospitalizations and fatalities resulting from traffic accidents in which alcohol was involved (Centro de Informações sobre Saúde e Álcool, 2023). Within this age group, university students emerge as a particularly vulnerable population (Cortés-Tomás et al., 2022).
High alcohol consumption is common in this group (Merril et al., 2023), with studies showing that college students tend to drink more than their non-college peers and the general population (Sancerni-Beitia et al., 2020; Yoo et al., 2020). The consequences of this behavior can significantly affect students’ health and survival, including various types of accidents (especially traffic-related), unprotected sex, increased risk of liver disease, depressive symptoms, stomach pain, and legal problems, among others (Aboagye et al., 2021).
In Brazil, research on alcohol consumption among college students has primarily focused on factors associated with increased use, that is, variables that encourage consumption (Rebonatto, 2019). However, given the complex and multifactorial nature of alcohol consumption, it is equally important to analyze and understand the psychological variables that may be associated with reduced or controlled drinking in this population.
From this perspective, an important aspect to consider is the motivation to stop or reduce alcohol consumption; that is, the reasons that may lead individuals to discontinue or moderate their use (Conde et al., 2017). Although such research is essential for informing effective interventions, studies on these factors remains scarce in Latin America (Conde et al. 2016). Furthermore, no psychological instruments with strong psychometric properties have been identified to assess these motivations, which limits professionals’ ability to plan adequate interventions to address the specific needs of this population (Conde et al., 2017).
To address this gap, Conde et al. (2016) developed the Motivos para Cesar o Reducir el Consumo de Alcohol (MCR-A) scale (Reasons to Stop/Reduce Alcohol Consumption). The instrument consists of 20 items assessing reasons for reducing alcohol consumption and 20 items assessing reasons for stopping alcohol consumption. Each set is structured around three factors: (F1) Rechazo del alcohol (Rejection of Alcohol), (F2) Salud y cambios vitales (Health and health changes), and (F3) Consecuencias severas (Severe consequences). The MCR-A was validated with a sample of 377 first- and second-year psychology students at the National University of Mar del Plata, Argentina. The results demonstrate good internal consistency for both constructs: stopping consumption (Factor 1: α = .66; Factor 2: α = .74; Factor 3: α = .86) and reducing consumption (Factor 1: α = .67; Factor 2: α = .71; Factor 3: α = .86), as well as adequate goodness-of-fit indices for both sets of items: reasons to reduce (χ²(153) = 1118.25, CFI = .96, TLI = .95, RMSEA = .04, SRMR = .05) and to stop alcohol consumption (χ²(14) = 1146.42, CFI = .92, TLI = .91, RMSEA = .07, SRMR = .07).
The current context presents a challenge to reducing excessive alcohol consumption in university settings (Ferreira Alves et al., 2021). In this regard, the availability of a psychological instrument to assess individuals’ reasons for reducing or stopping alcohol consumption is highly relevant. Such a tool can provide useful and valid information to support the development of targeted interventions and health care programs for this population (Beard et al., 2017).
Although the MCR-A demonstrated good internal consistency and adequate goodness-of-fit indices in the original sample (Conde et al., 2016), replicating these results in a new population is essential to confirm its applicability and external validity. This involves examining whether the factor structure identified in the original study remains consistent when applied to a different cultural and social context (Souza et al., 2017).
Given the particularities of the Brazilian context, adapting and analyzing the validity and reliability of the MCR-A scale may contribute to identifying relevant psychological variables associated with the reasons for reducing or stopping alcohol consumption among university students. Therefore, this study aimed to adapt and evaluate the psychometric properties of the MCR-A for use in Brazil. The following hypothesis (H1) was proposed: the factorial structure of the MCR-A will consist of three factors for both reasons for stopping and reducing alcohol use, as observed in the original version of the scale.
Method
This study employed a non-experimental, cross-sectional, and correlational (ex post facto) psychometric design.
Participants
A non-probabilistic convenience sample was used, consisting of 334 university students with a mean age of 22.9 years (SD = 4.20). The majority were female (67.7 %), of mixed race (44.0 %), single (85.9 %), and Catholic (47.0 %). Most participants reported initiating alcohol use before entering college (84.4 %), with first consumption occurring between the ages of 15 and 20 (58.4%). All undergraduate students who reported any alcohol use and voluntarily completed the study instruments were included.
Classic recommendations indicating a minimum of 10 participants per item as adequate in factor analysis were considered when estimating the sample size (Hair et al., 2009; Tabachnick & Fidell, 2013). The study sample met this criterion, as each construct included 20 items, ensuring that the analyses were robust and precise.
Instruments
Participants completed an online questionnaire consisting of the following instruments:
Motivos para Cesar o Reducir el Consumo de Alcohol (MCR-A) (Reasons to Stop/Reduce Alcohol Consumption). Developed by Conde et al. (2016), this instrument assesses two dimensions: reasons for stopping and reasons for reducing alcohol consumption. Each dimension consists of 20 items distributed across three factors: F1. Rejection of alcohol; F2. Health and life Changes; and F3. Severe consequences. Items are rated on a three-point scale: 0 (none), 1 (a little) and 2 (a lot).
Modified Drinking Motives Questionnaire-Revised (MDMQ-R). Developed by Grant et al. (2007), this instrument assesses motives for alcohol consumption. It consists of 28 items distributed across five factors: F1. Social; F2. Coping-Anxiety; F3. Coping-Depression; F4. Enhancement; and F5. Conformity. Items are rated on a five-point Likert scale ranging from 1 (almost never/never) to 5 (almost always/always). The version used in this study was validated by Sousa et al. (2024) with Brazilian university students and demonstrated good model fit (TLI = .97; CFI = .97; RMSEA (90% CI) = .078 (.073 - .084)), and excellent reliability (α = .94; ω = .94).
Sociodemographic Questionnaire. Developed to characterize the sample, addressing the participants’ age, sex, marital status, religion, and alcohol consumption.
Procedures
The first stage of the study involved the cross-cultural adaptation of the Reasons for Stop/Reduce Alcohol Consumption (MCR-A) scale for the Brazilian context. Initially, permission was requested from the instrument’s original authors for its use in Brazil. The adaptation process followed the methodological guidelines proposed by Borsa et al. (2012). Two bilingual translators independently translated the instrument from Argentine Spanish into Brazilian Portuguese, and their translations were reviewed and reconciled. Two experts in psychometrics and the target construct evaluated the reconciled version.
The next stage involved testing the instrument with 20 university students who were not part of the main sample. The goal was to assess item clarity through semantic evaluation. No semantic changes were deemed necessary. Two independent translators who had no access to the original version back-translated the instrument into Spanish, ensuring both conceptual and linguistic equivalence.
Finally, the instruments were organized and made available through LimeSurvey software for remote data collection. Participation in the survey was promoted via social media (WhatsApp, Instagram, and email), providing information about the study, participation criteria, and access to the questionnaires through the link (http://e.usp.br/pdq). Upon accessing the link, participants were directed to a page containing the informed consent form, which explained the study objectives and ensured anonymity and confidentiality. Participants were required to provide electronic consent in order to access the survey.
Those who provided their consent proceeded to complete the instrument items. The study was approved by the Institutional Review Board of FFCLRP/USP (Opinion No. 5,719,095; CAAE: 62718222.4.0000.5407) and complied with the ethical guidelines established by the National Health Council (Resolutions No. 466/12 and No. 510/16), including those specific to online research (Circular Letter No. 2/2021/CONEP/SECNS/MS).
Data analysis
Data were downloaded into a Microsoft Excel spreadsheet and then exported to the open-access statistical software JASP version 0.19.3 (University of Amsterdam, https://jasp-stats.org/) for analysis. Descriptive analyses were first conducted to characterize the study participants, followed by a Confirmatory Factor Analysis (CFA) to test the proposed structure of the MCR-A scale in the Brazilian sample. The reliability of the instrument was assessed using Cronbach’s alpha and McDonald’s omega.
CFA was conducted using the Diagonally Weighted Least Squares (DWLS) estimation method, which is appropriate for ordinal categorical data (Li, 2016). The following goodness-of-fit indices were used: Comparative Fit Index (CFI ≥ .95), Tucker-Lewis Index (TLI ≥ .95), and Root Mean Square Error of Approximation (RMSEA < .08; Hu & Bentler, 1999). Factor loadings above .40 were considered satisfactory (Castro et al., 2013). Cronbach’s alpha and McDonald’s omega values equal to or greater than .70 were considered acceptable for reliability (Cervin et al., 2022).
Results
The structure of the tested instrument showed good fit indicators. For the scale measuring reasons to stop alcohol consumption, the indices were: TLI = .99; CFI = .99; RMSEA (90% CI) = .074 (.066 - .082). For the scale measuring reasons to reduce alcohol consumption, the indices were: TLI = .99; CFI = 0.99; RMSEA (90% CI) = .076 (.068 - .084).
The factor loadings for the items and their respective factors on the scale of reasons to stop alcohol consumption are presented in Table 1. All lambda coefficients (λ) were above .40. Item 06 (“Because of the price of alcoholic beverages”) showed the lowest loading (λ = .60), while item 14 (“Because I notice positive differences in myself when I am not under the influence of alcohol”) had the highest (λ = .89). The table also displays the covariances among the model’s factors.
Table 1: Standardized factor loadings and covariances between the factors of reasons for stopping alcohol consumption
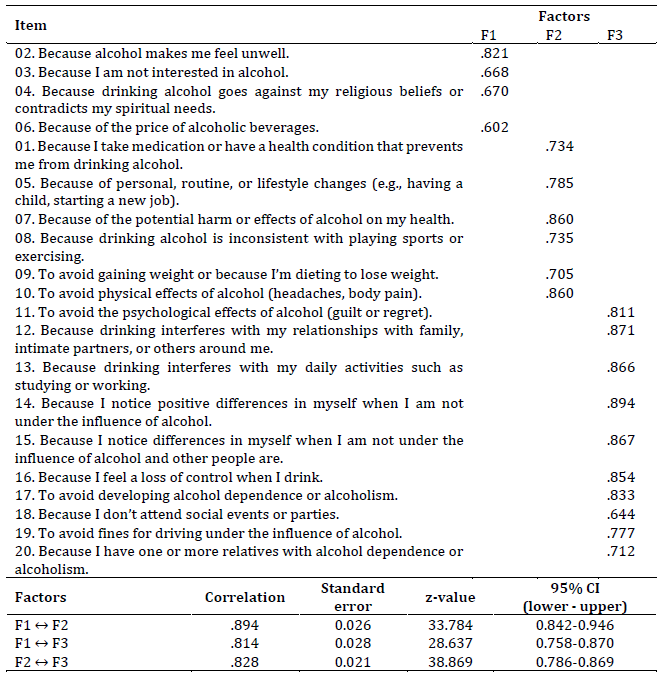
Note: All factor loadings and covariances are statistically significant (p < .001). F1: Rejection of alcohol; F2: Health and life changes; F3: Severe consequences.
For the scale of reasons to reduce alcohol consumption, the factor loadings were also greater than .40. Item 06 (“Because of the price of alcoholic beverages”) had the lowest loading (λ = .66), while item 14 (“Because I notice positive differences in myself when I am not under the influence of alcohol”) had the highest loading (λ = .94). Table 2 displays the lambdas (λ) coefficients of the items and their respective factors, as well as the estimates of the associations between the latent factors.
Table 2: Standardized factor loadings and covariances between the factors of reasons to reduce alcohol consumption
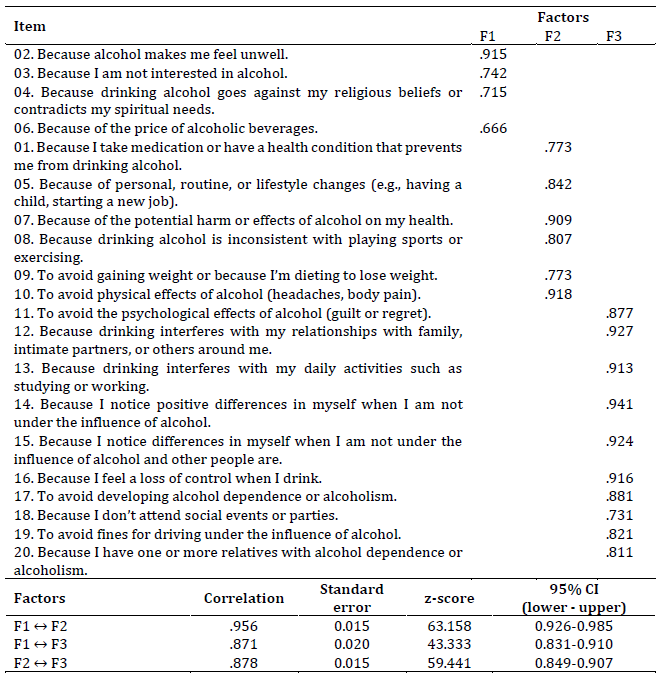
Note: All factor loadings and covariances are statistically significant (p < .001). F1: Rejection of alcohol; F2: Health and life changes; F3: Severe consequences.
Next, reliability was assessed using Cronbach’s alpha (α) and McDonald’s omega (ω) coefficients. These indices were calculated for both the unidimensional structure of the scales and their respective factors. Table 3 presents the coefficients for the two scales: reasons to stop alcohol consumption and reasons to reduce alcohol consumption.

Finally, to gather additional evidence of the measure's validity, a correlation analysis was conducted between the MCR-A total score and the MDMQ-R score. The results showed weak and statistically non-significant associations between the MCR-A and the MDMQ-R: reasons to stop (ρ = -0.100; p > .05) and reasons to reduce alcohol consumption (ρ = -0.081; p > .05).
Discussion
This study aimed to provide empirical evidence of the validity and reliability of the Brazilian version of the Reasons for Stop/Reduce Alcohol Consumption (MCR-A), originally developed in Argentina and adapted into Brazilian Portuguese as Motivos para Cessar e Reduzir o Consumo de Álcool (MCR-A). The hypothesis (H1) was that the scale would retain its three-factor structure for both reasons to stop and reduce alcohol consumption.
The results support hypothesis (H1), demonstrating that the factor structure of the MCR-A is empirically sound, as indicated by goodness-of-fit indices for the three-factor model (Hu & Bentler, 1999). These findings are consistent with the original Argentine study, suggesting that the three-factor model provides the best fit to the data (Conde et al., 2016).
Twenty items were tested for each construct (reasons to stop and reasons to reduce alcohol consumption) in the validation of the MCR-A by Conde et al. (2016); however, the item “Because of the price of alcoholic beverages” did not show adequate factor loadings for either construct. Similarly, the item “Because I take medication or have a health condition that prevents me from drinking alcohol” failed to show an adequate loading for the construct “reasons to reduce alcohol consumption.” Although these items exhibited the lowest factor loadings in this study, their saturations remained above 0.40 (Castro et al., 2013); therefore, they were retained due to their theoretical relevance and empirical adequacy in our sample.
Adaptation, validity, and reliability studies of psychological instruments in different contexts can result in variations in findings (Borsa et al., 2012). Such technical particularities can be attributed to sampling characteristics, which reflect the cultural specificities of each group studied. Therefore, empirical verification of technical indicators obtained with scales in different sociocultural contexts is crucial to advancing the field of knowledge (Sousa et al., 2020).
The literature acknowledges that the price of alcoholic beverages is a factor that can influence reduced consumption (Holmes, 2023; Santos et al., 2023), while young individuals frequently cite health issues as a significant reason for reducing alcohol use (Doyle, 2022). Given the theoretical importance of these items, the fit and reliability results of the MCR-A support their inclusion in the scale. It is worth noting that goodness-of-fit indices should be interpreted in conjunction with the theoretical robustness of the constructs (Castro et al., 2013).
The internal consistency of the MCR-A, measured by Cronbach’s alpha and McDonald’s omega, was adequate, with values exceeding the threshold recommended in the literature (≥ 0.70; Cervin et al., 2022). The use of McDonald’s omega as a complementary measure is justified by its greater robustness, as alpha is influenced by the number of items in a scale (Souza et al., 2017). These findings confirm that the MCR-A is a reliable instrument for assessing reasons to reduce and stop alcohol consumption in Brazil.
Furthermore, discriminant validity was assessed by correlating the general factor of the MCR-A with the Modified Drinking Motives Questionnaire-Revised (MDMQ-R). The weak and statistically non-significant correlations provide evidence of discriminant validity between the measures, indicating that they assess distinct constructs (Venâncio, 2021). These findings support the use of both instruments as complementary approaches to investigating motivations related to alcohol consumption among university students.
Understanding the reasons most frequently cited for reducing or stopping alcohol use among specific groups, as identified through the MCR-A, enables the development of effective and sensitive behavior change strategies, thereby increasing the impact of interventions. In the realm of public policy, this knowledge can inform the design of alcohol prevention and reduction programs within health services, particularly in primary care settings.
The World Health Organization (WHO, 2019), in collaboration with international partners, launched the SAFER initiative (Strengthen, Advance, Facilitate, Enforce, Raise) to support governments in reducing the harmful use of alcohol and its associated health and socioeconomic impacts. Although the initiative considers contextual variables in addressing this public health issue, one of its key actions is to enhance strategies for the rapid identification and treatment of excessive alcohol consumption, particularly among young people. In this context, identifying factors associated with the cessation and reduction of alcohol use among university students - through the use of a validated instrument such as the MCR-A - can assist professionals in recognizing relevant variables for planning both educational and clinical interventions, thereby helping to prevent further harm to this population’s development.
Final Considerations
This study evaluated the factorial structure of the MCR-A within the Brazilian sociocultural context, demonstrating that the instrument possesses adequate psychometric properties, including validity and reliability. These findings suggest that the MCR-A is a suitable tool for assessing motivations to reduce and stop alcohol consumption among university students.
However, this study has some limitations. First, the use of a convenience sample limits the generalizability of the findings. Second, data were collected through self-report instruments, which may be subject to social desirability bias. Finally, the cross-sectional and correlational design of the study restricts the ability to establish causal relationships.
Future research should consider using larger samples that ensure balanced representation from different Brazilian regions to test the consistency and replicability of the MCR-A across diverse cultural contexts. Additionally, it is important to investigate other types of validity, such as convergent and criterion-related validity (concurrent or predictive), to provide a more comprehensive evaluation of the instrument.
This study is the first to evaluate the psychometric properties of the MCR-A in Brazil, employing robust statistical techniques - an aspect that underscores both its strength and originality. While the results demonstrated solid psychometric qualities, further research is encouraged to deepen understanding of these constructs among Brazilian university students and to continue advancing knowledge in this field.

